尿肾损伤分子-1在急性肾损伤诊断中的价值
2015-03-14 08:00:59江洁龙苏克亮袁园兰雷黄珍珍彭丽
中国临床保健杂志 2015年3期
江洁龙,苏克亮,袁园,兰雷,黄珍珍,彭丽
(安徽医科大学附属省立医院、安徽省立医院肾内科,合肥 230001)
·论著·
尿肾损伤分子-1在急性肾损伤诊断中的价值
江洁龙,苏克亮,袁园,兰雷,黄珍珍,彭丽
(安徽医科大学附属省立医院、安徽省立医院肾内科,合肥 230001)
[摘要]目的探讨尿肾损伤分子-1(Kim-1)检测在急性肾损伤(AKI)诊断中的价值。方法选择确诊的AKI患者71例作为AKI组,并选择同时期健康体检者30例为健康对照组,分别检测尿Kim-1及血肌酐(Scr)水平。结果AKI组Scr、尿Kim-1较健康对照组明显升高(P<0.01),与健康对照组比较,Scr、尿Kim-1在AKI 1期、2期、3期均明显升高(P<0.01),与AKI 1期比较,Scr、尿Kim-1在AKI 2期、3期均明显升高(P<0.01),与AKI 2期比较,Scr及尿Kim-1在AKI 3期均明显升高(P<0.01);尿Kim-1与Scr之间具有明显相关性(r=0.842,P<0.01);尿Kim-1 ROC曲线下面积为0.915。结论尿Kim-1在AKI患者中排泄升高,对AKI具有诊断价值,可能为诊断AKI的敏感指标。
[关键词]急性肾损伤;诊断技术,泌尿科;糖蛋白类
急性肾损伤(AKI)是一种由多种原因引起、以肾功能急剧恶化并导致肾脏无法排泄尿毒素和维持电解质和水的平衡为特点的发病率高、临床常见的综合征[1]。在急性损伤早期进行有效干预可以逆转该病进展[2]。因此,寻找早期诊断AKI的生物标记物并对该病早期诊断、早期治疗是目前研究的热点。国外已有研究表明[3-6],肾损伤分子-1(Kim-1)对急性肾损伤可能具有早期诊断价值。本文通过观察不同时期AKI患者及非AKI患者中尿Kim-1变化情况,评价尿Kim-1对AKI的早期诊断价值。
1对象与方法
1.1研究对象选择2011年1月至2012年12月在我院住院确诊的急性肾损伤患者71例作为AKI组(AKI 1期23例、AKI 2期25例、AKI 3期23例),其中男39例,女32例;年龄 19~76周岁,平均(43.7±14.0)岁。选择同时期我院体检中心健康体检者30例为健康对照组,均无急慢性肾脏病、高血压病、糖尿病及其他严重疾病,近期未服用肾毒性药物,其中男18例,女12例;年龄19~68周岁,平均(40.3±13.5)岁。AKI组及健康对照组患者年龄及性别均差异无统计学意义。
1.2纳入与排除标准纳入标准即为AKI诊断标准:参照2005年9月荷兰阿姆斯特丹国际急性肾损伤网络(AKIN)第一次会议急性肾损伤专家共识小组制定的AKI标准。排除标准:(1)住院时间小于24 h;(2)终末期肾脏病行维持性透析患者;(3)肾移植患者;(4)再次住院患者;(5)年龄小于18周岁。
1.3标本收集所有入选的研究对象均留取新鲜晨尿 10 mL,以 1000 r/min离心10 min后取上清液进行检测,同时留取血标本5 mL送检。
1.4主要仪器、试剂及检测方法采用的仪器为上海科华 KHB-ST-360酶标仪、日本日立HITACHI7600-020全自动生化分析仪。尿Kim-1采用酶联免疫吸附法(ELISA)检测,Kim-1试剂盒由上海信裕生物科技有限公司提供,实验方法按试剂盒说明书操作。
1.5统计学处理使用SPSS15.0软件进行数据分析,AKI组与健康对照组间比较采用t检验,AKI各分期组及健康对照组组间比较采用One-way ANOVA分析;绘制受试者工作特征(ROC)曲线并计算选择最佳的诊断界限值。计数资料组间比较采用χ2检验。
2结果
2.1健康对照组与AKI组各项指标水平比较见表1。

表1 健康对照组与AKI组各项指标水平比较±s)
注:与健康对照组比较,aP<0.01;与AKI 1期组比较,bP<0.01;与AKI 2期组比较,cP<0.01
2.2Kim-1与Scr相关性Kim-1与Scr相关系数为0.842,P<0.01,见图1。
2.3尿Kim-1 ROC曲线下面积及诊断点尿Kim-1的ROC曲线下面积(AUC)为0.915,95% 的可信区间为0.853~0.978,以73.58 μg/L 作为AKI的诊断界限时,敏感性和特异性分别为93.0%和83.3%,见图2。
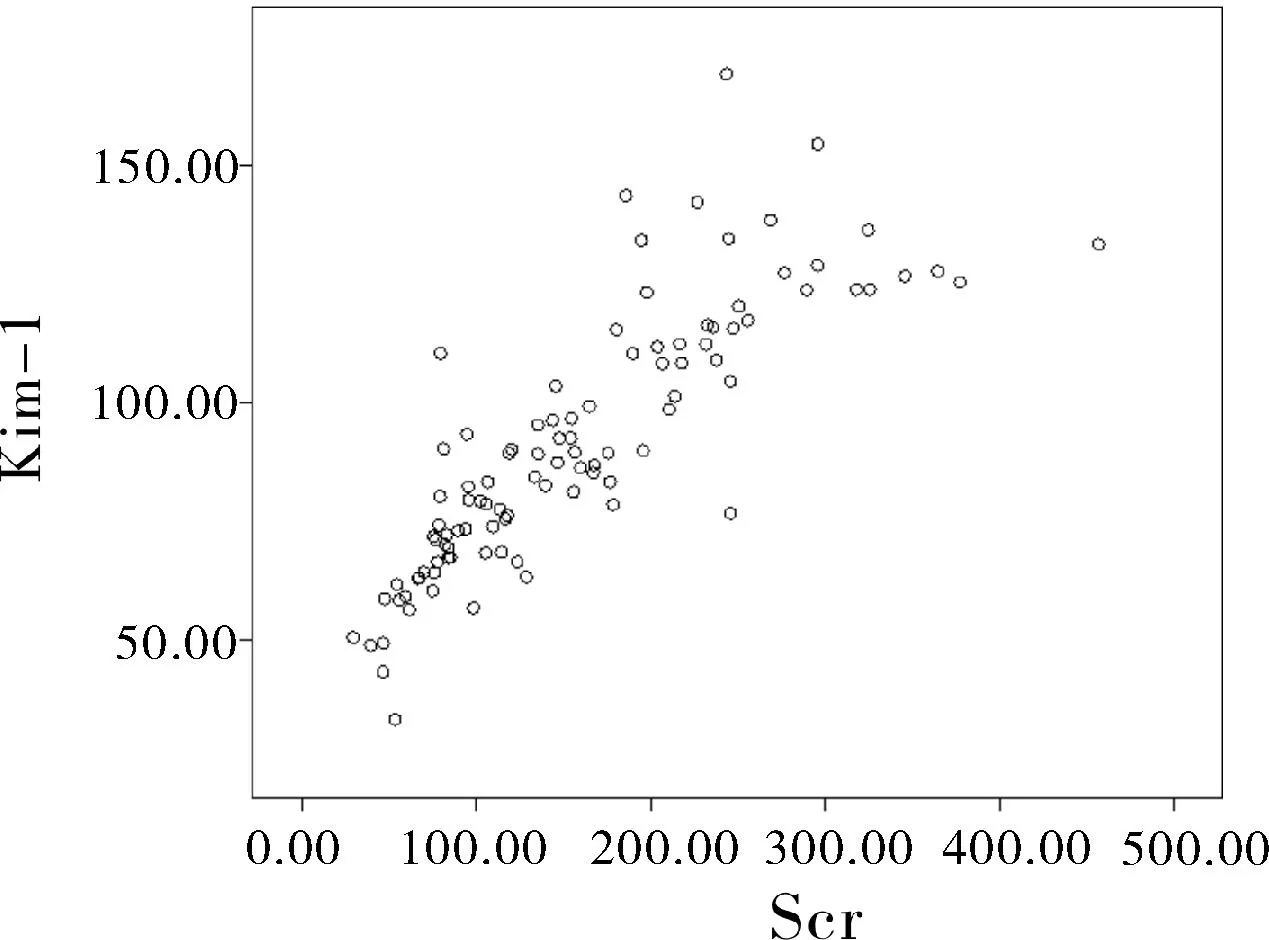
图1 尿与Scr相关性

图2 尿Kim-1 ROC曲线下面积及诊断点
3讨论
Kim-1是由肾脏近曲小管上皮细胞分泌一种跨膜1型糖蛋白,其中包含6-半胱氨酸域,属于免疫球蛋白基因超家族。它在正常肝、肾、脾组织中微量表达,而在受损后再生的近曲小管上皮细胞中表达明显增强。动物研究表明,Kim-1的外功能区断裂后产物能够通过尿中排出,因此检测尿中Kim-1水平可以间接评价肾脏损伤的情况,且已有研究表明,Kim-1对急性肾损伤具有早期诊断价值[7-10]。本研究发现,尿Kim-1在AKI组较健康对照组明显升高,且在AKI 1期、2期、3期逐渐升高,其两两相互比较差异均有统计学意义;尿Kim-1与Scr具有明显相关性(r=0.842,P<0.01);尿Kim-1的ROC AUC为0.915,以73.58 μg/L 作为AKI的诊断界限时,敏感性和特异性分别为93.0% 和83.3%,故尿Kim-1可能为诊断AKI的敏感指标。
同时,已有研究表明,目前常用的生物学标记物诊断AKI效能不同。Liangos等[11]比较了Kim-1、N-乙酰-β-D-氨基葡萄糖苷酶、中性粒细胞明胶酶相关脂质运载蛋白、白细胞介素-18、胱抑素C 、α1-微球蛋白等6种生物学标记物对AKI的诊断价值,发现Kim-1诊断AKI的AUC最大,为 0.78,其 95% 可信区间 0.64~0.91。
综上所述,尿Kim-1在AKI患者中明显升高,且在AKI不同分期患者中差异有统计学意义,结合其ROC AUC及诊断敏感性及特异性,其对AKI可能具有诊断价值。
参考文献
[1]Ricci Z,Cruz DN,Ronco C.Classification and staging of acute kidney injury:beyond the RIFLE and AKIN criteria[J].Nat Rev Nephrol,2011,7(4):201-208.
[2]Schrier RW,Wang W,Poole B,et al.Acute renal failure:definitions,diagnosis,pathogenesis,and therapy[J].J Clin Invest,2004,114(1):5-14.
[3]Tekce BK,Uyeturk U,Tekce H,et al.Does the kidney injury molecule-1 predict cisplatin-induced kidney injury in early stage?[DB/OL].Ann Clin Biochem,[2014-06-11].http://www.ncbi.nlm.nih.gov/pubmed/24670880.
[4]Hoste EA,Kellum J A.Acute kidney injury:epidemiology and diagnostic criteria[J].Curr Opin Crit Care,2006,12(6):531-537.
[5]Bellomo R,Ronco C,Kellum J A,et al.Acute renal failure-definition,outcome measures,animal models,fluid therapy and information technology needs:the Second International Consensus Conference of the Acute Dialysis Quality Initiative(ADQI)Group[J].Crit Care,2004,8(4):R204-R212.
[6]Long TE,Sigurdsson MI,Indridason OS,et al[Epidemiology of acute kidney injury in a tertiary care university hospital according to the RIFLE criteria [J].Laeknabladid,2013,99(11):499-503.
[7]Ichimura T,Asseldonk EJ,Humphreys BD,et al.Kidney injury molecule-1 is a phosphatidylserine receptor that confers a phagocytic phenotype on epithelial cells[J].J Clin Invest,2008,118(5):1657-1668.
[8]Bonventre JV.Kidney injury molecule-1(KIM-1):a urinary biomarker and much more[J].Nephrol Dial Transplant,2009,24(11):3265-3268.
[9]Han WK,Waikar SS,Johnson A,et al.Urinary biomarkers in the early diagnosis of acute kidney injury[J].Kidney Int,2008,73(7):863-869.
[10] Xue W,Xie Y,Wang Q,et al.Diagnostic performance of urinary kidney injury molecule-1(KIM-1)and neutrophil gelatinase-associated lipocalin(NGAL)for acute kidney injury in obstructive nephropathy patients[J].Nephrology(Carlton),2014,19(4):186-194.
[11] Liangos O,Tighiouart H,Perianayagam MC,et al.Comparative analysis of urinary biomarkers for early detection of acute kidney injury following cardiopulmonary bypass[J].Biomarkers,2009,14(6):423-431.
The diagnostic value of urinary Kim-1 detection in acute kidney injury
JiangJielong,SuKeliang,YuanYuan,LanLei,HuangZhenzhen,PengLi
(DepartmentofNephrology,AnhuiProvincialHospitalAffiliatedtoAnhuiMedicalUniversity,Hefei230001,China)
[Abstract]ObjectiveTo explore the diagnostic value of urinary Kidney injury molecule-1 (Kim-1) detection in patients with acute kidney injury (AKI). MethodSeventy-one patients with AKI were selected as the study group (AKI group), and 30 healthy individuals were enrolled as the control group. The levels of urinary Kim-1 and serum creatinine (Scr) were measured respectively.ResultsThe urinary Kim-1 and Scr were increased significantly (P<0.01) in AKI group when compared with the control group. The urinary Kim-1 and Scr increased significantly (P<0.01) in AKI stage 1, 2 and 3 in AKI group when compared with control group. The urinary Kim-1 and Scr were increased significantly (P<0.01) in AKI stage 2 and 3 when compared with stage 1. The urinary Kim-1 and Scr were increased significantly (P<0.01) in AKI stage 3 when compared with AKI stage 2. There was significant relationship between the urinary Kim-1 and Scr. The area under the receiver operating characteristics curve in the urinary Kim-1 was 0.915. ConclusionThe urinary Kim-1 excretion increases significantly in AKI group. It maybe has diagnostic value in AKI and used as a sensitive target diagnostic criteria for AKI.
[Key words]Acute kidney injury;Diagnostic techniques,urological;Glycoproteins
(收稿日期:2014-07-16)
Corresponding author:Su Keliang, Email:sukl8@163.com
中图分类号:R692.5
文献标识码:A
DOI:10.3969/J.issn.1672-6790.2015.03.008
通信作者:苏克亮,博士,副主任医师,Email:sukl8@163.com
作者简介:江洁龙,博士,主治医师,Email:jiangjl2013@126.com
基金项目:安徽省科技计划项目(10021403082)
猜你喜欢
中华养生保健(2020年10期)2021-01-18 06:45:30
中外医学研究(2016年32期)2017-02-27 01:48:34
现代仪器与医疗(2016年6期)2017-01-12 00:24:45
中国实用医药(2016年23期)2016-12-26 13:55:35
中国实用医药(2016年29期)2016-12-26 10:17:17
电子技术与软件工程(2016年20期)2016-12-21 10:36:10
科技创新与应用(2016年31期)2016-12-03 06:32:21
中国实用医药(2016年26期)2016-11-07 11:46:16
中国实用医药(2016年25期)2016-11-03 14:12:31
企业导报(2016年13期)2016-07-19 17:46:42