
Sex differences in injury rates in team-sport athletes:A systematic review and meta-regression analysis
2022-03-24 02:34AstriZchKrstnHollnrAstriJungSimonStiAnrsGrollJonsHinrFlorinNowkDnilPirAnnLinRhl
Astri Zch*,Krstn Hollnr,Astri Jung,c,Simon Sti,Anrs Groll,Jons Hinr,Florin NowkDnil PirAnn Lin Rhl
a Department of Human Movement Science and Exercise Physiology,Friedrich Schiller University Jena,Jena 07749,Germany
b MSH Medical School Hamburg,Hamburg 20457,Germany
c Swiss Concussion Center,Schulthess Klinik,Z€urich 8008,Switzerland
d Department of Human Movement,Training and Active Aging,Heidelberg University,Heidelberg 69117,Germany
e Department of Statistics,Technical University of Dortmund,Dortmund 44227,Germany
f Department of Sports and Exercise Medicine,Institute of Human Movement Science,University of Hamburg,Hamburg 20146,Germany
Abstract
Keywords: Athletes;Female;Injuries;Male;Team sports
1. Introduction
In recent years, sports injuries have been extensively researched in terms of their incidence,risk factors,and prevention measures.Team-sport athletes appear to be at particularly high risk of injury1due to the complex characteristics of their games, which usually include varied movements and interaction with the ball, team-mates, and opponents. The pooled incidence rates of match injury are about 36 injuries per 1000 exposure hours in elite male football (soccer)2or 81 injuries per 1000 exposure hours in elite male rugby.3However, specific injury rates vary according to circumstances,such as injury definition (time loss or all medical attention),4age level and type of exposure(match or training,tournament or season).Numerous studies that include seasonal injury rates for football and rugby exist, but fewer data are available for other team sports,such as basketball,volleyball,handball,and ice and field hockey. Data from the 2012 and 2016 Olympic Games indicate that the percentages of injured players in handball(females:10.7%and 26.3%;males:17.4%and 18.0%)and field hockey (females: 9.4% and 17.2%; males: 17.3% and 18.0%) are almost as high as in football (females: 14.8% and 45.0%; males:13.2%and 27.0%)and rugby(females: 15.3%;males 21.1%(2016 only)).5,6
A frequently overlooked aspect of epidemiological injury data is sex-specific differences. Systematic reviews and metaanalyses in recent years7-9 indicate a higher risk of ankle sprain,7concussion,8and anterior cruciate ligament (ACL)injury9in females. Although these reviews include a large number of studies, no sport-specific data are reported. Also,study samples vary, with some including a mixture of professional,(semi)amateur,collegiate,high school,and recreational and military athletes from various sports. One recently published meta-analysis shows a different risk for running-related injuries between females and males.10However, no such data exist for team sports. Another problem that may have more serious consequences for the interpretation of pooled data is the lack of differentiation among studies with differing injury definitions or periods of data collection (tournament vs. season).Comparing pooled data of surveillance studies that were carried out with males or females only may lead to an increased risk of bias.4,11,12As a consequence, it remains uncertain whether reported sex differences in injury incidence rates are caused by differences in injury definition,data collection,and/or sample characteristics.
Epidemiological studies reporting injury rates for both females and males during a single season using the same methods are rare,13-15 and results are inconclusive.For example,2 studies on injuries in elite football13,14agreed on a higher overall, training and match injury incidence in men (7.714and 8.313per 1000 h)compared to women (5.514and 6.313per 1000 h). However,severe injuries were similar for both sexes in one study(both 0.7 per 1000 h),14whereas the other study reported a higher incidence in women (1.42 per 1000 h) compared to men (0.95 per 1000 h).13In both studies,13,14the severity of injuries was defined as time loss of more than 28 days, which raises the question of whether females may be predisposed to injuries that require a long-term healing process and/or postoperative recovery period,such as ACL ruptures.16It is also mostly unclear whether sexspecific anatomical or physiological aspects contribute to differences in joint laxity or sensorimotor control mechanisms17,18and may,therefore,influence the risk of specific injury characteristics involving the ligament,tendon,or muscles.
Altogether, the current state of knowledge regarding sexspecific differences of injuries in team sports is influenced largely by studies conducted under particular circumstances and with a particular methodology,often with only one sex or the other. Therefore, the present study performed a metaanalysis to compare injury rates of both sexes in elite adult or youth team sports. To avoid systematic bias in data pooling,only studies with data for both sexes were included. Potential moderators in terms of competition characteristics(tournament vs. season), injury definition, or age level were considered using meta-regression analysis.
2. Methods
A systematic review with meta-analysis and meta-regression was conducted according to the Meta-analyses of Observational Studies in Epidemiology guidelines.19A review protocol is registered at the University of York, Centre for Reviews and Dissemination PROSPERO database:Registration No. CRD4201911883 (http://www.crd.york.ac.uk/prospero/).
2.1. Data search and selection criteria
Systematic database searches were performed through February 2021 using PubMed, Web of Science, and Google Scholar. For these, the term “injuries” was combined (AND)with “football” OR “soccer” OR “basketball” OR “handball”OR “volleyball” OR “rugby” OR “hockey”. Additionally,manual searches were performed of relevant systematic reviews and meta-analyses2,7-9 as well as reference lists within reviewed articles. The literature search was conducted by 2 researchers (FN and DP) with the assistance of 2 experienced researchers(ALR and AZ).
Studies involving a prospective cohort design were included if they reported (1) injury and exposure data, (2) the data for both female and male athletes,and(3)the data in one of the following Olympic team sports:basketball,field hockey,football, handball, rugby union or rugby sevens, and volleyball. These sports were chosen because they typically include multiple jump-landing, side-cutting, and change-of-direction movements, which are thought to be primarily responsible for noncontact injuries.20,21Studies were considered relevant if they (1) were published in the English, Spanish, or German language,(2)appeared in peer-reviewed journals,(3)reported acute and/or overuse injuries, (4) took place during tournaments or playing seasons, (5) were published after the year 1998, (6) performed a surveillance of players -16 years old,and(7)reported injuries in a high-level or collegiate league or in major senior or youth tournaments.Studies with data collection before 1998 were excluded in order to avoid the issue of changing physical demands in team sports over the past 2 decades,22,23which could influence the injury rate ratio between sexes.
Exclusion criteria related to insufficient data reporting included a lack of sex-specific data on injury and/or exposure,missing age in collegiate or youth players, and no specific team sport mentioned. Studies with a retrospective or mediabased data analysis were also excluded. Injury reports from central databases (e.g., National Collegiate Athletic Association) were excluded due to the lack of detailed information about the study sample (e.g., age) as well as in order to avoid duplicate injury data from the same surveillance period as reported in various studies. Studies of nonprofessional, semiprofessional, military, or high-school players under the age of 16 were also excluded.Eligible studies of the same team sport were carefully checked for potential overlaps in sample and surveillance period (e.g., same tournaments or seasons). In cases of overlap,24,25the study with the longer time period or greater amount of data was chosen.
2.2. Data extraction
Data were extracted independently by 3 authors(ALR,DP,and AZ)for football and by 2 authors(AZ and FN)for all other sports. The following information was retrieved: sample size,sample characteristics (age level, nationality of players), year(s)of data collection,exposure data for female and male players,tournament and/or season,and injury definition(time loss,all medical attention, or any physical complaint). Extracted injury data were overall, match, training, severe, head, upper extremity,trunk,hip/groin,thigh,knee,ankle,and foot injuries as well as sprains,strains,concussion,ankle sprains,hamstring injuries, and ACL and Achilles tendon ruptures. Retrieved exposure data were exposure hours and athletic exposure.Discrepancies between authors were resolved by consensus.Severe injuries were defined by a time loss of 28 or more days26following the injury.
2.3. Assessment of study quality
Two authors (ALR and AZ) independently assessed the methodological quality of included studies.A rating scale was developed based on other scales for quality assessment.8,27,28The 19 items with a maximum possible score of 30 points were: inclusion criteria, participant recruitment, players’ characteristics, season and/or tournament data, exposure assessment (4 items), frequency of data recording (2 items), injury definition (2 items), injury data collection (2 items), injury details (2 times), data reporting (2 items), and drop-out (for details, see Supplementary Table 1). The scoring for each study was summed for the total quality score. Disagreements between raters were resolved by consensus. For discrepancies that could not be resolved, a third author was consulted (DP for football, FN for all other sports). Publication bias was checked by visual inspection of funnel plots (incidence rate ratios against standard errors).
2.4. Statistical analysis
Injury data were analyzed using R software(Version 4.0.5;The R Core Team, Vienna, Austria) for meta-analysis and meta-regression.29Injury outcomes were (1) all injuries; (2)match injuries; (3) training injuries; (4) severe injuries; (5)injuries of the head,upper extremities, trunk,hip/groin, thigh,knee, ankle, and foot; (6) sprain and strain; (7) concussion,ankle sprain,ACL rupture,and Achilles tendon rupture.
The injury incidence rate ratio (IRR) between females and males with corresponding 95% confidence intervals (95%CIs)was calculated.The following equation was used for IRR calculation:(number of injuries of female athletes/exposure hours of female athletes)/(number of injuries of male athletes/exposure hours of male athletes).Only exposure hours were considered for the calculation because none of the included studies used other(athletic)exposure quantifications.The IRR resembles a ratio of the sex-specific (female/male) injury incidence rates. Consequently, a value smaller than 1 indicates a higher injury risk in males,and the closer the value is to 0,the larger is the difference in females. Meta-analysis included random effects based on a Mantel-Haenszel method for dichotomous data. A pooled estimate for the IRR was calculated for each outcome with two or more studies and summarized in a forest plot.Heterogeneity was assessed using the I2statistic.30
Meta-regression analyses were performed via the functions metainc and metareg from the R package meta31for each outcome for which 10 or more studies were available32in order to identify moderators that influenced the pooled estimates of the meta-analyses.33These categorial moderators were methodological characteristics that could potentially lead to an increased risk of bias4,12and that were reported consistently in the studies.They include(1)type of exposure(tournament vs.season), (2) injury definition (time loss vs. all medical attention/physical complaints),34(3)age level(senior vs.collegiate/youth players), (4) type of sports (football vs. rugby, basketball, handball, volleyball, or field hockey, respectively), and(5) study quality (-80% vs. <80%, cut-off representing the approximate median).The moderator“type of sports”had not 2 levels (like the other moderators) but 6 levels (one for each sport),so the level with the largest number of studies(football)was defined as the reference level. The reference level was then compared with each other sport.
3. Results
3.1. Search results
A total of 19,388 references in the 6 team sports were identified in the database search(Fig.1).Of those,4482 duplicates or noneligible language studies were excluded(21%).Another 14,379 studies were eliminated after reading the title and abstract. After full-text screening, 507 additional studies were excluded because they (1) did not report exposure data or required sample characteristics, (2) had no clear injury definition, or (3) collected data retrospectively or by using central databases. Finally, data from the remaining 20 studies were used for the qualitative and quantitative analyses.Two studies,from Bere et al.35and Soligard et al.,36reported data from players in different age groups. The groups not meeting our age limit (>16 years) were excluded. Overlaps in injury data reporting were observed for Junge et al.24and Langevoort et al.,25resulting in the exclusion of the 2004 Handball Olympics data from Junge et al.24
3.2. Characteristics of included studies and methodological quality
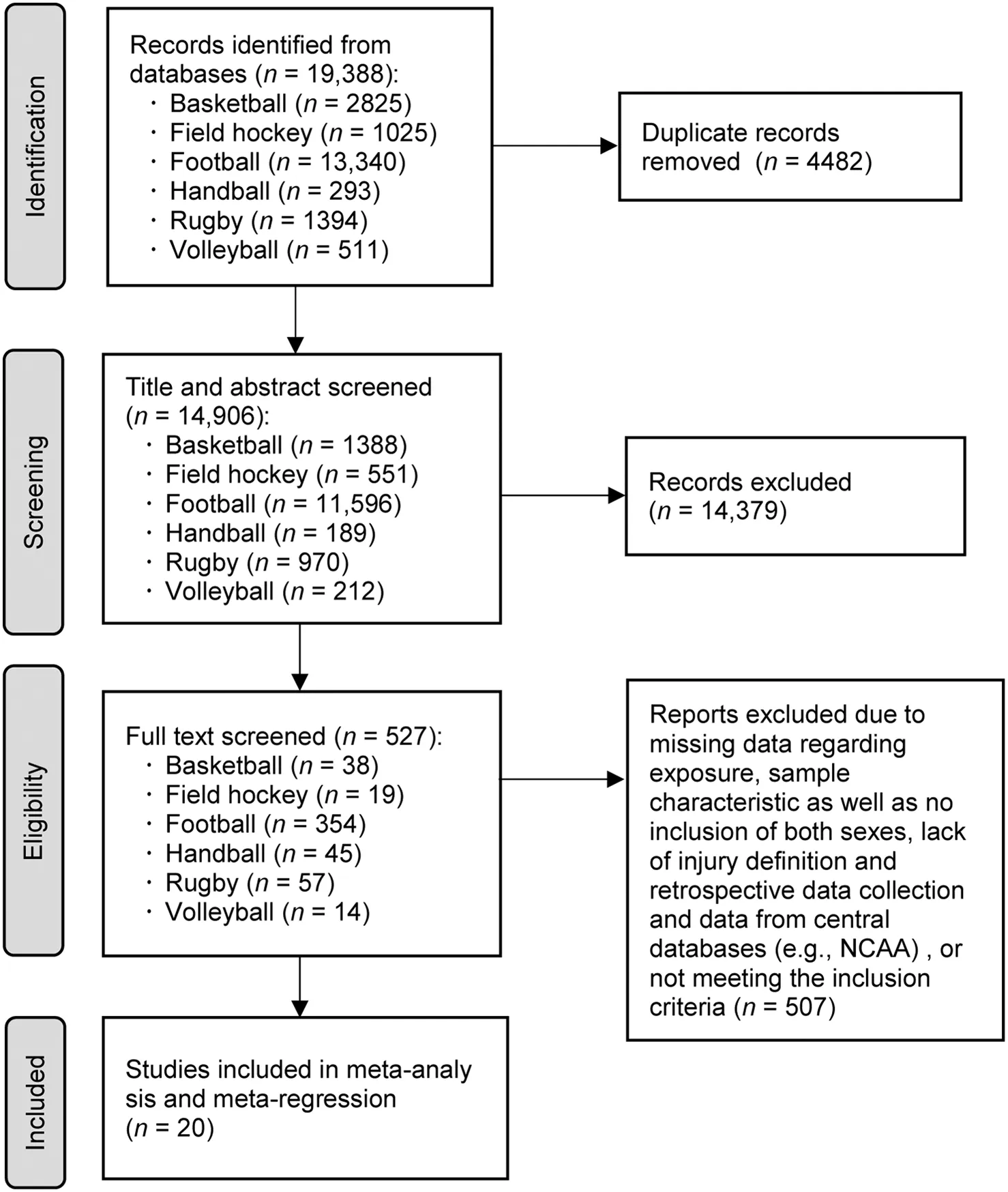
Fig.1. PRISMA flow diagram of the identification and selection of the studies included in this meta-analysis.NCAA=National Collegiate Athletic Association;PRISMA=Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Included studies collected injury and exposure data between 1998 and 2017 and were published between 2004 and 2020.Nine studies reported injury data from football,13,14,36-42 3 studies from rugby union/sevens,43-45 3 studies from handball,25,46,471 study from basketball,481 study from field hockey49, 2 studies from volleyball,35,50and 1 study from basketball and field hockey.24Thirteenstudiespresentedin-season data,13,14,37,40,42-50 and 7 studies presented tournament data(Olympic Games, World Cup, European Championships, and National Cup).24,25,35,36,38,39,41The majority of studies investigated senior athletes (n=16 studies),13,14,24,25,35,37,39-42,45-50 5 studies youth36,38,39,47,49and 2 studies collegiate43,44athletes.All studies collected data for both acute and overuse injuries.Seventeen studies13,14,24,25,37-43,45-50 collected data from a total of 8855 female and 16,317 male athletes. Three studies35,36,44had no information on the sample size but reported injury rates in a manner consistent with our methods. Exposure data in all included studies were presented in hours.The reported exposure time for match and training together was 391,250 h(match exposure:107,915 h)for female players and 832,383 h(match exposure:191,316 h)for male players.Injury was defined by time loss in 13 studies13,14,37,38,40-43,45,47-50 and by medical attention in the remaining 7 studies.24,25,35,36,39,44,46Details regarding sample characteristics,exposure,and injury data for each study are summarized in Supplementary Table 2.
The quality score of the 20 studies ranged between 19 and 28 out of a maximal 30 points, with a mean § SD score of 24.5 § 2.7 points. The 9 studies published before 2010 had a mean quality score of 25.3 points,and the 11 studies published after 2010 had a mean quality score of 24.0 points. The complete quality scores for each study are presented in Supplementary Table 1.Visual inspection of funnel plots(Supplementary Figs.1 and 2)indicated no publication bias.
3.3. Injury incidence,meta-analyses,and meta-regression
3.3.1. Overall injuries
The reported incidence of overall(match and training)injuries varied between a minimum of 2.4 (females)50and 3.8(males)50per 1000 h in volleyball and a maximum of 40.8(females)45and 45.0 (males)45per 1000 h in rugby. Six studies13,14,37,38,41,42of football players reported overall injury rates between 4.6 and 9.9 per 1000 h for female players and between 6.4 and 9.5 overall injuries per 1000 h for male players. Two studies43,45of rugby reported overall injury rates of 20.1 and 40.8 per 1000 h for females and 17.7 and 45.0 per 1000 h for males. No multiple overall injury data were available for any of the other sports.47-50
The overall injury IRR between females and males was 0.86(95%CI:0.76-0.98;I2=73%),indicating a higher injury rate in male players (Fig. 2). The meta-analysis of subgroups showed that this effect was statistically significant for football(IRR=0.75, 95%CI: 0.71-0.80; I2=0%) and handball(IRR=0.76, 95%CI: 0.61-0.96; I2=0%) but not for the other team sports.
The meta-regression confirmed that the pooled IRR is partially moderated by the type of sport. Basketball (regression coefficient estimate=0.835, 95%CI: 0.562-1.109; z=5.99;p<0.001)and rugby(estimate=0.255,95%CI:0.028-0.482;z=2.20; p=0.028) significantly differed from football in the sex-specific distribution of injury rates (reference level in the model). Moreover, no significant moderators of the IRR between females and males were found for tournament vs.season (estimate=-0.263, 95%CI: -0.660 to 0.134; z=-1.30;p=0.194), age level (estimate=-0.025, 95%CI: -0.334 to 0.283; z=-0.161; p=0.872), and study quality (estimate=-0.030, 95%CI: -0.165 to 0.105; z=-0.440;p=0.660).
3.3.2. Match injuries
Seventeen studies13,14,24,25,35-39,41,43,44,46-50 reported match injury incidences with a range of 4.250to 110.525per 1000 h for females and 3.850to 113.025per 1000 h for males.The lowest incidences in both sexes were found in volleyball50and the highest in handball.25Seven studies13,14,36-39,41 of football players reported between 13.937and 91.839match injuries per 1000 h for female players and between 22.137and 83.439match injuries per 1000 h for male players.In 3 studies of handball,25,46,47the match injury incidences were between 13.047and 110.525per 1000 h for females and 17.247and 113.025per 1000 h for males.In 2 rugby studies,43,44the match injury incidences were 17.044and 55.643per 1000 h for females and 16.944and 46.443per 1000 h for males. In 2 volleyball studies,35,50the match injury incidences were 4.450and 12.235per 1000 h for females and 3.850and 11.735per 1000 h for males.In 2 field hockey studies,24,49the match injury incidences were 9.649and 14.524per 1000 h for females and 9.549and 46.824per 1000 h for males. In 2 other basketball studies,24,48reported injuries per 1000 h were 55.348and 100.124for females and 46.848and 96.524for males.
The pooled IRR(0.90,95%CI:0.78-1.03;I2=80%)for all sports showed no significant differences between sexes(Fig. 3). Furthermore, the subgroup analysis identified no significant sex-specific differences in the match injury rates in any single team sport. No significant moderators were found for the match injury IRR between females and males in the meta-regression analysis.
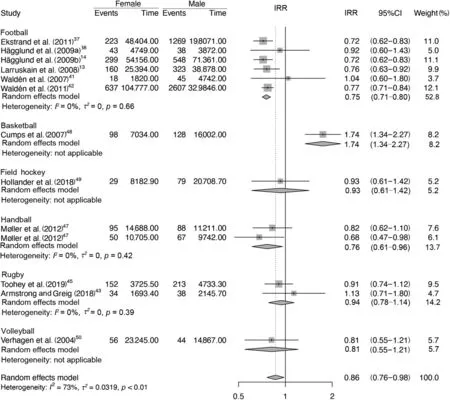
Fig.2. Forest plot with the pooled incidence rate ratios(IRRs)and 95%confidence intervals(95%CI;lower limit to upper limit)of the female vs.male comparisons for overall injuries.TagedEnd
3.3.3. Training injuries
The injury incidence rates during training in all team sports ranged between 1.550and 5.843per 1000 h for females and 1.338and 5.343per 1000 h for males. Five studies13,14,37,38,41of football players reported between 2.341and 3.814training injuries per 1000 h for female players and between 1.338and 4.738training injuries per 1000 h for male players. Two studies46,47with data on training injuries in handball reported an incidence of 2.147and 4.146training injuries per 1000 h for females and 3.246and 3.447per 1000 h for males.No multiple training injury data were available for any of the other sports.43,48-50
The meta-analysis (Fig. 4) resulted in a pooled random effect IRR of 0.87(95%CI:0.75-1.00;I2=32%).In the metaregression analysis, injury definition was the only significant moderator (estimate=-0.57, 95%CI: -1.12 to -0.01;z=-2.00; p=0.045) of sex-specific differences in training injuries.
3.3.4. Severe injuries
Eight studies13,14,24,25,35,37,38,41reported data for severe injuries. The incidence rate ranged from 0.637to 3.624per 1000 h for female players and from 0.714,37to 7.224per 1000 h for male players. The pooled IRR among all team sports was 0.96(95%CI:0.77-1.20;I2=0%).Most included studies with severe injury data concerned football players and showed an average incidence of 0.8 in both sexes (female: 0.637-1.641per 1000 h;male:0.737-2.541per 1000 h).No subgroup analysis or meta-regression was performed for the other sports because of the low number of studies.
3.3.5. Location of injuries
Nine studies13,14,24,25,37,41,44,45,49reported the incidence of thigh and foot injuries, and 10 studies13,14,24,25,37,41,43-45,49 reported head, upper extremity, trunk, hip/groin, knee, and ankle injuries. The IRR and meta-regression data for the various body locations in all team sports are shown in Table 1.The pooled IRR showed significantly more injuries in male players than female players for the upper extremity (IRR =0.75, 95%CI: 0.57-0.99; I2=30.3%), hip/groin (IRR = 0.60,95%CI: 0.41-0.88; I2=41.5%), thigh (IRR = 0.69, 95%CI:0.58-0.81; I2=0%), and foot (IRR = 0.64, 95%CI:0.46-0.88;I2=0%).
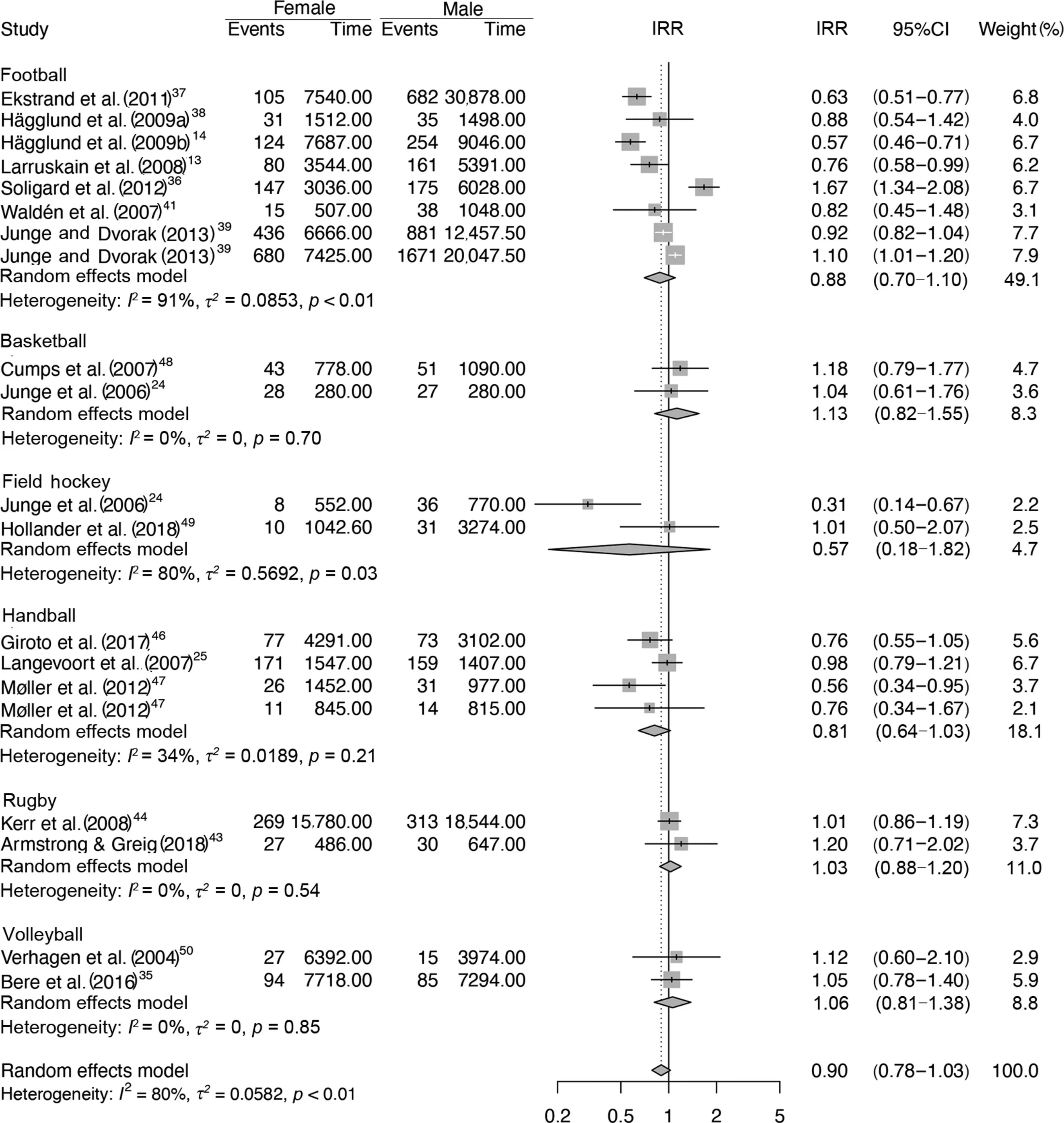
Fig.3. Forest plot with the pooled incidence rate ratios(IRR)and 95%confidence intervals(95%CIs;lower limit to upper limit)of the female vs.male comparisons for match injuries.TagedEnd
The meta-regression identified age level (senior vs. youth/collegiate) as a significant moderator for the hip/groin IRR(estimate=-2.00, 95%CI: -3.72 to -0.20; z=-2.18;p=0.029). The type of sport was a significant moderator for upper extremity (football vs. field hockey: estimate=1.08,95%CI: 0.04-2.11; z=2.04; p=0.041), trunk (football vs.rugby: estimate=1.42, 95%CI: 0.37-2.46; z=2.67; p=0.008),and hip/groin injuries (football vs. rugby: estimate=1.57,95%CI:0.67-2.47;z=3.43;p=0.001)(Table 1).No volleyball studies were included in the meta-regression analysis.
3.3.6. Injury types and diagnosis
Dataonsprainswereavailablein9 studies14,24,25,37,41,43-45,49 and on strains in 8 studies.14,24,25,37,41,43,44,49The injury rate for both sexes was reported for concussion in 9 studies,14,24,25,37,40,41,43,44,49the ACL rate in 3 studies,13,14,42ankle sprains in 2 studies,37,43and Achilles tendon injuries in 2 studies.13,41Hamstring injuries were not included in the meta-analysis because they were reported in only 1 study.37The pooled IRR indicates a significantly higher rate of ACL injuries(IRR=2.15,95%CI:1.27-3.62;I2=0%)in female compared to male athletes (Table 2). No significant differences between sexes were identified for the other injury types. In the meta-regression analyses (Table 2) for sprains and concussions, no significant moderators for the IRR between females and males were found. No volleyball studies were included in the meta-regression analysis.
4. Discussion
This meta-analysis compared the injury incidence between female and male players in 6 team sports. Only studies with injury data for both sexes were included, and their IRRs were used for data pooling. All of the 20 studies finally included had moderate to high methodological quality. The results emphasize the presence of sex-specific differences and,importantly,the direction of these effects differs depending on injury characteristics. Male team-sport players have a higher rate of overall, upper extremity, hip/groin, thigh, and foot injuries compared to female players. There is also a trend showing more match and training injuries in males compared to females,although the IRR was not significant.Female athletes showed a 2.15 times higher rate of ACL injury than males,but no significant sex differences were found for sprains, strains,concussions, ankle sprains, or Achilles tendon injuries. To date,almost no meta-analytic data exist for sex-specific differences of sports injuries.For running injuries,a meta-regression analysis10showed significantly more bone-stress injuries in females,whereas male runners were at higher risk for Achilles tendinopathies. This emphasizes our findings that suggest a different distribution of specific injury types and locations between sexes. However, contrary to Hollander et al.,10we also found significant differences between females and males in other injury categories.
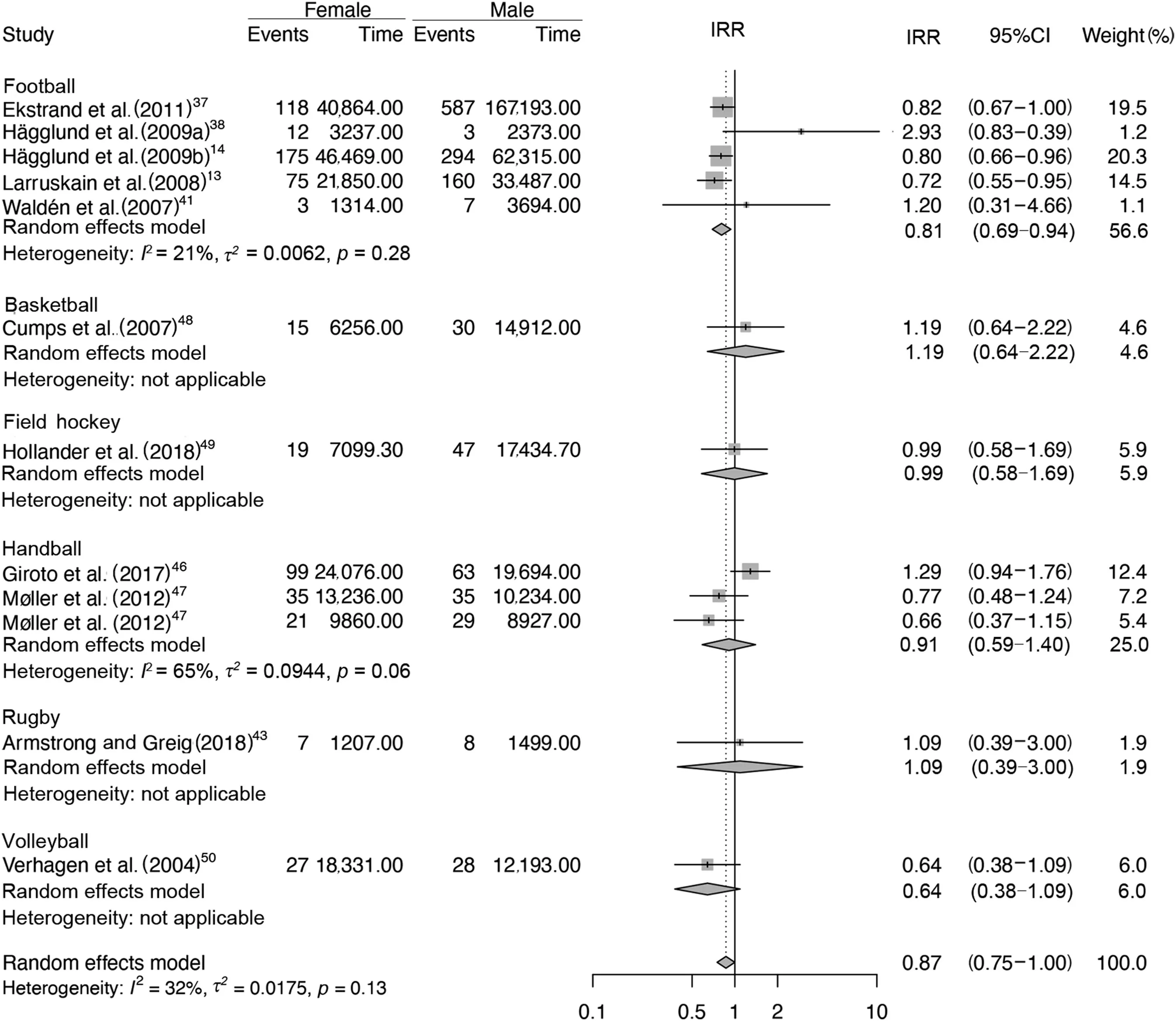
Fig.4. Forest plot with the pooled incidence rate ratios(IRRs)and 95%confidence intervals(95%CIs;lower limit to upper limit)of the female vs.male comparisons for training injuries.
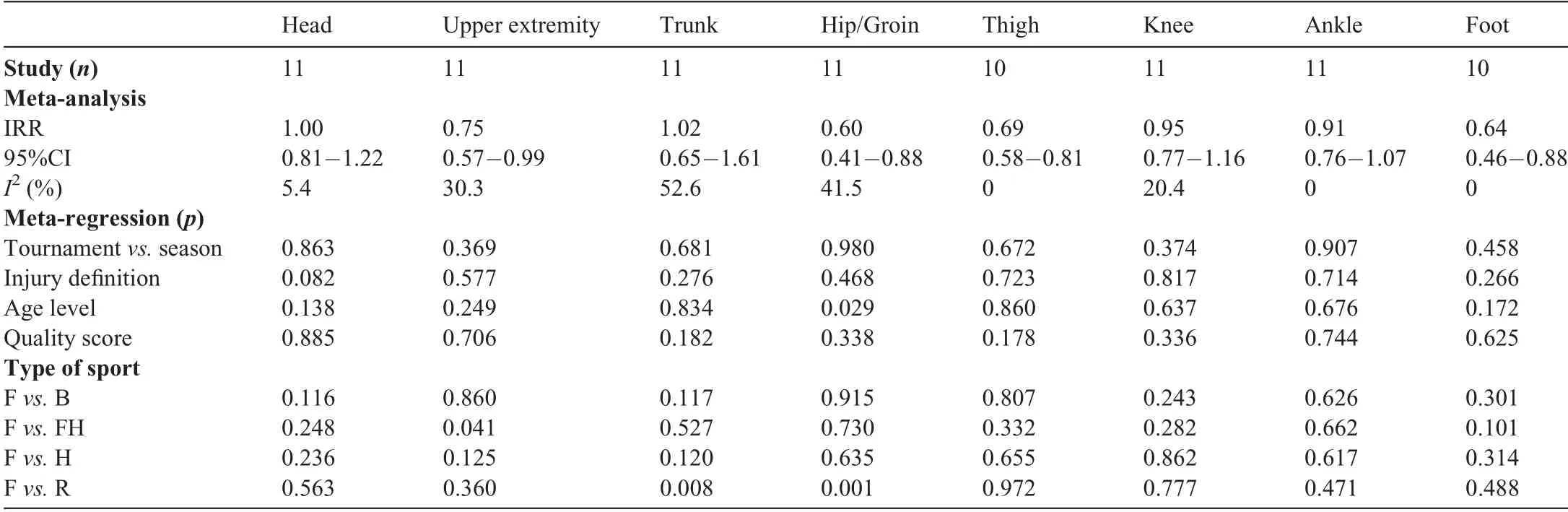
Table 1 Pooled IRR,95%CI,I2,and meta-regression p values for specific body locations.
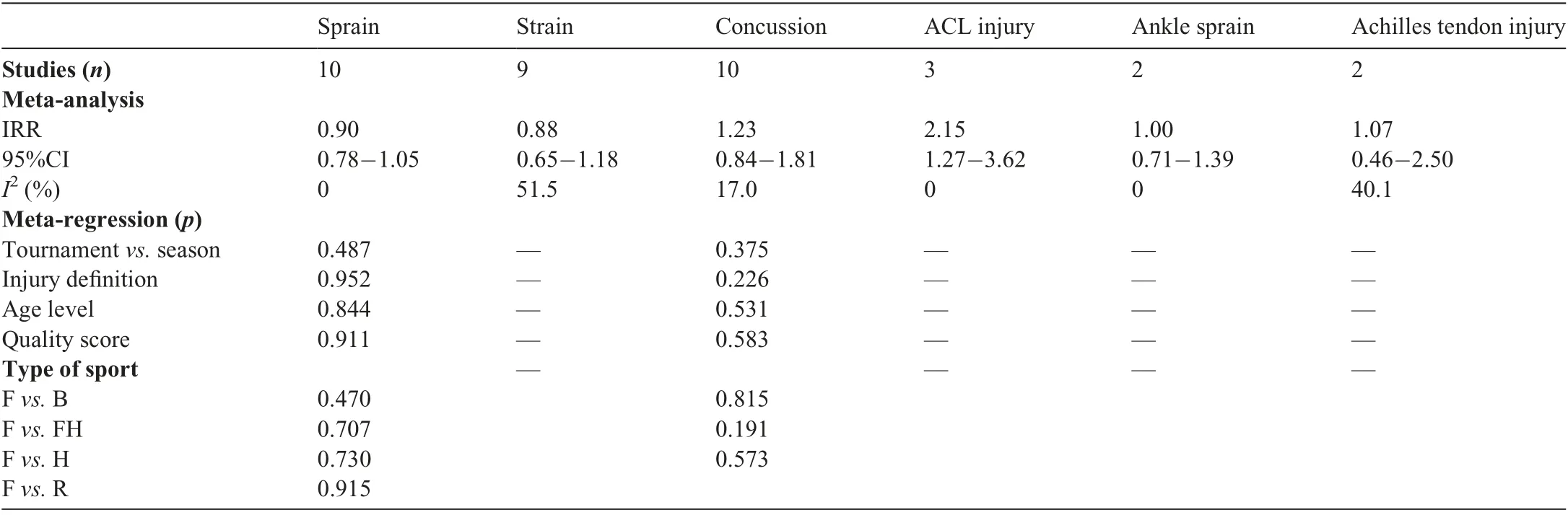
Table 2 IRR,95%CI,I2,and meta-regression p values for specific injury types.
4.1. Overall,match,and training injuries
The results show a significantly higher incidence of total injuries in male than in female players. Although there was a tendency toward higher rates in male players for match and training injuries, the rate ratio did not reach statistical significance.Not all included studies reported data on overall,match,and training injuries,which may have contributed to the different findings.Sixteen studies reported match injuries,but only 10 studies were available for training and overall injuries.Potential reasons for the higher overall injury rate in male team-sport players include multiple modifiable and nonmodifiable risk factors.51,52One explanation could be a difference in risk-taking behavior between sexes. In adolescent sports,female athletes have shown higher levels of perceived risk but lower levels of actual risk than male athletes.51In particular,the perceived risk (but not the actual risk) seems to be negatively associated with an increased rate of injury in sports.51,53Another possible explanation could be different loads in match/training or a different sport-specific performance of female and male players. For example, male football players were reported to cover more distance at higher speed thresholds than female players during a match.52
When taking a look at the sex-related rate ratio of the specific sports,the greater overall injury rate in male players compared to female players was confirmed for football and handball but not for the other team sports. However, because of the limited number of included studies, the data presented in the nonfootball sports should be viewed with caution.32,54For basketball, volleyball, and field hockey, only 2 or fewer studies were available, indicating a limited generalizability of the injury rate ratios. Data of single epidemiological studies depend heavily on the surveillance methods and/or circumstances and are of limited comparability. The methodological heterogeneity in injury surveillance studies and low comparability of data have been critically discussed elsewhere.1,12
4.2. Injury types and diagnoses
The significantly higher ACL injury rate in female players supports previous findings.9Possible explanations are greater neuromuscular-control deficits in females; an imbalance of muscle agonists,antagonists,and/or synergists;proprioceptive deficits;55or hormonal status.56,57
We found no significant differences between sexes for concussion rates. This is different from other studies and reviews that have reported a higher rate in females.8,58This may be explained by our restrictive study-selection criteria and the inclusion of only high-level team-sport athletes. The concussion risk seems to depend on sport-specific situations, such as tackling in male professional rugby,59and is associated with poor sleep quality and insomnia.60No plausible explanation exists for potential sex-specific differences.61However, it should be noted that greater concussion-reporting intentions in female athletes than in male athletes could influence study findings.62
The absence of sex differences in ankle sprains is in agreement with the literature review articles of Beynnon et al.63and Delahunt and Remus;64yet it contradicts the findings of the systematic review and meta-analysis done by Doherty et al.,7who showed that pooled incidence rates were twice as high in females as in males. These meta-analyses (ours and that of Doherty et al.7), however, are hard to compare due to the different study-inclusion criteria. Doherty et al.7included all available ankle-sprain studies, without a clear focus on a specific (sports) population. In our meta-analysis, only 2 studies with ankle sprain incidence rates37,43—in football and rugby players,specifically—met the narrow inclusion criteria.
4.3. Moderators of sex differences in injury rates
The type of sport, injury definition, age level, competition(tournament vs. season), and methodological quality score were considered to be potential moderators of sex differences in injury rates in our meta-regression analysis. The results show that the type of team sport significantly influences the rate ratio of overall,upper-extremity,trunk,and hip/groin injuries.For example,in contrast to the pooled data,Cumps et al.48showed a far higher overall injury incidence rate in female than in male basketball players.Furthermore,the sex differences were not present in the studies of rugby players, whereas the majority of other studies included football players and supported the higher injury rate in male athletes. Although some team sports were clearly under-represented in this meta-analysis, the results indicate that sex should not be considered a general risk factor65for overall sports injuries but should be viewed in interaction with the type of sport.Nonetheless,more surveillance studies are needed in sports other than football and rugby in order to strengthen the evidence.
The age level played no role in sex differences in most of the injury outcomes except for hip/groin injuries.Only 2 rugby studies43,44of collegiate athletes contributed to the differences in the sex-specific rate ratio for hip/groin injuries, so more research is needed in order to confirm or refute this finding.The training injury rate was significantly moderated by the injury definition, with more time-loss injuries in males and more physical complaints in females.One possible reason may be found in different reporting intentions. Female players seem to be more motivated to report minor(no time-loss)injuries than males.62Another explanation for the reported number of time-loss injuries could be the influence of the higher total training exposure for males compared to females. However,more studies are needed in order to strengthen these assumptions.
The observed sex-specific distribution of injuries in all analyzed categories did not differ between tournaments vs. seasons, nor were they influenced by the methodological quality of the studies.
4.4. Limitations
Although the narrow inclusion criteria(e.g.,the inclusion of studies involving both sexes)helped to reduce the risk of bias,it produces a certain limitation at the same time. Numerous surveillance studies of various team sports that had large study samples and comprehensive data had to be excluded because they examined males or females exclusively or did not report sufficient data. This reduced the data in our meta-analysis,thereby weakening the evidence base,especially in nonfootball team sports. Some comparisons had only a single study for 1 team sport. This problem was addressed by displaying all-team-sports IRR alongside the sport-specific IRR. The low number of included studies also limits the findings on specific injury types, such as ankle sprains or Achilles tendon injuries.Moreover,only football studies were included in the meta-analysis for ACL injuries,which reduces the comparability of findings.
In almost half of the included studies, football dominated our meta-analysis and the reported findings.This may bias the conclusions for team sports in general and indicates the strong need for further studies with both female and male participants in nonfootball sports.
Another limitation is the heterogeneity of some estimates.Even though the influence of methodological specifications was reduced, and no strong moderator of risk ratio data other than type of sport was identified, the degree of inconsistency of the results across studies was substantial for overall(I2=73%) and match injuries (I2=80%). For the other injury outcomes, a nonrelevant or moderate heterogeneity was identified.30,32
Furthermore, although a number of moderators were tested for their potential influence on sex-specific differences, there might have been other influencing factors not considered in our meta-regression due to lack of information. For example,Ekstrand et al.37showed a different injury rate between female and male football players on different playing surfaces.
It should also be noted that the proportion of match to total exposure hours was slightly higher for females than males(27%vs. 23%), which may have influenced the overall injury incidence. Other limitations include the use of a nonvalidated scale for the methodological quality assessment.However,most of the categories were adopted from the standardized rating scales8,27,28and adapted for use in epidemiological injury studies.
5. Conclusion
The IRRs of our meta-analysis provide evidence for sex-specific differences in injury rates in team sports. Male players show higher rates for overall, upper extremity,hip/groin, thigh, and foot injuries compared to female players,whereas females have more ACL injuries. The overall, upper extremity, trunk, and hip/groin injury IRRs between sexes are moderated by type of team sport,indicating that sex should not be considered a general risk factor but be viewed in interaction with the specific sport. No or minor influence on the rate ratio was found for the age level,injury definition,or type of competition (tournament vs. season). Further epidemiological studies including both sexes in team sports other than football are needed in order to strengthen the evidence. Future research should also focus on sex-specific differences in other age groups(e.g., high school players), different playing level (e.g., recreational or military populations),and individual sports.
Authors’contributions
AZ did the study conception and design, data collection,statistics, and writing; KH, AJ, and SS participated in study conception and design and writing;ALR did the study conception and design, data collection, and writing; FN and DP helped with the data collection and writing;AG and JH did the statistics and writing. All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.04.003.
 Journal of Sport and Health Science2022年1期
Journal of Sport and Health Science2022年1期
- Journal of Sport and Health Science的其它文章
- Residual force enhancement in human skeletal muscles:A systematic review and meta-analysis
- Physical exercises for preventing injuries among adult male football players:A systematic review
- Interference screws vs.suture anchors for isolated medial patellofemoral ligament femoral fixation:A systematic review
- Incidence of injuries in professional snow sports:A systematic review and meta-analysis
- “When you’re down,stay down”:A lesson for all competitive alpine skiers supported by an ACL rupture measured in vivo
- Maximizing recovery time between knock-out races improves sprint cross-country skiing performance