
“When you’re down,stay down”:A lesson for all competitive alpine skiers supported by an ACL rupture measured in vivo
2022-03-24 02:36orgSporriErihullerJosefKroll
J€org Sp€orri*,Erih M€uller,Josef Kr€oll
a Sports Medical Research Group,Department of Orthopaedics,Balgrist University Hospital,University of Zurich,Zurich 8008,Switzerland
b University Centre for Prevention and Sports Medicine,Department of Orthopaedics,Balgrist University Hospital,University of Zurich,Zurich 8008,Switzerland
c Department of Sport Science and Kinesiology,University of Salzburg,Hallein-Ri 5400,Austria
Abstract
Keywords: Alpine skiing;Athletes;Injury mechanism;Injury prevention;Knee injuries
1. Introduction
In the sport of competitive alpine skiing,traumatic injuries to the knee joint are frequent, with a rupture of the anterior cruciate ligament (ACL) being the most typical diagnosis.1-3 At the top level, absolute rates of ACL injuries have been reported as 5.4 and 5.5 injuries/100 athletes/season for females and males, respectively.4A tear of the ACL is also the most common injury requiring surgical treatment.5Concurrent injuries are prevalent with ACL injuries,6and serious long-term consequences such as a 4- to 6-fold increased risk of osteoarthritis have been reported.7Moreover,recurrence of ACL injuries is likely,and nearly 50%of competitive alpine skiers with a primary ACL injury must expect a secondary ACL injury upon return-to-sport.8
To develop effective injury prevention measures, however,a deeper understanding of the events leading to the injury situation as well as a precise description of the injury mechanism itself is crucial.9In the context of elite competitive alpine skiing, the most typical mechanisms resulting in rupture of the ACL are the so-called “slip-catch”, “dynamic snowplough”,and “landing back-weighted” mechanisms.10The “slip-catch”and“dynamic snowplough”mechanisms typically happen during ski turns, while the “landing back-weighted” mechanism occurs mainly when landing from a jump.10
In the first 2 mechanisms, the ski racer initially loses balance inward and/or backward,with the outside ski reducing its contact with the snow and drifting away.11In the further sequence, the inner edge of either the outer or inner ski abruptly catches on the snow surface, resulting in excessive compression of the knee joint, knee valgus, and internal rotation.12While the arthrokinematics during these injury mechanisms are similar to those known for ACL injuries in recreational skiing,13the causes and events leading to the injury situation are very specific to competitive alpine skiing,with a particularly direct ski-snow interaction due to aggressive equipment and artificially prepared snow surfaces.
As part of the“landing back-weighted”mechanism,the third competitive alpine ski racing specific ACL injury mechanism,the ski racer typically loses balance during flight due to backward angular momentum received at the jump take-off.11This results in the ski racer landing on the tails of the skis first,with the entire skis “clapping” down on the snow surface secondarily.10Thus, upon first contact with the ground, an angular momentum rotates the skis forward as the ski racer falls backward, thereby inducing tibiofemoral compression and causing the tibia to be pushed forward by the stiff rear part of the ski boot.10In addition, sudden and aggressive activation of the quadriceps muscles during jump landing may further increase anterior tibial translation and stress on the ACL.14,15
However, despite the existing knowledge on the mechanisms of competitive alpine skiing-related ACL injuries, primarily derived from systematic video analysis or theoretical modeling/simulation studies, comprehensive biomechanical insights into real in vivo ACL injury cases(including kinematics,kinetics,and muscle activation patterns)are currently lacking. Of course, this is not really surprising, since injury cases in which biomechanical data are measured in vivo are very rare.16Accordingly,the current dataset of a ski racer who sustained an ACL injury while equipped with measurement devices is quite unique. As such, it may provide a better understanding of the chain of events,the acting forces,and the accompanying muscle activation patterns during a real in vivo ACL rupture in competitive alpine skiing and help to derive effective prevention strategies.
The aim of the present study was,therefore,to biomechanically describe the corresponding ACL injury case from a functional perspective and in comparison to “normal” reference skiing.
2. Materials and methods
2.1. Measurement protocol
During a biomechanical field experiment,a male European Cup-level competitive alpine ski racer (age=30 years; body height=179 cm; body weight (BW)=78 kg) suffered an accidental tear of the ACL on the right knee without any other concomitant injuries.The injury occurred at the 9th turn(i.e., 5th left turn) of a giant slalom course set with 27 m linear gate distance and 6 m horizontal gate offset. Average slope inclination was 21˚. This study was approved by the Ethics Committee of the Department of Sport Science and Kinesiology at the University of Salzburg (EC_NR.2010_03),and the participant gave his written informed consent prior to participation.
2.2. Data collection and analysis
During the 8 turns (4 left turns) of injury-free skiing giant slalom,as well as during the left turn at which the ACL injury occurred, the ski racer was filmed by 2 panned, tilted, and zoomed High Definition Video cameras at 50 Hz(Sony PMWEX3; Sony Group Corporation, Tokyo, Japan). Bilateral knee and hip flexion angles were measured with 4 inertial measurement units attached to the shanks, thighs, and the sacrum and recording at a frequency of 500 Hz as well as with an evaluation algorithm proposed and validated in a previous study.17Tailored for alpine skiing, this method fuses 3-dimensional(3D) angular velocity and acceleration data, calculates driftreduced 3D segment orientations, and then determines knee and hip flexion angles with 0˚representing full extension.Accuracy and precision for estimating knee angle were found to be 1.7˚and 4.8˚; those for hip angle were -3.8˚and 6.0˚,respectively.17Ground reaction force (GRF)acting on the left and right leg were recorded using PEDAR pressure insoles at 100 Hz (Novel GmbH, Munich, Germany). For professional skiers performing cut turns on a steep slope,the accuracy and precision of the BW-normalized GRF measurement was reported to be 0.33 N/BW and 0.11 N/BW, respectively.18In addition, instantaneous rate of force development (RFD) was calculated as the change between 2 adjacent GRF data points divided by the change in time.A second-order Butterworth filter with a cut-off frequency of 6 Hz was applied to low-pass filter all kinematic and kinetic data.The cut-off frequency was set based on the presumption that the physiological regulatory capabilities in humans are limited to a maximum frequency of about 6 Hz.19,20
Electromyographic activity was recorded in accordance with previous studies in alpine skiing and cross-country skiing.21,22Signals from the gluteus maximus(GM),biceps femoris (BF), rectus femoris (RF), and vastus medialis (VM)muscles were captured by surface electromyography (EMG)on the right side using pre-gelled bipolar Ag/AgCl surface electrodes (10 mm diameter, 22 mm spacing; Skintact; Leonhard Lang GmbH, Innsbruck, Austria). Before attaching the electrodes, the skin was shaved, lightly abraded, degreased,and disinfected with alcohol. In accordance with international standards,the electrodes were placed in parallel on the surface of the muscle belly in the direction of the fibers.23The reference electrode was attached on the fibular head above the ski boot. EMGs were amplified at the source (bandwidth:10-500Hz,3 dB;EMG amplifier;Biovision,Wehrheim,Germany), recorded at 2000 Hz (Biovision Input Box; Biovision)and stored on a tablet PC(Viliv S5 Express P;Yukyung Technologies,Seoul,Republic of Korea).For data post-processing,a second-order Butterworth bandpass filter with a cut-off frequency of 10 Hz/300 Hz and a root mean square with 200 data points was applied.
All measurement systems were electronically synchronized.The 2 High Definition Video cameras were internally genlocked and optically synchronized with the other systems by recording an LED light activated by an external trigger signal.Post-processed data from all measurement systems were split into separated turn cycles (“normal” skiing turns and the turn where the injury occurred) and time-normalized with 300 data points.Turns separation was performed based on automatically determined minima in the total GRF curves at the turn change,as was done in previous studies.24-26 The right (outside) leg data from the left turn where the injury occurred was then used to describe the injury-initiating event in comparison to the reference data during “normal” skiing (i.e., the right or outside leg data from the preceding 4 left turns of the same run).
3. Results
The chain of events leading to the injury situation and the injury mechanism itself are illustrated in Fig.1.Corresponding kinematic and kinetic data are highlighted in Fig.2,EMG data in Fig. 3. A video sequence showing the injury occurrence in real time is provided as online Supplementary File 1.
3.1. “Normal”reference skiing
During “normal”, injury-free skiing, the average GRF on the right(i.e.,turn outer)leg was typically between 450 N and 1500 N,with individual peaks reaching 2500 N.After turn initiation, there was a constant increase in GRF, which reached its maximum when steering out of the fall line after gate passage. RFD remained relatively constant throughout the turn,oscillating in the range of§50,000 N/s and showing peaks up to 200,000 N/s. In the initial phase of the turn, when GRFs were rather low, an increasing knee and hip extension was observed. Starting from a knee angle of about 110˚and a hip angle of approximately -100˚,the knee and hip extension subsequently reached a maximum of around 40˚and -50˚,respectively,and then remained almost constant in the further course of the turn.The activation patterns of GM,BF,RF,and VM of the right (outside) leg showed similar patterns among themselves:increasing activity while steering into the fall line,followed by a steady plateau and a decrease in the last quarter of the turn.
3.2. Description of the ACL injury inciting event
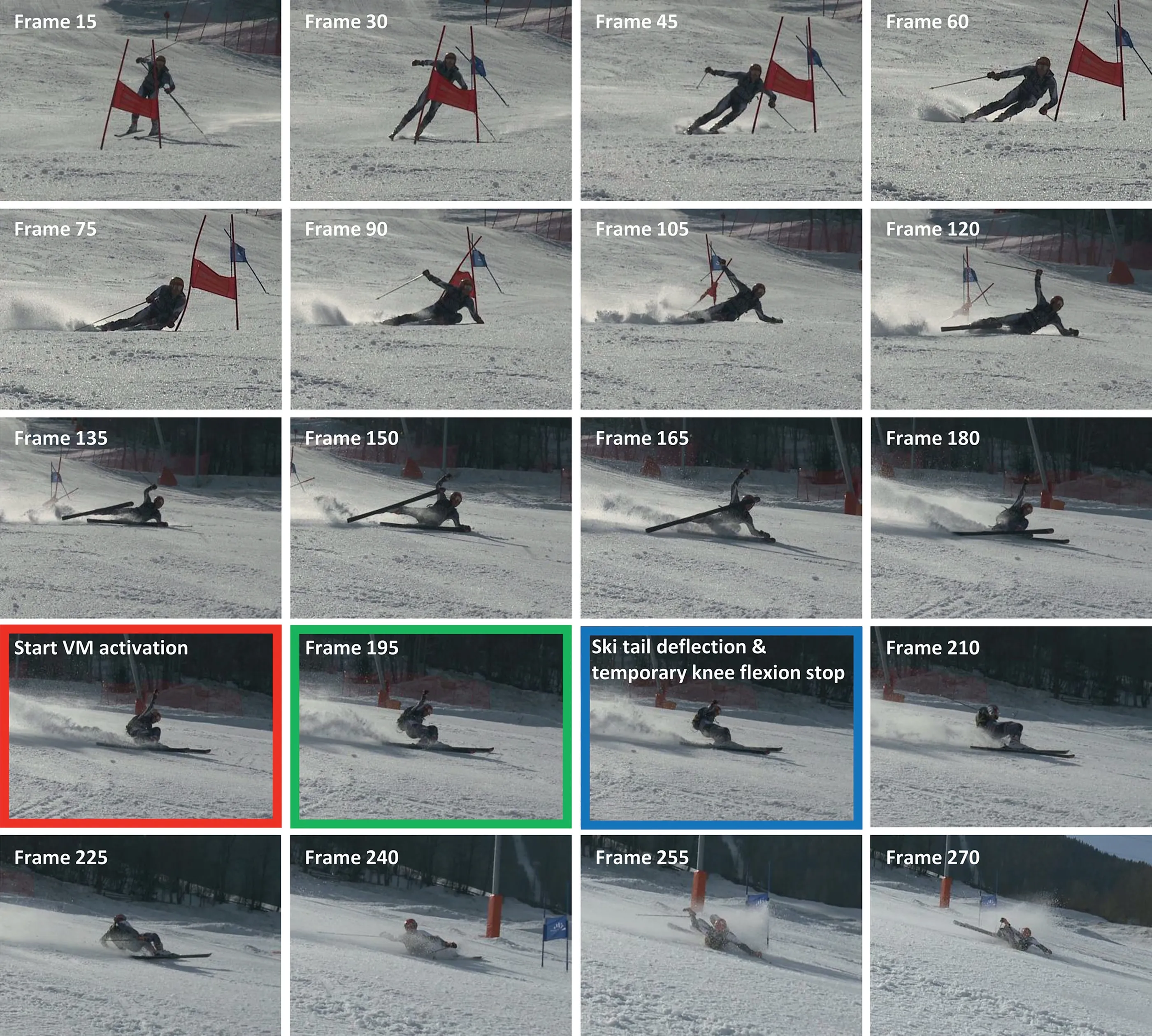
Fig.1. Static image series of the injury-relevant giant slalom turn starting from the turn switch.Highlighted frames:red-start of the aggressive sudden activation of the VM muscle;green-point of the highest acting force;blue-ski tail deflection and temporary stop of knee flexion.It is assumed that the ACL injury occurs in the area of one of the highlighted frames.ACL=anterior cruciate ligament;VM=vastus medialis.
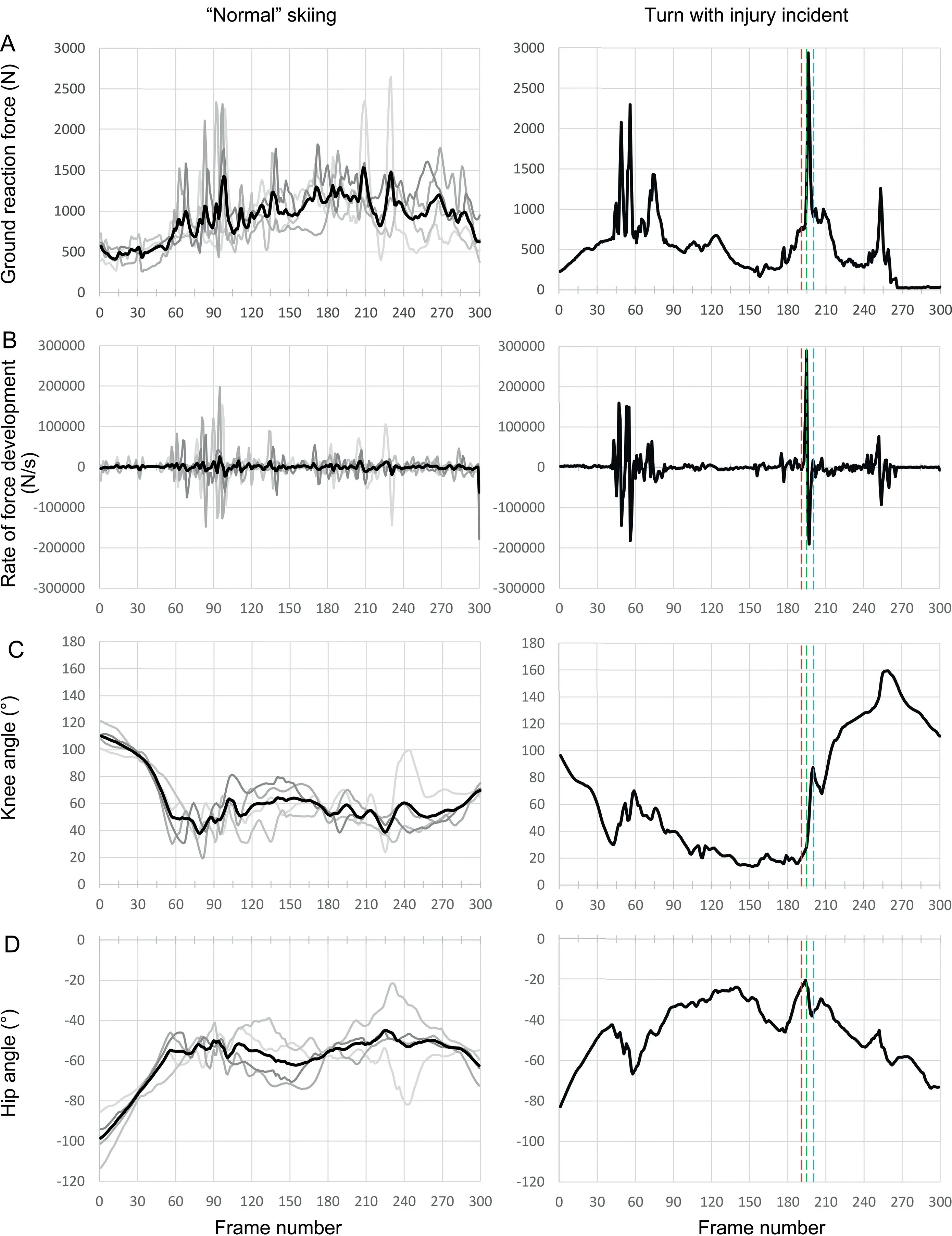
Fig.2. Kinematic and kinetic data of(A)ground reaction force,(B)rate of force development,(C)knee angle,and(D)hip angle.Left column:Right(outside)leg data from the 4 left turns of the same run preceding the injury (= normal injury-free skiing). Right column: right (outside) leg data from the left turn where the injury occurred.A value of 0˚knee and hip flexion angle is representing full extension.Highlighted frames:Red line-start of the aggressive sudden activation of the VM muscle;Green line-point of the highest acting force;Blue line-ski tail deflection and temporary stop of knee flexion.It is assumed that the ACL injury occurs in the area of one of the highlighted frames.ACL=anterior cruciate ligament;VM=vastus medialis.
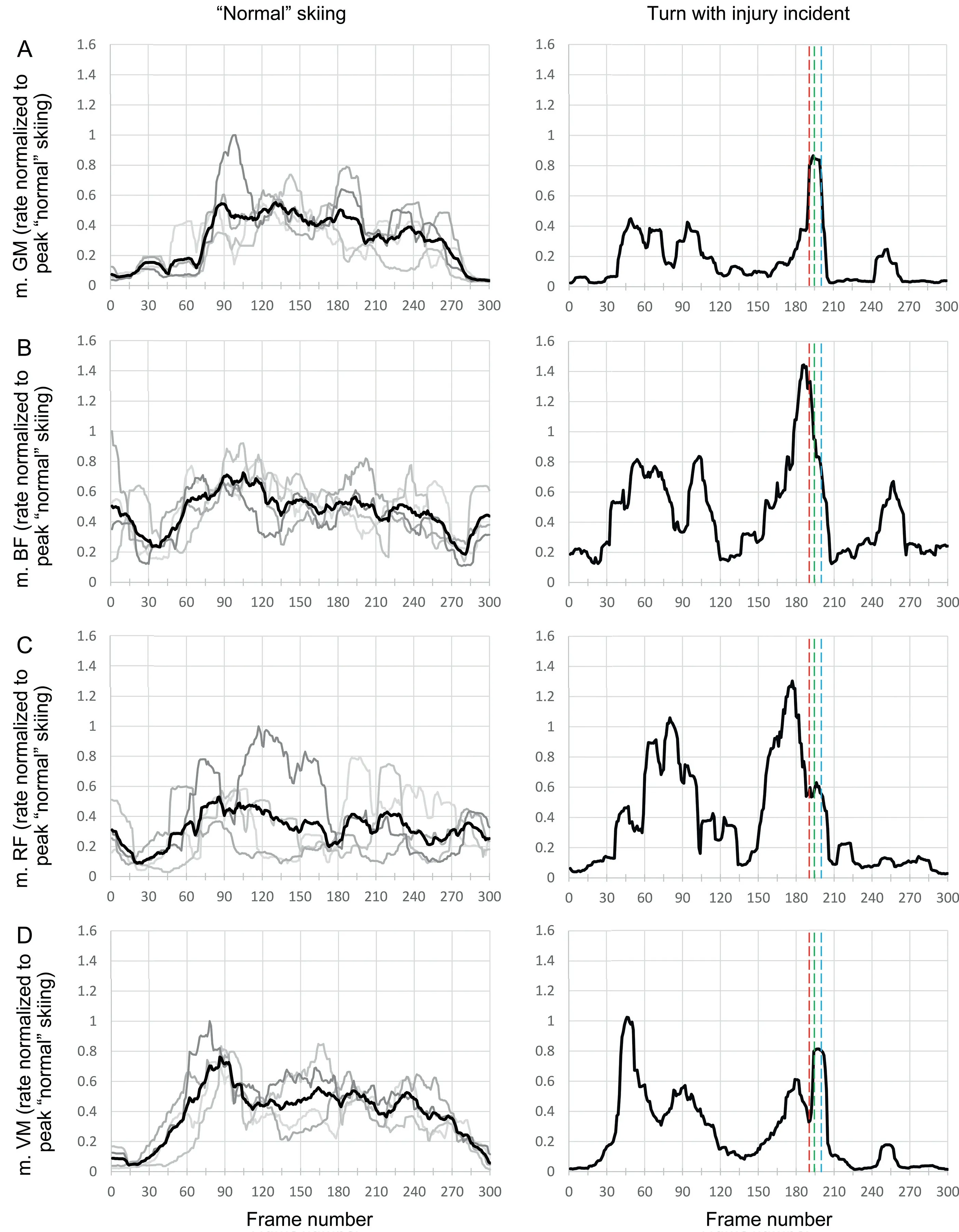
Fig.3. Electromyography data of(A)m.GM,(B)m.BF,(C)m.RF,and(D)m.VM.Left column:right(outside)leg data from the 4 left turns of the same run preceding the injury (= normal injury-free skiing); Right column: right (outside) leg data from the left turn where the injury occurred. Highlighted frames: Red line-start of the aggressive sudden activation of the vastus medialis muscle;green line-point of the highest acting force;Blue line-ski tail deflection and temporary stop of knee flexion.It is assumed that the ACL injury occurs in the area of one of the highlighted frames.ACL=anterior cruciate ligament;BF=biceps femoris;GM=gluteus maximus;m.=musculus;RF=rectus femoris;VM=vastus lateralis.
At the apex of a turn,the ski racer lost balance inward and began to slide sideways in a controlled manner.While the left(inside) leg was sliding on the ground, the right (outside) leg was actively abducted upward without touching the snow surface(Fig.1,Frames 120-150).The ski racer then tried to get back up by dropping his right leg back onto the snow surface(Fig. 1, Frames 150 to 195). At first, there was EMG activity in the knee stabilizing muscles BF, RF, and VM as well as in GM to control this dropping (Fig.1 Frames 150-180; Fig.3).However, just before the outer ski touched the ground, this dropping was accompanied by a decrease in EMG activity in the knee stabilizing muscles BF, RF, and VM, while GM remained pre-activated (Fig.1 Frames 180-195; Fig.3). Then,when the inside edge of the right (outer) ski caught the snow surface,there was a rapid increase in peak force(Fig.1 Frames 195; Fig.2; RFD, approximately 300,000 N/s; maximal GRF,around 3000 N, i.e., 3.84 N/BW on 1 leg). This peak force resulted in rapid knee flexion (from 16˚to 82˚; peak angular velocity, 2010˚/s) and aggressive sudden activation of VM(from 0.36 to 0.82 normalized to peak “normal” skiing rate),while BF and RF further decreased their activation levels(Figs. 2 and 3, Frame 195 to blue line). Simultaneously, the activation of GM suddenly increased from 0.38 to 0.84 normalized to peak“normal”skiing rate.Shortly thereafter,probably due to the backward momentum of the skier falling backward,a deflection of the tail of the outer ski was observed,and the knee temporarily stopped bending(Fig.2,blue line to Frame 210). In the subsequent sequence, GRF, RFD, and the activation values of all muscles decreased again, while knee and hip angles in flexion continued to increase.
4. Discussion
4.1. Potential ACL injury triggers
During the current ACL injury mechanism, we observed aggressive sudden activation of the VM muscle,while all other knee stabilizing muscles remained deactivated. This was likely caused by the inside edge of the right ski catching the snow surface as the ski racer attempted to get up again by dropping his outside leg back onto the snow surface. Such rapid and imbalanced muscle activation patterns likely resulted in excessive anterior translation of the tibia relative to the femur and,therefore, may be a key component of the observed ACL injury mechanism.15As far as possible prevention is concerned, this ACL injury trigger is hardly avoidable once the ski racer has decided to stand up again during the lateral slide.It seems that when gravity is used to passively drop the outer leg, there is a functional deactivation of the knee stabilizing muscles. It appears that the skier cannot effectively counteract this functionally induced drop in EMG pre-activity of the knee stabilizing muscles, especially the hamstrings, along with the subsequent high forces acting when the ski touches the ground.
Another potential ACL injury trigger could be a bootinduced anterior drawer of the tibia relative to the femur. In our observations, such a trigger might be reflected in the deflection of the outside ski tail as it dug into the snow surface and the temporary stop of knee flexion that can be observed around the estimated time of injury(Fig.1,blue frame).While the skier was falling backward, the mechanical constraint of the ski tail acting as a lever and the rigid connection of the ski with the rear part of the ski boot may have exerted an anteriorly directed force on the tibia. Such force may have further increased the load on the ACL and the already heavily loaded quadriceps muscle.14
4.2. “Sliding edge-catch”—A new combinatorial injury mechanism in alpine ski racing?
The current injury case bears some similarity to the “slipcatch” and the “landing back-weighted” ACL injury mechanisms described by Bere and colleagues.10-12 It also has strong similarities to parts of the“phantom foot”mechanism,which is very common in recreational skiing.27Regardless, the current case does not fit perfectly into any of the 3 mechanism categories. First, the chain of events leading to the injury includes a very specific and unique phase in which the entire body touches the ground and the ski racer,having lost his balance,slides several meters on his side. Second, the potential injury triggers appear to be a combination of the ski rapidly catching the snow surface(typical of the“slip-catch”mechanism)10and the tail of the ski acting as a lever(typical of the“landing back-weighted”and “phantom foot” mechanisms),10,27rather than any standalone mechanism. Based on these observations, the present mechanism,which we refer to as a“slipping edge-catch”mechanism, may be considered as a new and combinatorial ACL injury mechanism that has not yet been described in this form for ski racers in the literature. Nevertheless, despite this deficiency in the current scientific literature,based on non-scientific daily observations of coaches, the current mechanism is not uncommon in competitive alpine skiing, as ski racers always strive to stay in the race course as long as possible.
4.3. Lessons learned from an in vivo ACL rupture
As mentioned above, in view of the high acting forces as well as the functionally conditioned drop in EMG activity of relevant muscle groups when dropping the abducted outer leg in the direction of the snow surface, the ski racer has hardly any chance to protect the ACL once the ski has caught the snow surface. Accordingly, effective prevention strategies may instead be needed to address the chain of events beforehand.
The most effective way, of course, would be to keep the balance instead of slipping sideways while turning.Young ski racers in particular should train their general postural control skills and develop a skiing technique focused on proper loading of the outside ski and maintaining dynamic equilibrium.In this context, a recent study by Westin and colleagues28reported that an injury prevention program that included offsnow physical training and on-snow ski technical training was able to reduce the incidence of ACL injuries by 45%.
However,competitive alpine ski racers naturally perform at their limits, which is why out-of-balance situations will never be completely avoidable. Thus, based on our data, ski racers should be taught not to get back up after a side slip until they have come to a stop, especially if there is no way to get back on the course.Accordingly,Johnson and colleagues’29recommendation,“When you’re down,stay down”,though primarily directed at novice and recreational skiers, may also apply to competitive alpine skiers under certain circumstances (e.g., to minimize risk when there is“nothing to win”).In a way,however,this contradicts the coaches’doctrine of“always fighting your way back on course”, even during training runs, for example, so as to avoid inculcating the instinct to give up too easily. Therefore, appropriate and situation-dependent decisions as well as suitable fall strategies should be an essential part of the training path of young ski racers.Ettlinger and colleagues27trained ski patrollers and instructors to take a similar approach and found a 62%decrease in serious knee sprains.
4.4. Methodological considerations
The major limitation of the current study may be the underlying single-subject design, which limits the generalizability of the present findings. Nevertheless, the current dataset of a ski racer who sustained an ACL injury while equipped with measurement devices is unique and may contribute to a better understanding of the chain of events during a real in vivo ACL rupture in alpine skiing thanks to the insights it allows regarding acting forces and the activation patterns of knee stabilizing muscles.
5. Conclusion
The current study emphasizes the importance for ski racers who slide sideways after losing their balance to avoid getting back up before they have stopped sliding and to remember:“When you’re down,stay down.”
Acknowledgments
This study was financially supported by the International Ski Federation(FIS)Injury Surveillance System(ISS).
Authors’contributions
Both JS and JK contributed to the study design,data collection, data evaluation, data interpretation and manuscript writing; EM provided support in funding acquisition, study conceptualization, and revising the manuscript. All authors have read and approved the final version of the manuscript,and agree with the order and presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found,in the online version,at 10.1016/j.jshs.2021.11.004.
 Journal of Sport and Health Science2022年1期
Journal of Sport and Health Science2022年1期
- Journal of Sport and Health Science的其它文章
- Residual force enhancement in human skeletal muscles:A systematic review and meta-analysis
- Sex differences in injury rates in team-sport athletes:A systematic review and meta-regression analysis
- Physical exercises for preventing injuries among adult male football players:A systematic review
- Interference screws vs.suture anchors for isolated medial patellofemoral ligament femoral fixation:A systematic review
- Incidence of injuries in professional snow sports:A systematic review and meta-analysis
- Maximizing recovery time between knock-out races improves sprint cross-country skiing performance