
Incidence of injuries in professional snow sports:A systematic review and meta-analysis
2022-03-24 02:36XueLeiFuLinDuYiPingSongHongLinChenWngQinShen
Xue-Lei Fu,Lin Du,Yi-Ping Song,Hong-Lin Chen*,Wng-Qin Shen,*
a School of Medicine,Nantong University,Nantong 226001,China b School of Public Health,Nantong University,Nantong 226019,China
Abstract
Keywords: Incidence;Injury;Skiing;Snowboarding
1. Introduction
The Winter Olympic Games will be hosted by China in 2022 and are expected to mobilize millions of people to embrace winter sports.Recreational alpine skiing is one of the most popular winter sports, attracting several hundred million people worldwide.1,2In the United States, approximately 17 million people participate in snow-skiing and snowboarding every year.3These 2 snow sports often share the same slopes and facilities.4Generally, skiing-related injuries are the outcome of a complex multiple interaction of internal risk factors,including age,sex,and skill level,as well as external risk factors, including the environment and the ski-boot-binding equipment.5-7
An analysis from Australia reported that skiing and snowboarding have the highest incidence of injury among snow sports.8It is estimated that emergency departments in the United States treat 200,000 injuries related to skiing and snowboarding annually, and a majority of patients are adults.9,10Although most patients are discharged on the same day, roughly 7000 require hospitalization each year.9Skiers are often admitted to the floor or the operating room, while snowboarders are frequently sent to the intensive care unit.11Experienced skiers and snowboarders are more likely to sustain an injury resulting from jumps, while accidental falls are the most common cause of injury among beginners.12,13
The majority of the available data suggests that experienced athletes tend to gain additional health benefits,14-17 but athletes are still exposed to great risks of injury. Risk of injury is perceived as an inherent part of elite sports, because athletes always try to push the limits of performance.18Bianco et al.19reported that elite skiers are likely to gamble with their health to avoid missing an important competition or losing a spot on the team.
Little is known about injury incidence in professional snow sports. The availability of large datasets that combine clinical information with health outcomes would optimize prevention for individuals and populations,20and identifying the incidence of injuries would provide information for applying preventive measures. Therefore, a systematic meta-analysis was performed to estimate the incidence of injuries in professional snow sports. The secondary aim was to determine the injury incidence as it relates to location, severity, type, cause, sport discipline, the sex of participants, and events leading to an injury.
2. Methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)guidelines.21
2.1. Search strategy
Three electronic databases (PubMed, Web of Science, and MEDLINE) were systematically searched from inception to April 2020. The searches combined terms related to “skiing”,“alpine skiing”, “cross-country skiing”, “freestyle skiing”,“Nordic skiing”, “ski jumping”, “snowboarding”, “injury”,“professional”,and“elite”.The terms were adjusted according to individual database specifications(Supplementary Table 1).We limited the search to studies that were available in English.The reference lists of retrieved articles were hand searched for additional studies.
2.2. Study selection
Studies eligible for inclusion had to fulfill the following criteria: (1) studies that included participants who were professional skiers or snowboarders engaged in professional national or international competitions or who had studied at elite national sports schools after passing a strict entrance examination, (2) studies that reported injury incidence (the number of new injuries occurring in the population during a specific duration of time)among professional athletes or that provided sufficient data for calculation, (3) studies that were original research articles,and(4)studies that went through an independent peer-review process.Studies that did not meet the following criteria were excluded from our meta-analysis: (1) case reports,intervention studies,qualitative studies,editorial commentaries,systematic reviews,or abstracts and(2)studies that did not report measures of athlete-days or follow-up duration.
Two reviewers (XLF and LD) initially screened the titles,abstracts, and reference lists of studies based on the selection criteria. The full-text versions of articles were retrieved when titles and abstracts met the selection criteria. Any discrepancies regarding the selection process were discussed by the 2 reviewers, and a third external reviewer (HLC) was consulted if consensus could not be reached.
2.3. Data extraction
The following information was independently extracted by 2 reviewers (XLF and LD): (1) general study characteristics(authors, publication year, and study design), (2) description of the surveyed population(sport discipline,female/male,age,and body mass index(BMI)),(3)epidemiological data(injury,athlete-days,distribution of injuries by location,severity,type,cause, sex, and events leading to an injury). For studies that did not provide the number of athlete-days, it was approximated from follow-up duration and sample size.
2.4. Risk of bias assessment
Quality assessment was conducted according to the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.22This tool assesses items including study population,exposure, and outcome measures, whether the exposure was assessed prior to outcome measurement,whether the timeframe was sufficient and the number of participants lost to follow-up after baseline. Two reviewers (XLF and YPS) independently assessed included studies and recorded the number of checklist items fulfilled. Discrepancies in assessment were resolved by discussion. Study quality of each study was assessed and reported as poor (score of 0‒5), fair (score of 6‒9), or good(score of 10‒14).
2.5. Statistical analysis
Injury incidence in ea ch study was calculated(i.e.,the number of injuries divided by 1000 athlete-days).Where the number of injuries equaled zero, 0.5 was substituted to allow for stable calculations in meta-analysis.The I2statistic was used to quantify heterogeneity and describe the proportion of total variation resulting from heterogeneity.23A random effect model was applied where statistically significant heterogeneity(I2> 50%)was detected;otherwise,a fixed effect model was used.
Pooled estimates of injury incidence were summarized in forest plots for the following groups: (1) overall injury incidence, (2) location of injuries (upper extremity vs. lower extremity vs.head/neck vs.trunk),(3)severity of injuries(slight(1-3 days) vs. mild (4-7 days) vs. moderate (8-28 days) vs.severe (>28 days)), (4) type of injuries (fracture vs. sprain vs.strain vs.meniscus and cartilage vs.contusion vs.impingement vs. laceration, abrasion, and skin lesion vs. muscle cramps and spasm vs. other), (5) cause of injuries (overuse vs. contact vs.non-contact vs.other),(6)sport discipline of injuries(alpine skiing vs.freestyle skiing vs.Nordic skiing vs.snowboarding),(7)sex-specific injuries,and(8)training vs.competition injuries.
Publication bias was detected using funnel plot and Egger’s test. The possible influence of the following variables on the model was analyzed through meta-regression:median registration period, mean age, and mean BMI. In addition, time trends were represented by median registration period. For statistical tests, a significance level of p < 0.05 was applied throughout. Injury data extracted from the included studies were analyzed using STATA Version 12.0(Statacorp.,College Station,TX,USA).
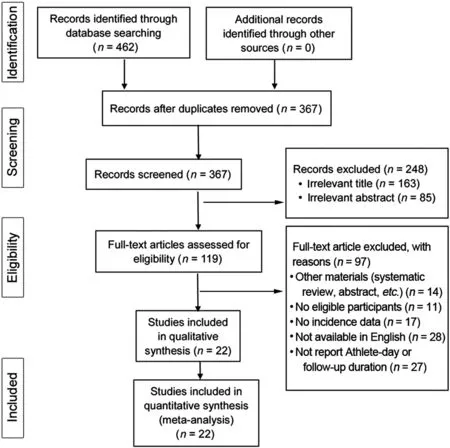
Fig.1. Flow diagram for identifying studies.
3. Results
3.1. Descriptive characteristics of the studies
As shown in the flow diagram(Fig.1),the electronic search yielded 367 nonduplicate articles.The full texts of 119 studies were retrieved and assessed for eligibility, of which 97 were subsequently excluded. Thus, 22 studies between 2005 and 2020 were included in the study. Participants included a total of 12,335 professional skiers or snowboarders.24-45 The mean age ranged from 11.7 years to 23.0 years, and the mean BMI ranged from 17.9 kg/m2to 22.2 kg/m2overall. A total of 1624-35,38,39,42,45 of the included studies had a prospective study design, and 636,37,40,41,43,44studies used a retrospective study design. The detailed data are presented in (Supplementary Table 2). A total of 14 studies
24,26-28,32-36,38,39,42,43,45 were considered to be of good quality, 7 studies25,29,31,37,40,41,44were of fair quality, and 1 study30was of poor quality (Supplementary Table 3).
3.2. Overall injury incidence
Of the included 22 studies, the injury incidence of snow sports varied greatly. The overall incidence was 3.49 injuries per 1000 athlete-days (95% confidence interval (CI): 2.97‒4.01) from random effect models. The level of heterogeneity in the analysis was high(I2=97.3%;p=0.000).Fig.2 displays a summary of the overall injury incidence.Significant publication bias was found by Egger’s test (p=0.000) and visual inspection of the funnel plot asymmetry. Neither the registration period (p=0.079), the age (p=0.500) nor BMI(p=0.392)had an impact on injury incidence.
3.3. Location of injury
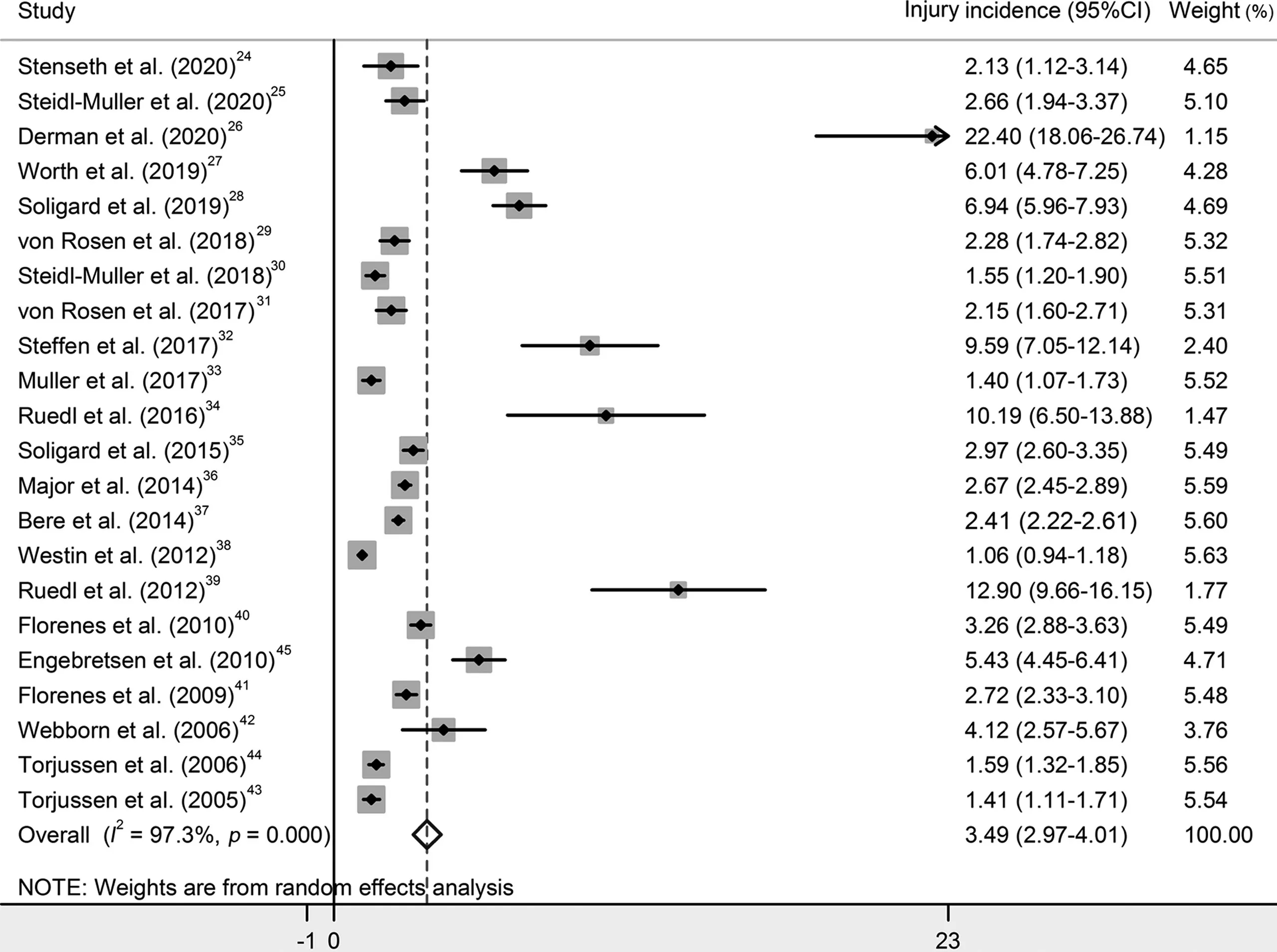
Fig.2. Forest plot for the overall injury incidence in professional snow sports.95%CI=95%confidence interval.
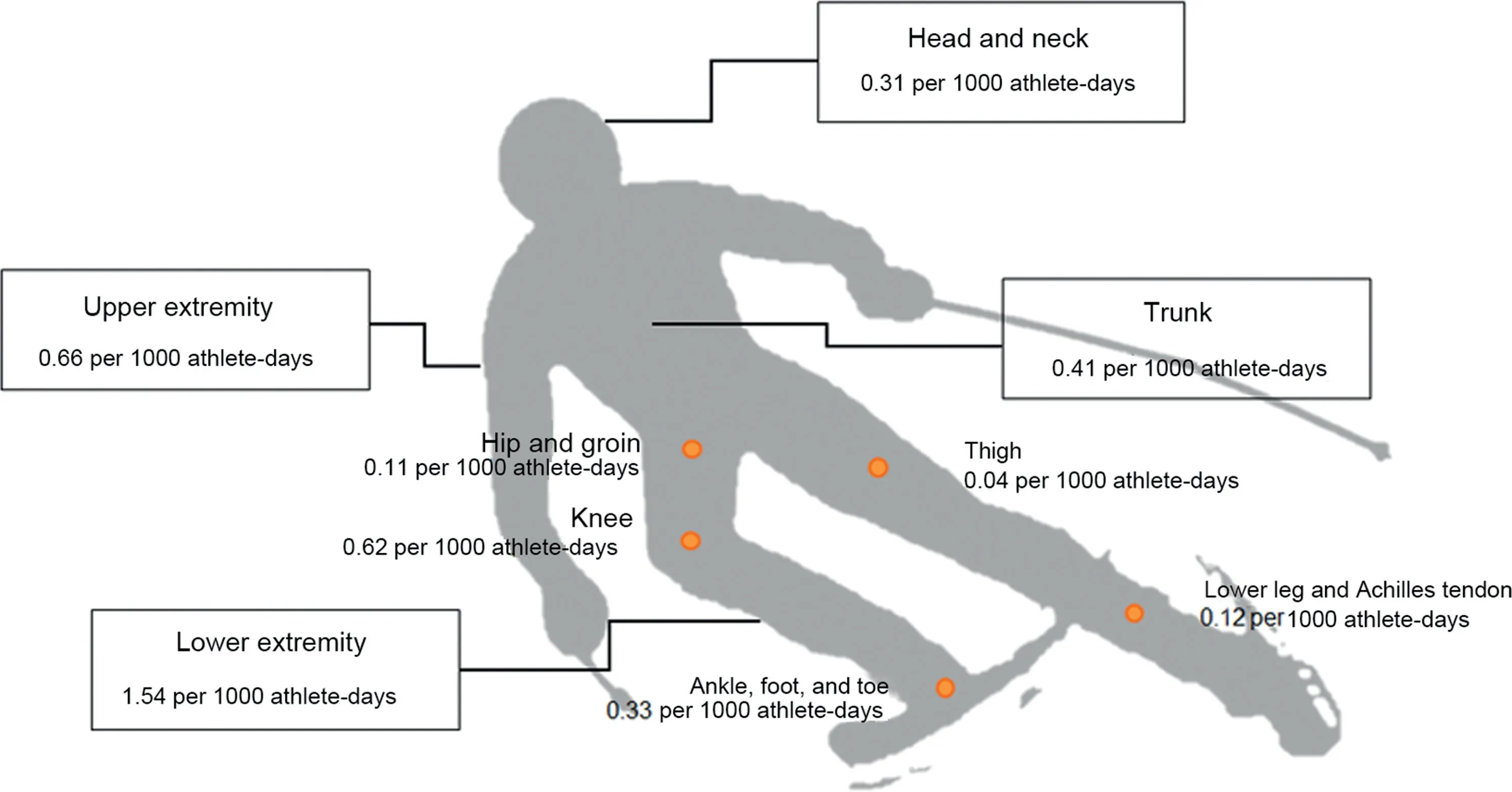
Fig.3. Injury incidence rates by location of injuries.
A total of 17 studies reported location of injuries.24,27-29,31-34,36-41,43-45 Lower extremity injuries had the highest injury incidence(1.54 per 1000 athlete-days,95%CI:1.24-1.84; I2=95.4%), followed by upper extremity (0.66 per 1000 athlete-days, 95%CI: 0.51-0.82; I2=92.3%), trunk (0.41 per 1000 athlete-days,95%CI:0.30-0.51;I2=90.4%),and head and neck injuries (0.31 per 1000 athlete-days, 95%CI:0.21-0.41;I2=90.2%).Additionally,15 studies reported data of lower extremity injuries.24,27-29,31,32,34,36,38-41,43-45 The incidence was represented in descending order: knee (0.62, 95%CI:0.47-0.78; I2=88.5%), ankle, foot, and toe (0.33, 95%CI:0.22-0.44; I2=90.5%), lower leg and Achilles tendon (0.12,95%CI: 0.07-0.17; I2=81.0%), hip and groin (0.11; 95%CI:0.06-0.16; I2=78.9%), and thigh (0.04, 95%CI: 0.02-0.07;I2=43.6%)(Fig.3).
3.4. Severity of injury
A total of 7 studies provided information on severity of injuries.24,30,33,37,38,40,41Incidence rates of slight, mild,moderate, and severe injuries were 0.26 (95%CI: 0.19‒0.33;I2=45.7%), 0.31 (95%CI: 0.14‒0.48; I2=95.8%), 0.57(95%CI:0.51‒0.64;I2=20.6%),and 0.59(95%CI:0.35‒0.82;I2=94.4%)per 1000 athlete-days,respectively.(Fig.4).
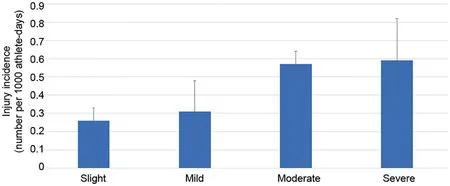
Fig.4. Injury incidence rates by severity of injuries.
3.5. Type of injury
A total of 6 studies were included in the pooled analysis.24,28,32,34,39,45The most common type of injury was contusion 1.82 (95%CI: 1.01‒2.63; I2=84.7%), followed by sprain 1.48 (95%CI: 1.07‒1.89; I2=41.3%); other 1.17(95%CI: 0.60‒1.74; I2=80.3%); strain 0.66 (95%CI: 0.33‒1.00;I2=59.2%);fracture 0.57(95%CI:0.38‒0.76;I2=7.8%);laceration, abrasion, and skin lesion 0.26 (95%CI: 0.01‒0.52;I2=72.3%); meniscus and cartilage 0.16 (95%CI: 0.04‒0.28;I2=14.1%); and impingement 0.07 (95%CI: 0.00‒0.14;I2=0.0%) per 1000 athlete-days. No statistical significance was found for muscle cramps and spasm (Supplementary Fig. 1).
3.6. Cause of injury
The cause of injuries was reported in 5 studies.28,32,34,39,45Contact trauma was the most common cause of injury (3.20 per 1000 athlete-days, 95%CI: 1.32‒5.08; I2=94.2%) compared with the other causes. Incidence rates of non-contact trauma,overuse injuries,and other injuries were 2.38 per 1000 athlete-days (95%CI: 1.52‒3.24; I2=75.0%), 1.16 per 1000 athlete-days (95%CI: 0.59‒1.73; I2=74.0%), and 0.97 per 1000 athlete-days (95%CI: 0.48‒1.46; I2=68.9%), respectively(Supplementary Fig.2).
3.7. Sport discipline of injury
A total of 21 studies provided an indication of sport discipline of injuries.24,26-45 Freestyle skiing had the highest incidence rate(6.83 per 1000 athlete-days,95%CI:4.00‒9.66;I2=92.6%),followed by snowboarding (3.99 per 1000 athlete-days, 95%CI:2.86‒5.12;I2=95.6%),alpine skiing(3.57 per 1000 athlete-days,95%CI: 2.77‒4.36; I2=96.7%), and Nordic skiing (2.70 per 1000 athlete-days, 95%CI: 1.94‒3.46; I2=87.2%) (Supplementary Fig. 3). Fig. 5 and Supplementary Table 4 show the incidence proportion of injury location,severity,type,and cause.
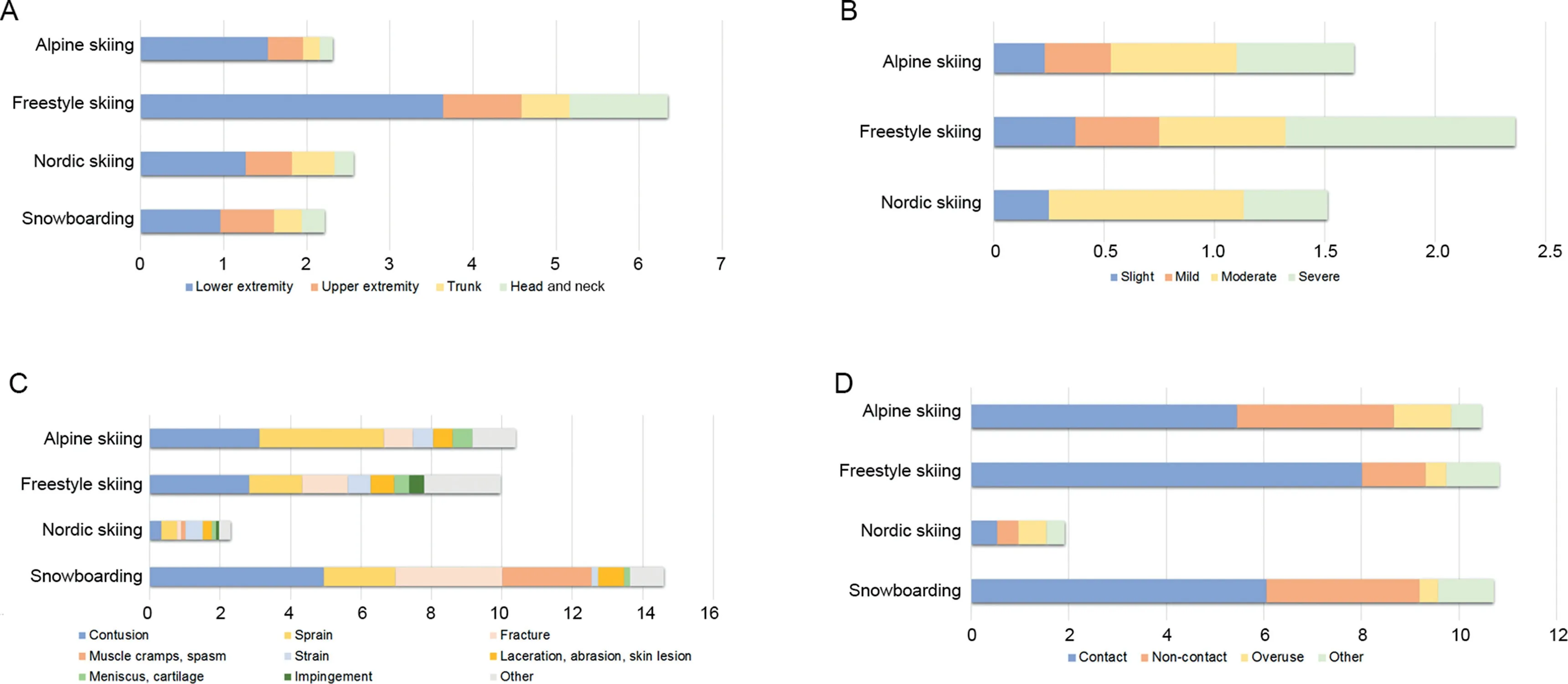
Fig.5. Incidence proportion of(A)injury location, (B)severity,(C)type,and(D)cause in different snow sports.
3.8. Sex-specific injury
A total of 10 studies reported injury data.28,31,32,34,37,39-42,45 The pooled incidence among males was 2.46 injuries per 1000 athlete-days (95%CI: 1.84‒3.07; I2=94.3%) (Supplementary Fig. 4),and among females was 2.10 injuries per 1000 athletedays (95%CI: 1.62‒2.58; I2=91.8%) (Supplementary Fig. 5).Fig.6 displays the time trend among males and females.
3.9. Training versus competition injury
A total of 15 studies in our analysis allowed us to compare training injuries and competition injuries.24,28,31,32,34-38,40-45 The incidence in training injuries(1.74 per 1000 athlete-days,95%CI:1.30‒2.18;I2=98.2%)was higher than in competition injuries (1.16 per 1000 athlete-days, 95%CI: 0.93‒1.39;I2=91.8%)(Supplementary Fig.6).
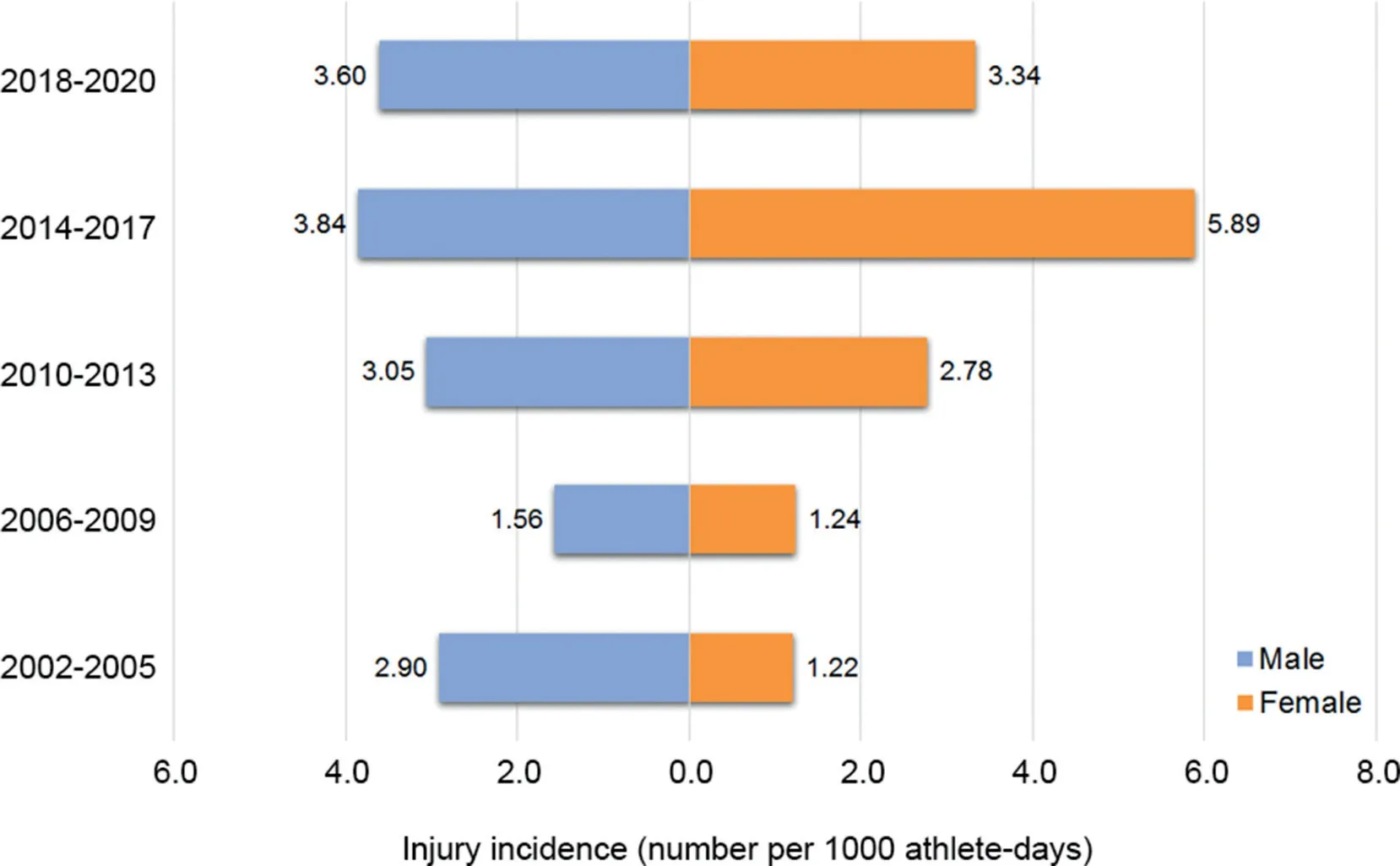
Fig.6. Injury incidence of time trends among males and females.
4. Discussion
We conducted an in-depth meta-analytic systematic review that assesses the injury incidence of professional snow sports. The pooled incidence of injuries across studies was 3.49 per 1000 athlete-days. Incidence rates for alpine skiing, freestyle skiing, Nordic skiing, and snowboarding were 3.57, 6.83, 2.70, and 3.99 per 1000 athletedays, respectively. A large body of research suggests that snowboard cross and halfpipe, aerial and halfpipe skiing and ski cross, and downhill alpine skiing events are present the greatest risk of injuries.28
Among all World Cup alpine skiing injuries,approximately 45%occur during competitions and only 25.1%during various forms of training on snow.46It is reported that almost all injuries occur while the alpine ski racer is turning or landing.47The most frequently injured body parts are the knee and the lower leg, with sprains of the anterior cruciate ligament being the most common type.46,48Interestingly, in our analysis we found that sprain injury and lower extremity injury were both common among alpine skiers, but detailed diagnoses of these injuries are too few to calculate injury incidence targeting a specific diagnosis. Additionally, knee pain and low back pain are reported to be the most frequent overuse injuries in alpine skiing.49
The results of our study found that the injury incidence of the head or neck in freestyle skiing was highest compared with the other snow sports.This finding is reasonable since all freestyle disciplines include aerial elements.50Moreover,our analysis has also shown that contact trauma is the main cause of freestyle skiing injuries.Randjelovic et al.51analyzed video of elite freestyle ski cross and pointed out that the main cause of injury was unintentional skier-opponent contact when jumping, bank turning and rolling. This observation confirms our findings to some extent.
Nordic skiing had the lowest injury incidence among all snow sports,with a rate of 2.70 per 1000 athlete-days.Previous studies have reported that the incidence rate among athletes competing in national squads versus professional clubs was 0.02 per 1000 athlete-days and 0.09 per 1000 athlete-days,respectively.52Our study aimed to determine global injury incidence, while the study by Ketterl52was conducted based on a specific region with a small sample size. Regional differences might help to explain why our study found a higher rate of injuries.
When elite snowboarders perform difficult maneuvers at high speed,the lower extremities often sustain amplified levels of force,and these athletes tend to suffer from injuries that are of greater severity.53As expected, lower extremity injuries were found to have the highest snowboarding-related injury incidence rate in our study. In the United States, incidence rates of lower extremity injuries presenting to emergency departments were reported to be 19 injuries per 1,000,000 person-years for snowboarders.54Emergency departments reported that there was an overall decrease in snowboardingrelated injuries from 2010 to 2016 in the United States.Among snowboarding injuries, the most prevalent injury type was fractures, with fractures of the upper extremities being most likely.55However,in our study fractures were the second most common injury type. Since our study was based on professional athletes rather than the general population, this difference might be expected.
In our study, snow sports injuries were more common among males. Male athletes are deemed to be “superhuman”,and their mental health is frequently overlooked.56Although athletes are more likely to experience depression compared with the general population,57conformity to traditional masculine gender norms and the stigma of mental illness often deters male athletes from seeking help.58,59This situation creates a vicious circle for the male athlete and influences his personal and sporting life, resulting in performance issues and in turn increasing the risk of injury.56
To improve performance, athletes must modify their training load, particularly increases in frequency, duration, and intensity. However, training and competition stress often lead to temporary decrements in physical performance and significant levels of fatigue,increasing the risk of injury.60When athletes are unable to cope with their stress,other emotions,such as chronic anger, hostility, confusion, depression, apathy, or anxiety, can occur. Additionally, more and more pressure to achieve elite sport performance has led to earlier specialization in snow sports and may contribute to an increased rate of overuse injury and sport burnout.61
An injury has a great impact on a professional athlete since it may portend the end of the athlete’s playing career.62Therefore,injury prevention plays an important role in elite sports.19It is particularly important for sports medicine physicians to have the information required to counsel athletes regarding safer snow sport participation and to recognize and treat their most common injuries. Additionally, clinicians and coaches should formulate appropriate exercise prescriptions to strengthen, maintain, or restore health and physical fitness for snow sport athletes.63These athletes should be informed about physical and mental health issues that may contribute or detract from excellence in performance and career longevity.
Our study has some weaknesses.First,there was substantial statistical heterogeneity across the included studies(I2=97.3%),which may be explained by the broad time frame that was covered across the included studies. Elite skiers or snowboarders from as early as 2001 through to 2018 were included as participants in the studies.Precise data on athletedays were not made available in many of the studies, so the true injury incidence was likely underestimated.Second,there was a risk of bias identified in several studies. A total of 6(27.3%) of the 22 included studies collected data retrospectively, which may have led to a risk of bias. Despite our systematic and comprehensive search,there was undeniably a risk for publication and language bias.
5. Conclusion
Our meta-analysis provides evidence that injury incidence in snow sports is very high, with a rate of 3.49 injuries per 1000 athlete-days. The lower extremities were the most frequently injured, and contusion was the most common type of injury. Contact trauma was the main cause of injuries. However,injury characteristics in different snow sports varied significantly.Our findings can inform the planning and provision of healthcare to elite skiers, snowboarders, and other snow sport participants. Clinicians and coaches should be aware of the common diagnoses and develop appropriate injury prevention strategies targeted specific snow sports. Future studies should focus on developing training programs for skiers and snowboarders in order to reduce the risks of long-term injury.
Acknowledgments
This study was supported by the Humanities and Social Sciences Research Planning Fund Project of the Ministry of Education (Project Number 20YJAZH007). It was also supported by the Social and People’s Livelihood Technology in Nantong City‒General Project(Project Number MS12019038).
Authors’contributions
XLF developed the search strategy, drafted the published protocol,led data extraction and critical appraisal,and drafted the final manuscript;LD contributed to the abstract screening,data extraction,critical appraisal of the data and critical review of the manuscript;YPS contributed to the design of the study,interpretation of the data analysis and statistical calculations and critical review of the manuscript;HLC and WQS contributed to the design of the study, acted as the guarantor of the study, developed the search strategy, performed, supervised and refereed data extraction, reviewed the data analysis, contributed to drafting the manuscript and critically reviewed the final manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found,in the online version,at doi:10.1016/j.jshs.2020.10.006.
 Journal of Sport and Health Science2022年1期
Journal of Sport and Health Science2022年1期
- Journal of Sport and Health Science的其它文章
- Residual force enhancement in human skeletal muscles:A systematic review and meta-analysis
- Sex differences in injury rates in team-sport athletes:A systematic review and meta-regression analysis
- Physical exercises for preventing injuries among adult male football players:A systematic review
- Interference screws vs.suture anchors for isolated medial patellofemoral ligament femoral fixation:A systematic review
- “When you’re down,stay down”:A lesson for all competitive alpine skiers supported by an ACL rupture measured in vivo
- Maximizing recovery time between knock-out races improves sprint cross-country skiing performance