
Estimates of voluntary activation in individuals with anterior cruciate ligament reconstruction:Effects of type of stimulator,number of stimuli,and quantification technique
2022-03-24 02:36StevenGrciKzndrRodriguezScottBrownRinnPlmieriSmithChndrmouliKrishnn
Steven A.Grci,Kzndr M.Rodriguez,Scott R.Brown,Rinn M.Plmieri-Smith,c,Chndrmouli Krishnn,,d,*
a School of Kinesiology,University of Michigan,Ann Arbor,MI 48109,USA
b Neuromuscular and Rehabilitation Robotics Laboratory(NeuRRo Lab),Department of Physical Medicine and Rehabilitation,University of Michigan,Ann Arbor,MI 48108,USA
c Department of Orthopaedic Surgery,Michigan Medicine,University of Michigan,Ann Arbor,MI 48109,USA
d Robotics Institute,University of Michigan,Ann Arbor,MI 48109,USA
Abstract
Keywords: Anterior cruciate ligament;Central activation;Inhibition;Knee strength;Triplet;Twitch interpolation
1. Introduction
Quadriceps muscle weakness is a common byproduct of anterior cruciate ligament reconstruction (ACLR) and is reported to persist for several years after completing rehabilitation.1Persistent quadriceps weakness is problematic because it is associated with a host of suboptimal patient outcomes such as aberrant knee biomechanics,2,3increased risk of early-onset post-traumatic knee osteoarthritis,4,5and decreased knee health-related quality of life.1,6Accordingly, several studies have focused on understanding the mechanisms that may contribute to quadriceps weakness after ACLR.7-11 The results of these studies indicate that reduced quadriceps muscle voluntary activation(i.e.,the inability to drive the muscle maximally during a contraction)is a key factor for the immediate and persistent quadriceps weakness postoperatively.10-13
Voluntary activation is traditionally estimated in ACLR individuals using an electrical superimposition technique where a strong electrical stimulus(generally a 10-pulse train)is delivered to the quadriceps muscle while an individual is performing a maximal voluntary isometric contraction (MVIC).7,14,15In individuals who are unable to fully activate all available motor units or fire the motor units at a maximal rate,the superimposed electrical stimulus augments the muscle force/torque.16Expressing the maximal voluntary muscle torque generated before the delivery of the electrical stimulus relative to the maximally evoked torque following burst superimposition is commonly referred to as the central activation ratio(CAR)in Eq.(1):17-21

Voluntary activation can also be quantified using percent activation derived from the interpolated twitch technique(ITT)in which the delivery of a single,double,or train of 3 or more stimuli are commonly used,as has been described in the literature.22-28 The ITT is similar to the burst superimposition technique in that an electrical stimulus is provided to the muscle during an MVIC,but it also involves the application of an identical electrical stimulus when the muscle is at rest and potentiated (i.e., within a few seconds after MVIC).16The evoked torque during MVIC is then normalized to the evoked torque at rest to compute percent activation in Eq.(2):

The advantage of providing an additional stimulus at rest is that(1)it accounts for the inability of the electrical stimulus to evoke a true maximal muscle torque and(2)it ensures that the evoked torque during contraction is normalized to the torque elicited by the same stimulated muscles and not to synergistic muscles that may be contributing to torque produced during a volitional contraction.16,29,30Furthermore, the evoked torque at rest has been shown to provide additional insights into changes in peripheral muscle morphology, especially in individuals with ACLR.8,31Nonetheless,the burst superimposition technique remains the method of choice for estimating voluntary activation in ACLR participants,10,11,13,15,32-34 despite the fact that the CAR has been shown to overestimate voluntary activation in healthy participants.29,30,35Given that the overestimation using CAR has been shown to increase with an increase in activation deficit,29,30ITT may be a more sensitive and superior approach for estimating voluntary muscle activation in patient populations that are known to have significant voluntary activation deficits.
In addition to the quantification technique, the type of electrical stimulator (constant current vs. constant voltage)used during activation testing can affect the estimates of voluntary activation because of the differences in current intensity delivered during testing.16Constant current stimulators adjust the voltage in response to change in impedance (i.e.,skin/tissue resistance) to ensure that a constant current is delivered to the participant during testing. Conversely, constant voltage stimulators do not adjust the voltage in response to changes in impedance; thus, the current delivered to the participant will vary depending on the skin/tissue impedance observed during testing.However,it is unclear to what extent the type of stimulator used during activation testing affects the estimates of voluntary activation.This information is critical to compare results across studies that have used constant voltage2,9-11,13,36 and constant current7,8,37-39 stimulators or when choosing electrical stimulators for voluntary activation testing.
正常情况下,水利工程建设的施工场地都是现场情况比较复杂,这就很可能在施工过程中由于地质情况复杂而出现一些安全事故,这些事故的出现容易影响施工的正常进展,并且极有可能使工程的质量出现一定的问题。在水利工程进行施工的过程中出现安全事故的原因除了自然因素之外,还有可能因为人为的行为引发。这些人为因素主要有以下几个方面:施工过程中的监管不到位,施工所使用的测量设施落后,施工人员的安全意识不足,施工材料质量达不到施工要求便投入使用,施工设施不齐全加大施工难度等。[1]这些问题的出现都有可能使水利工程出现极为严重的安全问题,一旦安全事故发生,常常会使人员出现伤亡和施工单位出现经济损失。
The number of electrical pulses used during testing could also affect voluntary activation estimates16and have varied throughout the literature.7,10,40For example, single- and double-pulse electrical stimuli are known to result in inconsistencies or overestimations when quantifying voluntary activation because of the lesser evoked torque during contraction and/or at rest.35,40,41This factor is particularly problematic when using the CAR because the superimposed torque during contraction is not normalized to an evoked resting torque to account for differences in the strength of the electrical stimuli.Unfortunately,the effect of pulse train on voluntary activation estimates has mainly been studied in healthy individuals free of injury or neurologic deficits,35,40so less is known of these effects in individuals with ACLR. Furthermore, many studies in individuals with ACLR commonly report using a 3-pulse or 10-pulse train of electrical stimuli,7,15and it is unclear if voluntary activation estimates would differ when using a 3- or 10-pulse train.Thus,further research is needed to understand if differences in methodologic techniques (i.e., stimulator type and the number of pulses per train)affect estimates of volitional activation and resting torques in individuals with ACLR.
Therefore, the purpose of this study was to compare the effect of quantification technique (percent activation vs.CAR),electrical pulse train(3-pulse vs.10-pulse),and electrical stimulator type(Digitimer(constant current stimulator)vs.Grass (constant voltage stimulator)) on estimates of volitional quadriceps muscle activation in individuals with ACLR. We hypothesized that: (1) voluntary activation estimates obtained from the CAR would be significantly higher than those from ITT-based percent activation across both stimulators and electrical pulse train conditions, (2) CAR-based voluntary activation would differ between stimulators and pulse train conditions, and (3) voluntary activation estimates would significantly differ between the 2 stimulators.
2. Methods
2.1. Participants
Eighteen individuals with unilateral ACLR were recruited for this study. The participant characteristics and demographics are presented in Table 1. All participants provided written informed consent/assent before participation, and the study procedures were approved by the University of Michigan Medical School Institutional Review Board. Participants were included in this study if they were(1)at least 6 months and up to 5 years post-ACLR and (2) between the ages of 16 and 40 years. Participants were excluded if they reported any of the following:(1)more than 1 ACLR,(2)a history of injury or surgery to the ACLR knee or the contralateral, unaffected knee, (3) a history of significant anterior knee pain, (4) a history of recent fractures or surgery of the lower extremity, (5)pregnancy(in female participants),and(6)a history of uncontrolled diabetes, hypertension, or other significant cardiac or neurologic conditions.
Table 1 Participant characteristics and demographics(mean§SD).
2.2. Quadriceps strength and activation procedures
All participants completed quadriceps strength and activation testing on the reconstructed leg in a 2-h visit.After orienting the participant to the testing procedures,they were seated on an isokinetic dynamometer(Humac NORM;Computer Sports Medicine Inc.,Stoughton,MA,USA)with their knee and hip placed at 90˚ and 85˚,respectively.Their thigh,hip,and torso were secured to the chair according to the manufacturer’s instructions.The chair was adjusted to align each participant’s lateral femoral condyle with the axis of rotation of the dynamometer arm,and the distal torque pad was affixed to the shank at 2 finger widths above the medial malleolus. Before testing, alcohol pads were used to prepare the skin before applying 2 self-adhesive electrodes(2.75 inch£5.00 inch,Dura-Stick II;Chattanooga Group,Hixon,TN,USA)to the proximal vastus lateralis and distal vastus medialis muscles.After this procedure,participants completed a standardized warm-up protocol consisting of 2 submaximal trials at 50% and 75% of the participant’s perceived maximal effort and 1 practice MVIC trial with 1 min of rest between each trial.After a 2-min rest period, the participant performed 8 MVIC trials(with 2 min of rest between trials)during which voluntary quadriceps muscle activation was evaluated with different electrical stimulators and pulse train conditions (see below for details).During the MVIC trials, participants were instructed to kick out as hard and fast as possible with their hands crossed over their chest. Loud verbal encouragement and visual feedback of their torque curves were provided to facilitate maximal effort.
To test voluntary quadriceps muscle activation, 2 commonly used electrical stimulators (Digitimer DS7AH constant current stimulator (Digitimer Ltd., Hertfordshire, UK) and Grass S88 constant voltage stimulator (Grass-Telefactor; An Astro-Med Inc.,Warwick,RI,USA))and pulse trains(3-pulse and 10-pulse) were used.7-9,11,13,15,38,42 Participants were oriented to the pulse trains from both stimulators using several submaximal electrical stimuli (Digitimer: 50-180 mA and Grass: 30-90 V). The electrical stimuli during testing were delivered using an automated torque-triggering approach via a custom-written LabVIEW program (LabVIEW 11.0; National Instruments Corp., Austin, TX, USA).43Briefly, participants were shown a visual torque target that was determined based on a previously recorded MVIC.If a participant surpassed the torque target and plateaued (as determined by a torque drop of-1 N¢m), the LabVIEW program automatically triggered the electrical stimulator. Identical electrical stimuli were also provided immediately following the MVIC to obtain a potentiated evoked torque at rest. Two MVIC trials were performed for each condition(Digitimer 3-pulse,Digitimer 10-pulse,Grass 3-pulse, and Grass 10-pulse), and 2 min of rest was provided between each trial/condition. The order of testing for each of the 4 conditions was randomized before participant enrollment by first randomizing the device (Digitimer vs. Grass) and then randomizing the pulse train conditions (3-pulse vs. 10-pulse).The discomfort associated with the electrical stimuli (both at rest and during contraction) for each condition was evaluated using a visual analog scale (VAS) from 0 (no pain) to 10 (the worst imaginable pain). Stimulator settings (frequency, pulse width,and intensity)on the Digitimer and Grass were based on previous research and kept constant for all testing conditions(Digitimer: 100Hz, 200-ms pulse duration, 400V; Grass:100 Hz, 600-ms pulse duration, 135 V),2,9-11,13,15,29,34-36 except for differing pulse train conditions(i.e., 3-pulse and 10-pulse). The current intensities for activation testing with Digitimer were determined on a sex-specific basis based on previous work from Krishnan and Williams29(females: 290 mA,males:360mA). We noted that the Grass stimulator overloaded on 2 occasions(i.e.,the output circuit shut off for safety reasons).In these instances,we recleaned the anterior thigh where the stimulator electrodes were placed,reapplied the electrodes to reduce skin impedance,and then reset the Grass-unit MVIC trials were then repeated after adequate rest(i.e.,2 min).
2.3. Data management
The torque signals from the isokinetic dynamometer and the synchronization pulses from the electrical stimulators were sampled at 1000 Hz using a Dell Vostro 230 desktop with a 16-bit high-accuracy M-series data acquisition card (NI-USB-6251; National Instruments, Austin, TX, USA). The raw torque signals from the dynamometer were converted to torque values(N¢m)using calibrated equations determined before the testing. All data were low-passed filtered with a 0 phase-lag low-pass Butterworth digital filter (4th order, 10 Hz cut-off).Estimates of voluntary activation were computed using the CAR and percent activation methods as shown in Fig. 1. The average peak torque and activation estimates derived from the 2 MVIC trials were used in further analyses.
2.4. Statistical analyses
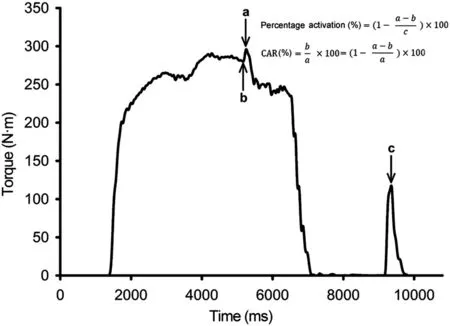
Fig. 1. Schematic showing the calculation of voluntary activation estimates using the percent activation and CAR. In the percent activation method derived from the interpolated twitch technique,voluntary activation is quantified by comparing the torque increment associated with the electrical stimulus during MVIC(“a -b”in the equation)to the torque generated by an identical electrical stimulus delivered when the muscle is at rest(evoked torque at rest;“c”in the equation). In the CAR method derived from the burst superimposition technique, voluntary activation is quantified by comparing the torque at the time of electrical stimulus during MVIC (“b” in the equation) to the total torque evoked by the electrical stimulus(“a”in the equation).Note that this is identical to comparing the torque increment associated with the electrical stimulus during MVIC(“a -b”in the equation)to the total torque evoked by the electrical stimulus (“a” in the equation). CAR=central activation ratio;MVIC=maximum voluntary isometric contraction.
All statistical analyses were performed using SPSS for Windows (Version 24.0; IBM Corp., Armonk, NY, USA).Descriptive statistics were computed for each variable. A one-way repeated measures analysis of variance (ANOVA)was used to evaluate whether the peak torque values produced during activation testing differed between the 4 conditions(Digitimer 3-pulse, Digitimer 10-pulse, Grass 3-pulse, and Grass 10-pulse).A three-way repeated measures ANOVA was used to evaluate whether the estimates of voluntary activation were affected by quantification technique (percent activation,CAR), type of stimulator (Digitimer, Grass), and pulse train(3-pulse, 10-pulse) used during testing. A significant interaction effect was followed by post hoc pairwise comparisons using paired t tests with a Bonferroni correction to adjust for multiple comparisons.A two-way repeated measures ANOVA was used to evaluate whether the evoked torque at rest differed between stimulators and pulse train conditions. The nonparametric Friedman test was used to compare the discomfort associated with the electrical stimulus (VAS score) between the resting and superimposed stimuli across pulse train conditions(3-pulse and 10-pulse) and stimulators (Digitimer and Grass)followed by post hoc analyses using the Wilcoxon signed-rank test. Additionally, Pearson’s product-moment correlation analyses were used to evaluate the associations between voluntary activation estimates derived from different quantification techniques(percent activation and CAR) and pulse train conditions(3-pulse and 10-pulse)using Digitimer and Grass stimulators. A significance level of a=0.05 was set for all statistical analyses.
3. Results
3.1. MVIC peak torque across conditions
There were no significant differences in MVIC peak torque values across conditions (F (3, 51)=1.059, partial h2=0.059,p=0.375;Table 2),indicating that any differences observed in voluntary activation estimates between conditions were not confounded by the differences in peak torque values produced during activation testing.
3.2. Voluntary activation estimates
Repeated measures ANOVA results revealed a significant effect of quantification technique (F (1, 17)=24.895, partial h2=0.594, p < 0.001) and train£quantification technique(F (1, 17)=7.693,partial h2=0.312, p=0.013) interaction on the estimates of voluntary activation. The main effect for quantification technique indicated that voluntary activation estimates were approximately 11.7% higher when using the CAR than the ITT-based percent activation (95% confidence interval (95%CI) mean difference: 6.734-16.603). Post hoc analyses of the interaction effect indicated that the estimates of voluntary activation differed significantly between pulse train conditions when using the CAR(3-pulse CAR:88.2%§2.4%,10-pulse CAR:86.4%§2.8%,p=0.003),but not when using the ITT-based percent activation(p=0.357).There were no significant main effects of stimulator (F (1, 17)=0.009,partial h2=0.001, p=0.924) or pulse train conditions(F (1, 17)=0.398, partial h2=0.023, p=0.536) on voluntary activation estimates. Similarly, no stimulator£train(F (1, 17)=0.738, partial h2=0.042, p=0.402), stimulator£quantification technique (F (1, 17)=2.690, partial h2=0.137, p=0.119), or stimulator£train£quantification technique (F (1, 17)=0.024, partial h2=0.001, p=0.879)interactions were observed.
3.3. Evoked torque at rest
Repeated measures ANOVA results revealed a significant main effect of stimulator (F (1, 17)=20.608, partial h2=0.548,p<0.001)and pulse train(F(1,17)=55.804,partial h2=0.766, p < 0.001) on the evoked torque at rest. The main effect for stimulator indicated that the Digitimer stimulator evoked approximately 10.1 N¢m greater evoked torque at rest than the Grass stimulator (95%CI mean difference:5.4-14.8).The main effect for train indicated that across stimulators the 10-pulse train evoked approximately 23.1 N¢m greater evoked torque at rest than the 3-pulse train (95%CImean difference: 16.6-29.7). There was no significant stimulator£train interaction effect on the evoked torque at rest(F(1,17)=0.737,partial h2=0.042,p=0.403).

Table 2 Estimates of quadriceps muscle voluntary activation, voluntary peak torque, and electrically evoked torque at rest across stimulators and pulse train conditions(mean§SD).
3.4. Relationship between voluntary activation estimates from various conditions
There were strong correlations between voluntary activation estimates derived from the CAR and ITT-based percent activation methods for both the stimulators (r=0.935-0.973,all p<0.001;Table 3 and Fig.2).There were also strong correlations between voluntary activation estimates derived from the 3-pulse and 10-pulse trains for both stimulators(r=0.962-0.981,all p<0.001;Table 3 and Fig.3).
3.5. Discomfort associated with electrical stimuli during testing
The Friedman test indicated a significant difference in VAS scores between various testing conditions (df=7,x2=102.034,p<0.001).Post hoc analyses indicated that the discomfort associated with electrical stimuli delivered at rest was greater than during maximal contraction across stimulators and pulse train conditions (all p < 0.001, Table 4). Similarly,the discomfort associated with 10-pulse electrical stimuli was greater than 3-pulse electrical stimuli(all p -0.05).This was particularly the case when the train of electrical stimuli was provided with the Digitimer stimulator(Table 4).
4. Discussion
The primary purpose of this study was to compare the effect of quantification technique (percent activation, CAR), pulse train condition (3-pulse, 10-pulse), and stimulator type (Digitimer, Grass) on the estimates of voluntary quadriceps muscle activation in individuals with ACLR. Additionally, we examined the relationship between voluntary activation estimates derived from the interpolated twitch (i.e., percent activation)and burst superimposition (i.e., CAR) techniques. The key findings of this study are that (1) voluntary activation wassignificantly overestimated by the CAR when compared with percent activation; (2) voluntary activation did not differ between pulse train conditions when using percent activation,although 3-pulse stimuli resulted in greater overestimation than 10-pulse stimuli when using CAR;(3)the type of electrical stimulator did not affect the estimates of voluntary activation, although the strength of the electrical stimuli (as determined by the evoked torque at rest) was greater when using the Digitimer than when using the Grass stimulator;and(4) the estimates of voluntary activation derived from the 2 quantification techniques were strongly associated.
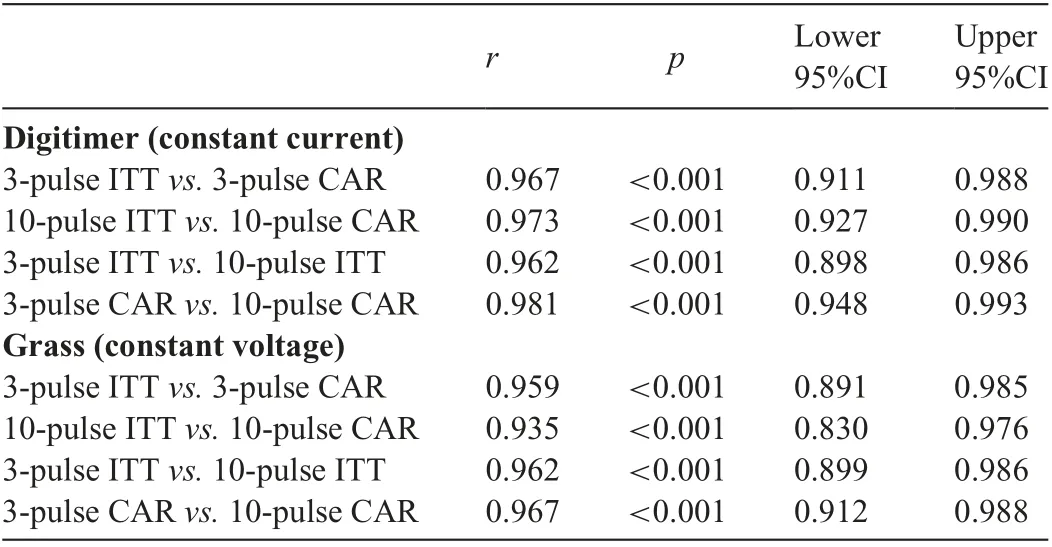
Table 3 Correlation coefficients describing the strength of association between voluntary activation estimates obtained from different quantification techniques and pulse train conditions using Digitimer and Grass stimulators.
Accurately quantifying voluntary activation deficits in individuals with ACLR is important to understanding the extent of quadriceps dysfunction. Previous studies have used the CAR and ITT-based percent activation to quantify voluntary activation in individuals with ACLR,2,7,9-11,13-15,34,36,38,44,45 but there are no studies that have directly compared each technique in an ACLR population.This information is key to accurately compare results across studies,especially considering that CAR is known to overestimate voluntary activation in healthy, uninjured populations.29,40Our results show that voluntary activation estimates are about 12% greater when using the CAR compared with percent activation,which is in agreement with our hypothesis and consistent with findings in healthy cohorts.29,40Our finding also seems to be supported by the existing anterior cruciate ligament literature, where quadriceps activation values are generally lower in studies in which voluntary activation was quantified with percent activation compared with those quantifying activation with the CAR. For example, studies using the percent activation method have shown that individuals with anterior cruciate ligament injuries have about 20%-25%of activation deficits,38,44,45which can persist even 2 years after surgery.44However, studies using the CAR method have shown that activation deficits are generally less than 10% both before surgery and at a time-point when individuals return to sports.46-51 The CAR method provides higher estimates of voluntary activation when compared with the ITT-based percent activation because it fails to account for the inability of the electrical stimuli to evoke a true maximal muscle torque.29As a result,the torque to which the evoked torque during contraction is normalized always ends up being higher in the CAR method, which results in an overestimation of voluntary activation. Although percent activation and the CAR are highly correlated, as shown in our study (r > 0.940) and in other studies,29,35it needs to be understood that direct comparisons of voluntary activation estimates cannot be made across studies using different techniques without correcting the CAR.29This factor is especially problematic when activation deficits are significant(e.g.,early after the injury or surgery),because the differences in voluntary activation estimates between the 2 methods increase as a function of increasing activation deficits (i.e., greater activation deficits will result in greater differences in voluntary activation estimates between CAR and percent activation). Moreover, it is important to note that the relationship between voluntary activation estimates derived from CAR and ITT (for both stimulators and pulse train conditions) becomes more variable when activation deficits are substantial (i.e., >40%) (Fig. 2).
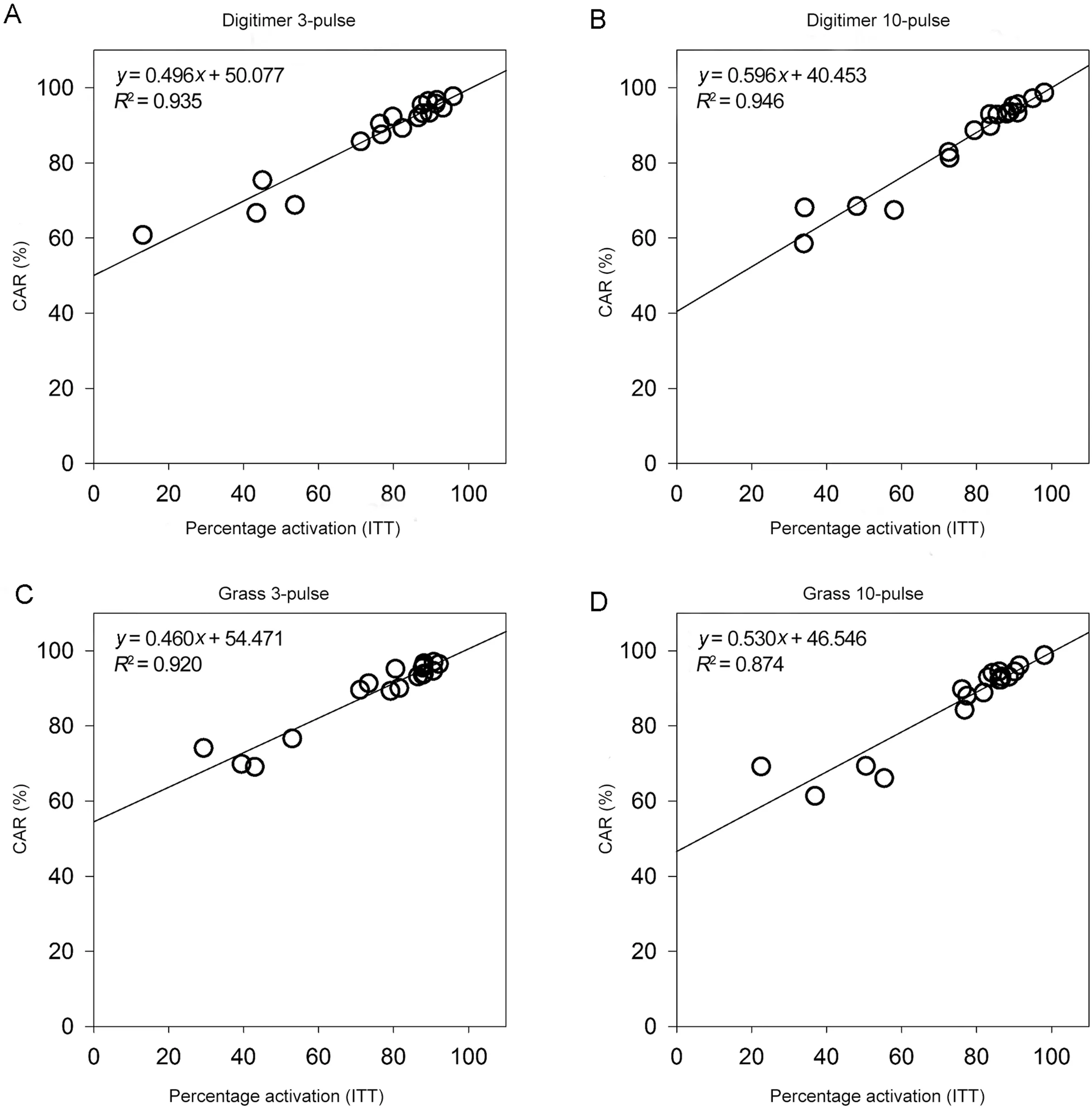
Fig. 2. Scatterplots demonstrating the relationship between voluntary activation estimates derived from the percent activation method and the CAR across all 4 experimental conditions:(A)Digitimer 3-pulse,(B)Digitimer 10-pulse,(C)Grass 3-pulse,and(D)Grass 10-pulse.Note that there was a strong linear relationship between activation values obtained from the percent activation method and the CAR for both constant current(Digitimer)and constant voltage(Grass)stimulators and 10-pulse and 3-pulse electrical trains.CAR=central activation ratio;ITT=interpolated twitch technique.TagedEnd
Both constant current (Digitimer) and constant voltage(Grass) stimulators have been used when quantifying voluntary activation.However,it was unclear until now whether the type of stimulator affects the estimates of voluntary activation.This information is important to reliably compare results across studies and also to choose the appropriate type of stimulator when assessing voluntary activation. Our findings indicate that either stimulator can be used for activation testing because the voluntary activation estimates did not differ significantly between stimulators. However, it is to be noted that the Digitimer produced greater evoked torque at rest than the Grass,indicating that the Digitimer has a greater ability to deliver the required current to maximally stimulate the quadriceps muscle during activation testing.Moreover,in our experience, the Grass stimulator sometimes overloads (i.e., the output circuit will shut off for safety reasons to prevent component damage because of overload or short circuiting) or plateaus before eliciting a maximal muscle torque (i.e., the evoked torque at rest does not plateau/decrease before the maximal stimulator output is reached), which could result in measurement errors.In the case of device overload,if adequate measures are not taken(i.e.,recleansing of the skin with alcohol to decrease skin impedance, reapplication of electrode pads, etc.), suboptimal stimulation may be delivered to the muscle. Furthermore, it is possible that the reliability of constant voltage stimulators may be lower for longitudinal investigations because the differences in skin/tissue impedance between days could alter the amount of current delivered to the muscle.For these reasons,it may be more beneficial to use a constant current stimulator as opposed to a constant voltage stimulator(like Grass)for voluntary activation testing.
The number of pulses in the electrical stimuli are known to affect voluntary activation estimates.16,52Previous research has shown that voluntary activation values are more consistent between trials and are also better estimated with a higher number of pulses.30,40,41,52However, the benefits of a higher number of pulses plateau after 3 or more pulses for the percent activation method, but not for the CAR.52,53Our results corroborate these findings;we found no difference in voluntary activation estimates between pulse train conditions when using the percent activation but did find differences between pulse trains when using the CAR. The differences in voluntary activation values between pulse train conditions were only observed with the CAR and not with percent activation because of how the activation values are computed in these techniques. In the CAR method, the superimposed torque(i.e.,evoked torque during MVIC)is normalized to the total torque during MVIC (i.e., MVIC+superimposed torque), whereas in the percent activation method, the superimposed torque is normalized to the torque evoked by the same stimulus at rest.Thus,unlike CAR estimates,the percent activation estimates are less susceptible to differences in pulse parameters because any differences in the superimposed torque due to differences in pulse trains are better accounted for by normalizing it to the evoked torque at rest. Considering that voluntary activation values derived from the CAR are significantly affected by the number of pulses in the electrical stimuli, we recommend using percent activation derived from the ITT or,at the very least,employing a wider pulse CAR train(-10 pulses)to minimize the overestimation of voluntary activation derived from CAR.

Fig.3. Scatterplots demonstrating the relationship between voluntary activation estimates derived using the 10-pulse and 3-pulse electrical stimuli.Note that there was a strong linear relationship between activation values obtained from the 3-pulse and 10-pulse electrical stimuli for both stimulators (constant current (Digitimer,A and B)and constant voltage(Grass,C and D))and quantification techniques(percent activation,A and C;CAR,B and D)used in this study.CAR=central activation ratio.
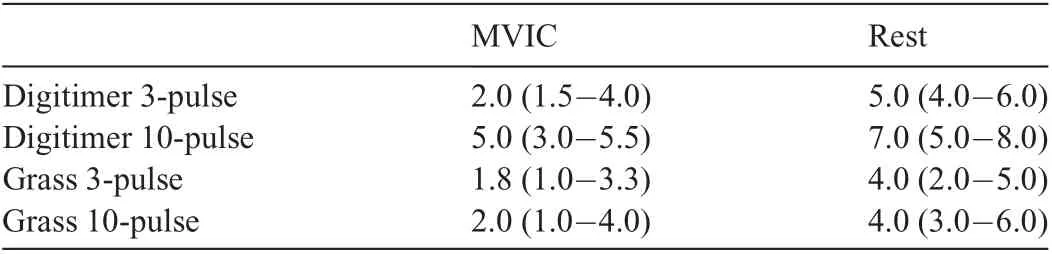
Table 4 VAS score of discomfort associated with electrical stimuli during MVIC and at rest.
It is to be noted,though,that the discomfort associated with the electrical stimulation is a key factor that limits the ability of an investigator to select a wide pulse train during voluntary activation testing. This discomfort is particularly higher when providing an electrical stimulus at rest than during an MVIC.7,35As a result,many investigators favor the use of the burst superimposition technique over the ITT. Although our findings confirm that participant discomfort during the resting stimulation was greater than during the MVIC,the discomfort owing to 3-pulse electrical stimuli at rest was similar to 10-pulse electrical stimuli during contraction (median VAS scores of 4.0 and 3.8, respectively). Hence, using a 3-pulse ITT instead of a 10-pulse CAR will provide more accurate voluntary activation estimates while simultaneously minimizing participant discomfort during activation testing.
There are some potential limitations to this study.We evaluated voluntary activation at 90˚of knee flexion even though activation deficits are known to be higher at shorter knee angles(i.e.,<90˚).7However,most studies have used the 90˚angle for quadriceps strength and activation testing.8,10,11,13,15,34,47,48,54It is unclear if our results for the 90˚knee flexion angle are generalizable to other knee angles, and further research is needed to verify whether our findings hold true at different knee angles. Another limitation involves our use of predetermined stimulus intensities based on previous research,since we wanted to minimize participant discomfort during testing. However, it is possible that optimal intensities may have differed for each person29and could have resulted in some measurement error when estimating voluntary activation. Finally, fatigue and/or participant familiarization with electrical stimulation may have affected voluntary activation estimates and VAS scores. However, we believe that this is extremely unlikely to have affected the general findings in our study given that we provided adequate rest between trials (2 min), randomized the order of testing conditions, and did not observe significant differences in MVIC peak torque values across conditions (Table 2).
5. Conclusion
The results of this study indicate that the estimates of voluntary activation are not affected by the type of electrical stimulator but are significantly affected by the quantification technique used during voluntary activation testing in individuals with ACLR. Notably, in our sample, CAR-based estimates were about 12%greater than the estimates derived from ITT-based percent activation—this difference in activation estimates is expected to further increase with an increase in voluntary activation deficit (e.g., individuals with acute anterior cruciate ligament injury/surgery). The results also indicate that voluntary activation estimates derived from the ITT-based percent activation are less affected by variations in pulse trains and stimulators when compared with those derived from the CAR. However, we note that the discomfort due to evoked torque at rest in ITT is greater. Nonetheless, a 3-pulse ITT instead of a 10-pulse CAR with Digitimer or Grass could be used to accurately quantify voluntary activation estimates while simultaneously keeping participant discomfort at the minimum.
Acknowledgments
This work was partly supported by the National Institute of Child Health and Human Development of the National Institutes of Health(Grant No.R21 HD092614).
Authors’contributions
SAG contributed to the acquisition,analysis and interpretation of data, and writing of the manuscript; KMR and SRB contributed to the acquisition of data and critical review and editing of the manuscript;RMPS contributed to the study conception and design, analysis and interpretation of data, and critical review and editing of the manuscript; CK contributed to the study conception and design,analysis and interpretation of data, writing, and critical review and editing of the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
猜你喜欢
建材发展导向(2021年12期)2021-07-22
科学与财富(2019年29期)2019-10-21
建筑建材装饰(2016年13期)2017-01-04
建筑工程技术与设计(2015年29期)2015-10-21
小康(2015年12期)2015-06-23
海外英语(2013年5期)2013-08-27
 Journal of Sport and Health Science2022年1期
Journal of Sport and Health Science2022年1期
- Journal of Sport and Health Science的其它文章
- Residual force enhancement in human skeletal muscles:A systematic review and meta-analysis
- Sex differences in injury rates in team-sport athletes:A systematic review and meta-regression analysis
- Physical exercises for preventing injuries among adult male football players:A systematic review
- Interference screws vs.suture anchors for isolated medial patellofemoral ligament femoral fixation:A systematic review
- Incidence of injuries in professional snow sports:A systematic review and meta-analysis
- “When you’re down,stay down”:A lesson for all competitive alpine skiers supported by an ACL rupture measured in vivo