
基于CT测定的细胞外体积分数对结肠腺癌术前病理分级的预测价值
2024-04-30 05:12:33王庆慧高飞王锡明
中国中西医结合影像学杂志 2024年2期
王庆慧 高飞 王锡明
[摘要] 目的:探讨CT测定的细胞外体积分数(ECV)预测结肠腺癌病理分级可行性。方法:选取经手术病理证实的结肠腺癌患者380例,术前均行腹部多期动态CT增强扫描。结肠癌病灶的ECV通过平扫和平衡期图像在ROI测量计算。根据病理分级将患者分为高级别组100例和低级别组280例,比较2组影像特征及临床特征。ECV与结肠腺癌病理分级的相关性行二元logistic回归分析。采用ROC曲线评价ECV对结肠腺癌病理分级的诊断效能。结果:多因素logistic回归分析显示,ECV是结肠腺癌病理分级的独立预测因子,OR值为1.380(95%CI 1.289~1.477)。ROC曲线显示:ECV对结肠腺癌病理分级的诊断效能较好,AUC为0.898(95%CI 0.851~0.947),敏感度为90.0%,特异度为91.4%。结论:基于CT测定的ECV有助于预测结肠腺癌的病理分级,且对个体化治疗具有一定意义。
[关键词] 结肠癌;细胞外体积分数;体层摄影术,X线计算机;病理分级
Predictive value of the extracellular volume fraction based on CT in the preoperative pathological grading of colon adenocarcinoma
[Abstract] Objective:To investigate the feasibility of the extracellular volume fraction (ECV) determined using CT to predict the pathologic grade of colon adenocarcinoma. Methods:A total of 380 patients with pathologically proven colon adenocarcinoma were selected. Pre-operative multi-phase dynamic enhanced CT scans were conducted for all patients. The ECVs of colon cancer lesions were calculated using ROI measurements on unenhanced and equilibrium-phase CT images. According to pathological grade,the patients were divided into a high-grade group (100 patients) and a low-grade group (280 patients). The imaging features and clinical data between the two groups were compared. The correlation between ECV and the pathological grade of colon adenocarcinoma was analyzed with binary logistic regression. ROC curve was used to evaluate the diagnostic efficiency. Results:The multi-factor logistic regression analysis showed that ECV was an independent predictor for the pathological grade of colon adenocarcinoma,with OR of 1.380(95%CI 1.289~1.477). The ROC curve demonstrated that ECV had better diagnostic accuracy in predicting the pathologic grade of colon adenocarcinoma,with the AUC of 0.898(95%CI 0.851~0.947),the sensitivity of 90.0% and the specificity of 91.4%. Conclusion:The ECV determined using enhanced CT is helpful for predicting the pathological grade of colon adenocarcinoma and may contribute to personalized treatment.
[Key words] Colon cancer;Extracellular volume fraction;Tomography,X-ray computed;Pathologic grade
結肠癌是临床常见且致死率较高的恶性肿瘤之一[1],其中结肠腺癌最常见,约占结肠癌的90%以上[2]。研究表明,结肠腺癌的分化程度是影响预后的重要因素[3]。WHO消化系统肿瘤分类第五版将结肠腺癌分为高级别和低级别2种类型[4]。高级别结肠腺癌在肿瘤切除术后复发的风险较高,预后较差[5]。细胞外体积分数(extracellular volume fraction,ECV)是血管外细胞体积分数与血管内空间分数之和,能反映微血管密度和基质纤维化程度,充分反映肿瘤微环境[6]。Takumi等[7]证实CT上ECV越高,胸腺上皮肿瘤的分化程度越低。Adams等[8]发现,通过MRI确定的ECV可准确预测高、低级别肾透明细胞癌,但目前临床很少将其应用于结肠腺癌的病理分级评价。因此,本研究旨在探讨基于CT测量的ECV对结肠腺癌术前病理分级的预测价值。
1 资料与方法
1.1 一般资料
回顾性分析2019年6月至2023年6月于山东省立医院经手术病理学证实的结肠腺癌患者380例,男240例,女140例;年龄17~87岁,平均(60.9±11.6)岁。其中高级别组100例,男61例,女39例,平均年龄(61.7±11.3)岁;低级别组280例,男179例,女101例,平均年龄(60.6±11.8)岁。术前均行腹部CT增强扫描。收集患者的临床资料,包括腹痛腹胀、便血、肠梗阻、腹部包块、便秘、大便性状的改变情况及血细胞比容值。本研究经山东省立医院伦理委员会批准,并放弃书面知情同意。纳入标准:①均经术后病理证实为结肠腺癌;②术前均行常规腹部CT增强扫描;③临床资料及生化检查信息完整。排除标准:①术前行新辅助化疗;②图像未见肿瘤;③图像质量差;④合并其他恶性肿瘤。
1.2 仪器与方法
所有患者均行全腹部常规CT平扫及增强扫描。采用Somatom Force CT扫描仪,扫描前禁食6~8 h,扫描范围从膈肌顶部至耻骨联合下缘。扫描参数:120 kV,250~400 mA(自动管电流调节技术),旋转时间0.5 s,探测器准直0.625 mm,矩阵512×512,螺距1.0。对比剂采用碘海醇,剂量1.5 mL/kg体质量,注射流率 3~4 mL/s,于注射后30、60、180 s行动脉期、静脉期、平衡期扫描。
1.3 图像分析
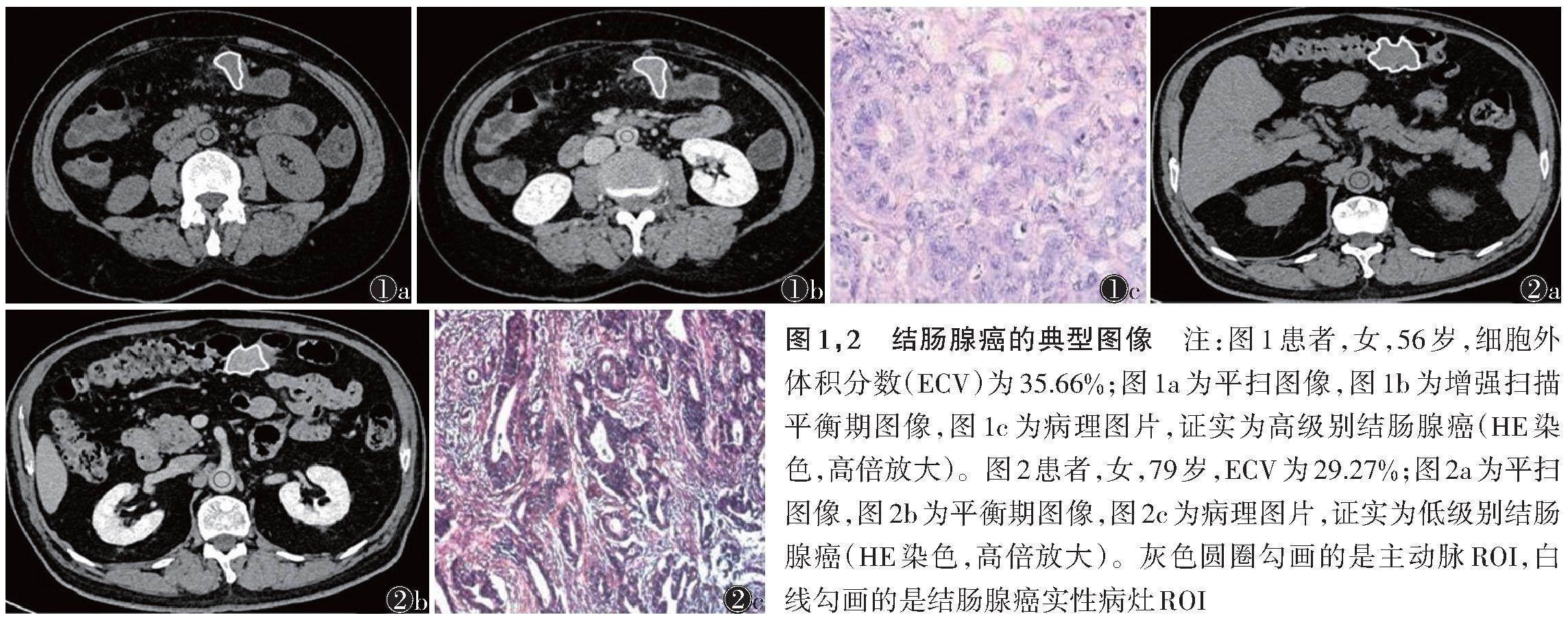
将数据传送至PACS工作站,行图像后处理,获得冠状位、矢状位MPR,必要时重组VR图像。所有图像均由2位放射科医师双盲阅片,观察肿瘤的大小(<5/≥5 cm)、边界(肠壁增厚/肠腔肿块)、周围脂肪间隙(清晰/模糊)、腹部肿大淋巴结(短径>1 cm)等,意见不统一时,经讨论取得一致。选取病灶最大层面,分别在平扫、平衡期手动绘制ROI,并测量结肠癌实性病灶及同层面主动脉的CT值,测量3次,取平均值(图1,2)。注意勾画ROI时避开坏死、囊变、钙化及出血部位。ECV计算公式如下:ECV(%)=(1-血细胞比容)×(ΔHU肿瘤/ΔHU主动脉)×100%。其中ΔHU肿瘤是病灶实性部分平衡期CT值减去相应平扫CT值,ΔHU主动脉是主动脉平衡期CT值减去相应平扫CT值。
1.4 统计学分析
采用SPSS 26.0统计软件。计量资料采用Shapiro-
Wilk法行正态分布检验。正态分布、方差均匀数据的组间比较采用独立样本t检验;否则采用Mann-Whitney U检验。变量组间比较行χ2检验。采用单因素和多因素logistic回归分析确定ECV与结肠腺癌病理分级的相关性。采用ROC曲线评价ECV对结肠腺癌病理分级的诊断效能。以P<0.05为差异有统计学意义。
2 结果
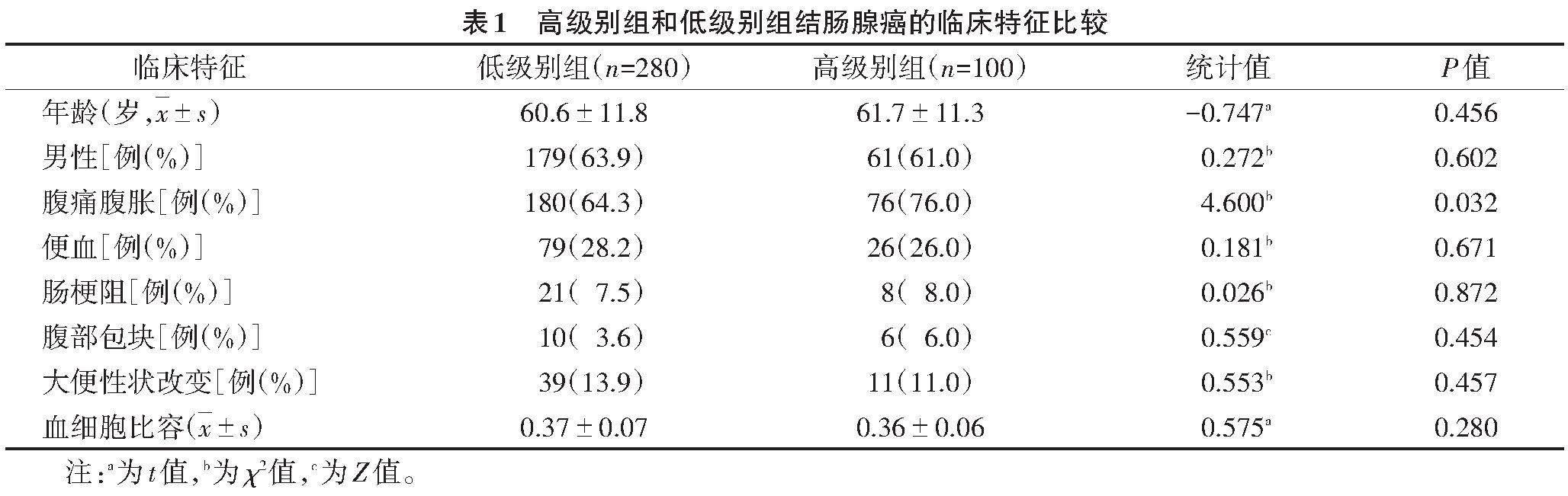
2.1 2组临床特征比较(表1)
高级别组腹痛腹胀的发生率高于低级别组,差异有统计学意义(P<0.05)。2组年龄、性别、便血、肠梗阻、腹部包块、大便性状改变及血细胞比容的发生率差异均无统计学意义(均P>0.05)。
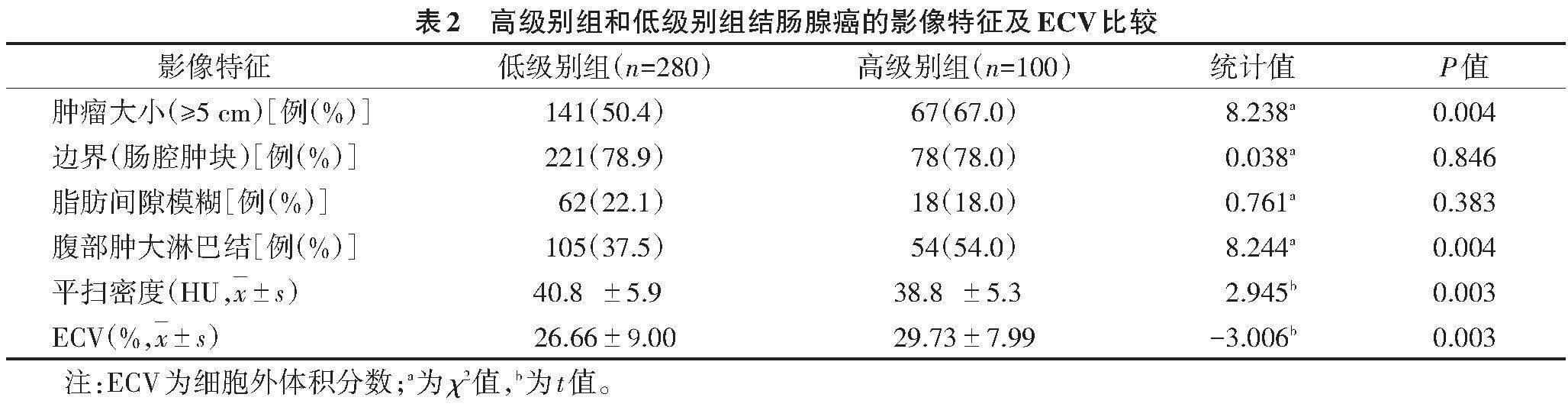
2.2 2组影像特征及ECV比较(表2)
高级别组平扫密度低于低级别组,≥5 cm肿瘤及腹部肿大淋巴结的发生率高于低级别组,差异均有统计学意义(均P<0.05)。2组肿瘤边界为肠腔肿块型、腹部脂肪间隙模糊的发生率差异均无统计学意义(均P>0.05)。
2.3 单因素和多因素logistic回归分析(表3)
单因素logistic回归分析示,ECV与结肠腺癌病理分级密切相关。高级别组ECV是低级别组的1.39倍。将单因素logistic分析中有统计学意义的参数,即ECV、腹痛腹胀、肿瘤大小、腹部肿大淋巴结、平扫密度,行多因素logistic回归分析,结果表明ECV是结肠腺癌病理分级的独立预测因子(P<0.001)。
2.4 ECV诊断结肠腺癌病理分级的ROC曲线(图3)
ECV评估结肠腺癌病理分级的AUC为0.898(95%CI 0.851~0.947),敏感度和特异度分别为90.0%、91.4%。
3 讨论
病理分级是结肠癌的独立预后因素,结肠腺癌患者的5年生存率与肿瘤分期、分级密切相关,分期、分级越高,预后越差[9]。不同病理分级,可能需要不同的治疗方法[10-13]。治疗前区分高、低级别结肠腺癌,识别复发高危患者,对实施个体化治疗、提高疗效至关重要[14]。结肠镜活检通常用于结直肠癌的诊断,可提供肿瘤分级的部分信息,但其具有出血、结肠穿孔和腹痛等不足[15-16]。此外,活检也存在定位不佳、瘤内异质性、样本质量差等缺点。MRI费用较高,在临床中的应用较CT少。CT已被常规应用于结肠癌患者的术前分期[17-19]。Huang等[14]开发了一种基于CT的放射组学模型来区分高、低级别结肠癌;该模型在训练数据集和验证数据集上均表现出良好的识别能力。双能谱CT虽能定量分析结肠癌的分化程度[20],但辐射剂量较大。
ECV在临床中应用广泛,通过CT或MRI确定的ECV与病理性纤维化体积相关,ECV已被很好地应用于心臟和肝脏纤维化的评估[21-22]。Fukukura等[23]报道通过CT增强扫描测定的肿瘤ECV是一种有价值的影像学生物标志物,可预测胰腺癌患者化疗后的生存率。然而,很少有关于ECV与结肠腺癌病理分级关系的研究。因此,本研究应用基于CT测定的ECV来鉴别高、低级别结肠腺癌,通过单因素和多因素logistic回归分析,证明ECV是结肠腺癌病理分级的独立预测因子,AUC为0.898,敏感度、特异度分别为90.0%、91.4%,具有较好的诊断效能。
基于CT的ECV測定具有以下优点:①相对于组织学检查,ECV无创、易于测定且能避免组织学检查带来的并发症;②与MRI相比,CT扫描速度快,空间分辨力高,可评估MRI禁忌证的患者,如体内有金属植入、幽闭恐惧症等;③与双能谱CT比较,基于常规CT的ECV辐射剂量小、临床应用广泛。
本研究中,腹痛腹胀多见于高级别结肠腺癌,原因可能是高级别结肠腺癌较低级别肿瘤周围微环境更易发生变化,造成血管和神经的浸润,从而引发腹痛腹胀。高级别结肠腺癌肿瘤大小常≥5 cm,多伴腹部淋巴结肿大;肿瘤分化程度低,更易发生淋巴结转移[24];较低级别肿瘤平扫密度低,可能与肿瘤恶性程度高、生长速度快、易发生坏死囊变有关。
本研究存在的不足:为回顾性研究,存在选择偏倚;样本量较小,尤其是高级别结肠腺癌,需加大样本量进一步研究;测量平扫与增强扫描CT值时存在人工误差。
综上所述,基于CT测定的ECV是结肠腺癌病理分级的独立预测因子,具有良好的诊断效能,且无创、便于临床推广,可为结肠癌患者的个体治疗提供依据。
[参考文献]
[1] SIEGEL R L,MILLER K D,WAGLE N S,et al. Cancer statistics,2023[J]. CA Cancer J Clin,2023,73(1):17-48.
[2] FLEMING M,RAVUlA S,TATISHCHEV S F,et al.
Colorectal carcinoma:pathologic aspects[J]. J Gastrointest Oncol,2012,3(3):153-173.
[3] VASILE L,OLARU A,MUNTEANU M,et al. Prognosis
of colorectal cancer:clinical,pathological and therapeutic correlation[J]. Rom J Morphol Embryol,2012,539(2):383-391.
[4] NAGTEGAAL I D,ODZE R D,KLIMSTRA D,et al.
The 2019 WHO classification of tumours of the digestive system[J]. Histopathology,2020,76(2):182-188.
[5] BOCKELMAN C,ENGELMANN B E,KAPRIO T,et al. Risk of recurrence in pa-tients with colon cancer stage Ⅱ and Ⅲ:a systematic review and meta-analysis of recent literature[J]. Acta Oncol,2015,54(1):5-16.
[6] ZHOU Z,WANG R,WANG H,et al. Myocardial extracellular volume fraction quantification in an animal model of the doxorubicin-induced myocardial fibrosis:a synthetic hematocrit method using 3T cardiac magnetic resonance[J]. Quant Imaging Med Surg,2021,11(2):510-520.
[7] TAKUMI K,NAGANO H,MYOGASAKO T,et al. Feasibility of iodine concentration and extracellular volume fraction measurement derived from the equilibrium phase dual-energy CT for differentiating thymic epithelial tumors[J]. Jpn J Radiol,2023,41(1):45-53.
[8] ADAMS L C,JURMEISTER P,RALLA B,et al. Assessment of the extracellular volume fraction for the grading of clear cell renal cell carcinoma:first results and histopathological findings[J]. Eur Radiol,2019,29(11):5832-5843.
[9] BARRESI V,REGGIANI BONETTI L,IENI A,et al.
Histological grading in colorectal cancer:new insights
and perspectives[J]. Histol Histopathol,2015,30(9):1059-1067.
[10] CHEONG C K,NISTALA K R Y,NG C H,et al. Neoadjuvant therapy in locally advanced colon cancer:a meta-analysis and systematic review[J]. J Gastrointest Oncol,2020,11(5):847-857.
[11] DE GOOYER J M,VERSTEGEN M G,'T LAM-BOER J,et al. Neoadjuvant chemotherapy for locally advanced T4 colon cancer:a nationwide propensity-score matched cohort snalysis[J]. Dig Surg,2020,37(4):292-301.
[12] PELLINO G,WARREN O,MILLS S,et al. Comparison of western and Asian guidelines concerning the management of colon cancer[J]. Dis Colon Rectum,2018,61(2):250-259.
[13] HASHIGUCHI Y,MURO K,SAITO Y,et al. Japanese
Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer[J]. Int J Clin Oncol,2020,25(1):1-42.
[14] HUANG X,CHENG Z,HUANG Y,et al. CT-based radiomics signature to discriminate high-grade from low-grade colorectal adenocarcinoma[J]. Acad Radiol,2018,25(10):1285-1297.
[15] VIIALA C H,ZIMMERMAN M,CULLEN D J,et al.
Complication rates of colonoscopy in an Australian
teaching hospital environment[J]. Intern Med J,2003,33(8):355-359.
[16] SENORE C,EDELE A,FANTIN A,et al. Acceptability
and side-effects of colonoscopy and sigmoidoscopy in a screening setting[J]. J Med Screen,2011,18(3):128-134.
[17] 蔣华东,顾庆春,朱荣荣,等. MSCT对结肠癌术前诊断及分期的临床价值[J]. 中国中西医结合影像学杂志,2016,14(1):31-33.
[18] 赵庆,金艳. MSCT在评估结肠癌侵犯程度的价值[J].医学影像学杂志,2019,29(7):1159-1162.
[19] LEUFKENS A M,VAN DEN BOSCH M A,VAN LEEU-
WEN M S,et al. Diagnostic accuracy of computed tomography for colon cancer staging:a systematic review[J].
Scand J Gastroenterol,2011,46(7-8):887-894.
[20] YANG C B,HE T P,DUAN H F,et al. Quantitative assessment of the degree of differentiation in colon cancer with dualenergy spectral CT[J]. Abdom Radiol (NY),2017,42(11):2591-2596.
[21] BANDULA S,WHITE S K,FLETT A S,et al. Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT:validation against histologic fndings[J]. Radiology,2013,269(2):396-403.
[22] LUETKENS J A,KLEIN S,TRABER F,et al. Quantifcation of liver fbrosis at T1 and T2 mapping with extracellular volume fraction MRI:preclinical results[J]. Radiology,2018,288(3):748-754.
[23] FUKUKURA Y,KUMAGAE Y,HIGASHI R,et al. Extracellular volume fraction determined by equilibrium contrast-enhanced multidetector computed tomogra-phy as a prognostic factor in unresectable pancreatic adenocarci-noma treated with chemotherapy[J]. Eur Radiol,2019,29(1):353-361.
[24] DERWINGER K,KODEDA K,BEXE-LINDSKOG E,et al. Tumour differentiation grade is associated with TNM staging and the risk of node metastasis in colorectal cancer[J]. Acta Oncol,2010,49(1):57-62.
猜你喜欢
中国医药科学(2016年13期)2017-02-06 20:53:51
中国实用医药(2016年29期)2016-12-26 10:14:12
华夏医学(2016年4期)2016-12-12 00:49:41
西南国防医药(2016年7期)2016-12-01 06:01:15
今日健康(2016年12期)2016-11-17 19:17:51
中国实用医药(2016年8期)2016-03-30 23:06:45
中国卫生标准管理(2015年1期)2016-01-14 03:41:26
中国实用医药(2016年2期)2016-01-05 09:28:26
河南医学研究(2014年3期)2014-02-27 14:51:48
河北医科大学学报(2011年4期)2011-03-25 10:16:13
