
进行性肌阵挛性癫一例临床表型及基因突变分析
2018-05-10 03:47宋兴旺管玉青吴倩仪易咏红
中国现代神经疾病杂志 2018年4期
宋兴旺 管玉青 吴倩仪 易咏红
病例资料
患者 男性,43岁,主因发作性四肢抽搐20余年,加重伴行走不稳2年余,于2015年6月24日入院。患者20余年前无明显诱因突然倒地、肢体抽搐、意识障碍,持续数分钟至10余分钟后自行缓解,于1993和1994年各发作1次,分别发生于爆竹惊吓后和电视节目换台后;此后未出现上述症状而突发肢体抖动,持续时间不足1 s,无肢体抽搐和意识障碍,多于光刺激或受惊吓后诱发,并导致骨折2次;反复发作,光刺激后肢体抖动加重而日常需佩戴墨镜出行,未予正规抗癫治疗,呈进行性加重;2年前逐渐出现行走不稳,于2013年3月5日至我院门诊就诊,门诊以癫首次收入院。体格检查:行走基底宽,“一字步”不稳,余未见异常。实验室检查:血浆乳酸2.52 mmol/L(1.33~1.78 mmol/L),肌酶谱均于正常值范围。辅助检查:脑电图背景节律稍慢,清醒期可见弥漫性阵发性2.50~3.00 Hz中高波幅不规则δ波,予1、3、13、15、25和30 Hz的闪光刺激可见顶区、枕区和后颞区棘⁃慢复合波。肌电图和头部MRI未见明显异常。临床拟诊为进行性肌阵挛性癫,予以丙戊酸钠(德巴金)0.25 g/早和0.50 g/晚,左乙拉西坦(开浦兰)1 g/次、2次/d,吡拉西坦(脑复康)8 g/次、3次/d口服,共住院18 d,出院时无癫发作,日常无需佩戴墨镜,行走不稳未见明显改善。出院后遵医嘱按原剂量服用抗癫药物(AEDs),未再发生癫发作,但行走不稳呈进行性加重,无明显行走拖拽,伴四肢酸痛感,为求进一步诊断与治疗再次入院。患者自发病以来,精神、睡眠、饮食尚可,大小便正常,体重无明显变化。
既往史、个人史及家族史均无特殊。
入院后体格检查 体型消瘦,身高178 cm,体重63 kg,四肢可见轻度肌萎缩,四肢近端肌力为4~5级、远端正常,肌张力均正常,行走基底宽,“一字步”不稳,双侧指鼻试验、快复轮替动作、跟⁃膝⁃胫试验稳准,深浅感觉正常,四肢腱反射减弱,病理征阴性,脑膜刺激征阴性。
辅助检查 实验室检查:血浆肌酸激酶(CK)468 U/L(38~174 U/L),α⁃羟丁酸脱氢酶(HBDH)193 U/L(72~182 U/L),血浆乳酸2.67 mmol/L,其余指标均于正常值范围。影像学检查:头部MRI显示轻度脑萎缩。神经电生理学检查:肌电图显示左侧正中神经、尺神经、胫后神经和腓总神经运动感觉神经传导速度未见异常;左侧胫前肌可见自发性电位、运动单位时限增宽,左侧股内侧肌和小指展肌可见自发性电位、运动单位时限未见肯定增宽或缩窄,提示神经源性损害。视频脑电图(VEEG)显示,清醒安静闭目状态下背景可见持续弥漫性3.00~3.50 Hz δ波,偶见少量θ波,并夹杂大量β波,睁眼时上述节律抑制不完全,清醒期可见弥漫性阵发性2.50~3.00 Hz中高波幅不规则δ波,持续1~2 s,可夹杂单个尖波,尤以双侧额颞区显著;过度换气未见局灶性慢波活动和异常放电;予1、3、13、15、25和30 Hz闪光刺激可诱发以后头部尤其是枕区为主的棘⁃慢复合波,且于闪光刺激停止后仍可见(图1)。
肌肉病理学检查 患者行股四头肌外侧肌组织活检术,行HE染色、改良Gomori三色(MGT)染色、高碘酸⁃雪夫(PAS)染色、油红O(ORO)染色、还原型辅酶Ⅰ四氮唑还原酶(NADH⁃TR)染色、琥珀酸脱氢酶(SDH)染色和细胞色素C氧化酶(COX)染色以及超微结构观察,结果显示,(1)HE染色:肌束结构正常,肌间质未见增生,肌纤维轻度不均匀,可见散在分布的多角形或条形萎缩肌纤维(图2a);可见散在分布的“裂隙”样改变和周围蓝染的肌纤维,未见肌纤维坏死、吞噬或再生,内核纤维比例轻度增加,未见炎性细胞浸润、肌束间血管异常。(2)MGT染色:可见大量散在分布的典型破碎红纤维(图2b),未见镶边空泡、肌内神经束。(3)NADH⁃TR染色:Ⅰ型和Ⅱ型肌纤维呈镶嵌分布,未见同型肌纤维群组化,未见选择性单型肌纤维萎缩;肌纤维内网格结构大致正常,可见散在分布的少量边缘过度深染的肌纤维。(4)PAS染色、ORO染色、SDH染色和COX染色:均未见明显异常。(5)超微结构观察:透射电子显微镜观察显示,大部分肌膜连续,可见排列整齐的Z线,但部分肌纤维内可见“串珠”样脂肪滴沉积,肌原纤维溶解,Z线消失;部分线粒体嵴呈管状或同心圆状(图3a);偶见肌膜下堆积的线粒体和溶酶体(图3b),部分肌纤维可见巨大线粒体;偶见肌纤维内肌原纤维溶解,可见少量糖原占位效应;间质毛细血管基膜轻度增厚。
基因检测 采集患者外周血4 ml,采用QIAamp DNA Blood Mini/Max Kit(德国 Qiagen公司)提取基因组DNA,Primer 3.0软件(加拿大Primer公司)设计扩增线粒体tRNAlys基因引物:上游引物序列为 5'⁃CATGCCCATCGTCCTAGAAT⁃3',下游引物序列为 5'⁃TGTTGGGTGGTGATTAGTCG⁃3',均由华大基因合成。聚合酶链反应(PCR)产物片段大小为464 bp;反应体系共50 μl,包含样品 DNA 100 ng、引物 0.40 mol/L、dNTPs 0.20 mmol/L、镁离子 1 mmol/L和Taq酶1 U;反应条件为95℃预变性7 min,95℃3 min、53 ℃ 30 s、72 ℃ 40 s,共29 个循环,72 ℃延伸7 min;PCR扩增产物送检华大基因进行Sanger测序。结果显示,外周血线粒体DNA c.8344A>G突变(图4)。
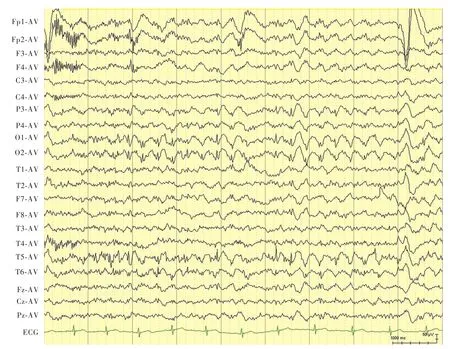
图1 VEEG显示,闪光刺激停止后仍可见后头部棘⁃慢复合波(电压50 μV,时间1000 ms)Figure 1 VEEG findings showed that spike and slow waves complex discharge in occiput could be seen after intermittent photic stimulation(voltage 50 μV,time 1000 ms).
诊断与治疗经过 根据患者临床表现,初步诊断考虑进行性肌阵挛性癫,结合骨骼肌组织活检术和基因检测结果,最终明确诊断为肌阵挛性癫伴破碎红纤维。住院期间继续予丙戊酸钠0.25 g/早和0.50 g/晚,左乙拉西坦1 g/次、2次/d以及吡拉西坦8 g/次、3次/d口服,共住院7 d,出院后遵医嘱继续上述治疗方案。电话随访,癫发作控制良好,但步态异常仍缓慢加重,目前仍可独立行走,偶有跌倒,外院复查头部MRI显示脑萎缩。
讨 论
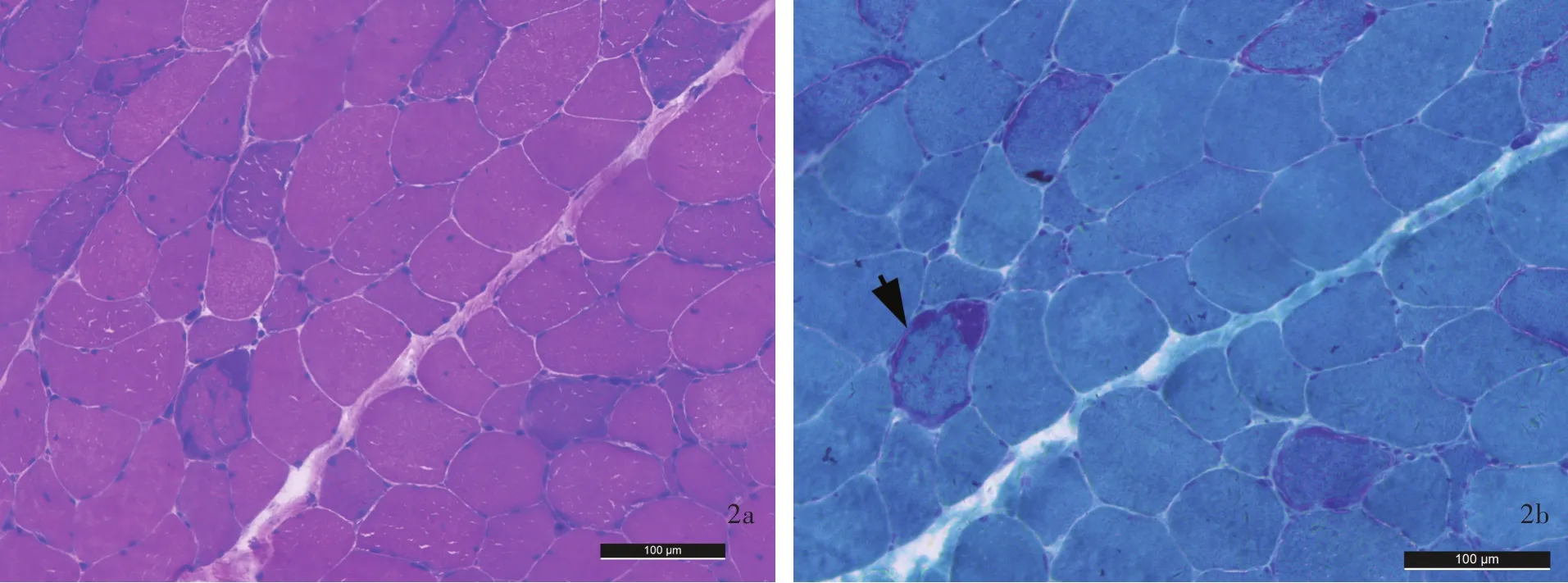
图2 光学显微镜观察所见 ×400 2a 可见散在分布的萎缩肌纤维 HE染色 2b 可见典型破碎红纤维(箭头所示) MGT染色Figure 2 Optical microscopy findings ×400 Scattered atrophic muscle fibers could be seen(Panel 2a). HE staining Typical ragged⁃red fibers were shown(arrow indicates,Panel 2b). MGT staining

图3 透射电子显微镜观察所见 枸橼酸铅和醋酸铀双重染色 3a 部分线粒体嵴呈管状(白箭头所示)或同心圆状(黑箭头所示) ×50 000 3b 肌膜下可见堆积的线粒体(白箭头所示)和溶酶体(黑箭头所示) ×10 000Figure 3 Transmission electron microscopy findings Lead citrate and uranyl acetate double staining Tubular(white arrow indicates)and concentric(black arrow indicates)mitochondrial cristae were seen(Panel 3a). ×50 000 Large amount of mitochondria(white arrow indicates)and lysosomes(black arrow indicates)accumulated under muscular membrane(Panel 3b). ×10 000
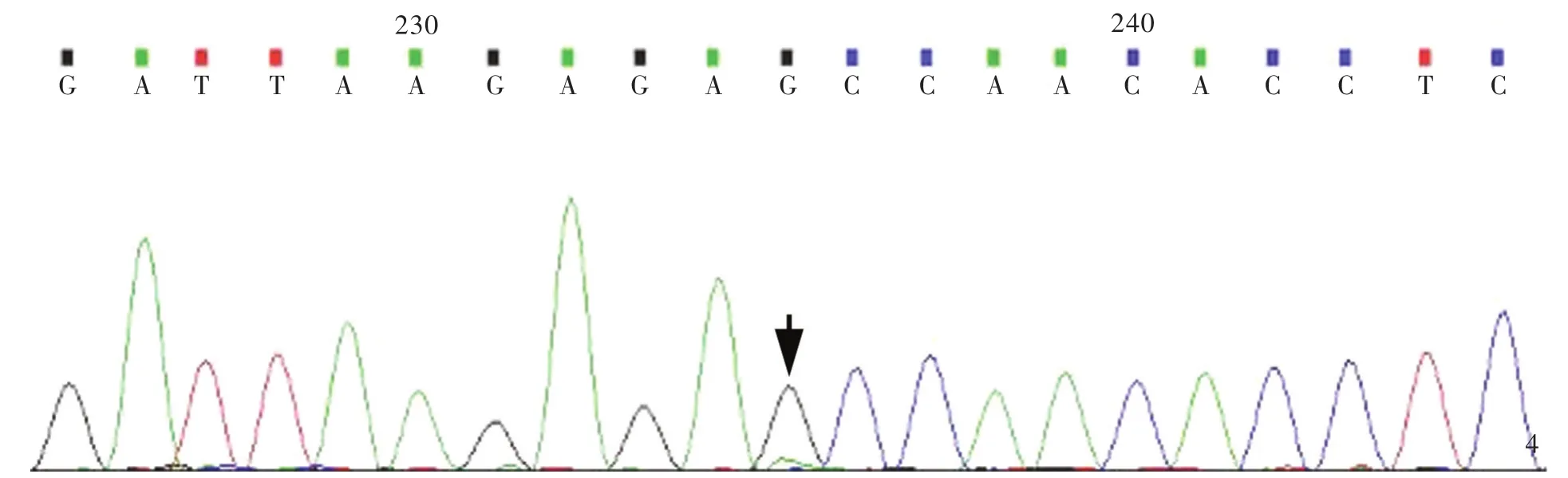
图4 Sanger测序显示,线粒体DNA c.8344A>G杂合突变(箭头所示)Figure 4 Sanger sequencing of the mitochondrial genome showed heterozygous mtDNA c.8344A>G mutation(arrow indicates).
[1]de Siqueira LF.Progressive myoclonic epilepsies:review of clinical,molecular and therapeutic aspects[J].J Neurol,2010,257:1612⁃1619.
[2]Altmann J,Büchner B,Nadaj⁃Pakleza A,Schäfer J,Jackson S,Lehmann D,Deschauer M,Kopajtich R,Lautenschläger R,Kuhn KA,Karle K,Schöls L,Schulz JB,Weis J,Prokisch H,Kornblum C,Claeys KG,Klopstock T.Expanded phenotypic spectrum of the m.8344A>G"MERRF"mutation:data from the German mitoNET registry[J].J Neurol,2016,263:961⁃972.
[3]Blakely EL,Alston CL,Lecky B,Chakrabarti B,Falkous G,Turnbull DM,Taylor RW,Gorman GS.Distal weakness with respiratory insufficiency caused by the m.8344A>G"MERRF"mutation[J].Neuromuscul Disord,2014,24:533⁃536.
[4]DiMauro S,Hirano M,Kaufmann P,Tanji K,Sano M,Shungu DC,Bonilla E,DeVivo DC.Clinical features and genetics of myoclonic epilepsy with ragged red fibers[J].Adv Neurol,2002,89:217⁃229.
[5]Cohen BH.Neuromuscular and systemic presentations in adults:diagnoses beyond MERRF and MELAS[J].Neurotherapeutics,2013,10:227⁃242.
[6]DiMauro S,Schon EA.Mitochondrial respiratory⁃chain diseases[J].N Engl J Med,2003,348:2656⁃2668.
[7]Lorenzoni PJ,Scola RH,Kay CS,Silvado CE,Werneck LC.When should MERRF (myoclonusepilepsyassociated with ragged ⁃red fibers)be the diagnosis[J]?Arq Neuropsiquiatr,2014,72:803⁃811.
[8]Chew NK,MirP,EdwardsMJ,CordivariC,MartinoD,Schneider SA,Kim HT,Quinn NP,Bhatia KP.The natural history ofUnverricht⁃Lundborg disease:a reportofeight genetically proven cases[J].Mov Disord,2008,23:107⁃113.
[9]Lalioti MD,Scott HS,Buresi C,Rossier C,Bottani A,Morris MA,Malafosse A,Antonarakis SE.Dodecamer repeat expansion in cystatin gene in progressive myoclonus epilepsy[J].Nature,1997,24:847⁃851.
[10]Boissé Lomax L,Bayly MA,Hjalgrim H,Møller RS,Vlaar AM,Aaberg KM,Marquardt I,Gandolfo LC, Willemsen M,Kamsteeg EJ,O'Sullivan JD,Korenke GC,Bloem BR,de Coo IF,Verhagen JM,Said I,PrescottT,Stray⁃Pedersen A,Rasmussen M,Vears DF,Lehesjoki AE,Corbett MA,Bahlo M,Gecz J,Dibbens LM,Berkovic SF.'North Sea'progressive myoclonus epilepsy:phenotype of subjects with GOSR2 mutation[J].Brain,2013,136:1146⁃1154.
[11]Turnbull J,Girard JM,Lohi H,Chan EM,Wang P,Tiberia E,Omer S,Ahmed M,Bennett C,Chakrabarty A,Tyagi A,Liu Y,Pencea N,Zhao X,Scherer SW,Ackerley CA,Minassian BA.Early⁃onset Lafora body disease[J].Brain,2012,135:2684 ⁃2698.
[12]Kecmanovic M,Keckarevic⁃Markovic M,Keckarevic D,Stevanovic G,Jovic N,Romac S.Genetics of Lafora progressive myoclonic epilepsy:current perspectives[J].Appl Clin Genet,2016,9:49⁃53.
[13]Minassian BA,Ianzano L,Meloche M,Andermann E,Rouleau GA,Delgado⁃Escueta AV,Scherer SW.Mutation spectrum and predicted function of laforin in Lafora's progressive myoclonus epilepsy[J].Neurology,2000,55:341⁃346.
[14]Mole SE, Cotman SL.Genetics of the neuronal ceroid lipofuscinoses (Batten disease)[J].Biochim Biophys Acta,2015,1852:2237⁃2241.
[15]Striano P,Specchio N,Biancheri R,Cannelli N,Simonati A,Cassandrini D,Rossi A,Bruno C,Fusco L,Gaggero R,Vigevano F,Bertini E,Zara F,Santorelli FM,Striano S.Clinical and electrophysiological features of epilepsy in Italian patients with CLN8 mutations[J].Epilepsy Behav,2007,10:187⁃191.
[16]Maruyama S,Saito Y,Nakagawa E,Saito T,Komaki H,Sugai K,Sasaki M,Kumada S,Saito Y,Tanaka H,Minami N,Goto Y.Importance ofCAG repeatlength in childhood⁃onset dentatorubral⁃pallidol⁃uysian atrophy[J].J Neurol,2012,259:2329⁃2334.
[17]De la Mata M,Garrido ⁃Maraver J,Cotán D,Cordero MD,Oropesa⁃Ávila M,Izquierdo LG,De Miguel M,Lorite JB,Infante ER,Ybot P,Jackson S,Sánchez⁃Alcázar JA.Recovery of MERRF fibroblasts and cybrids pathophysiology by coenzyme Q1[0J].Neurotherapeutics,2012,9:446⁃463.
[18]Chang JC,Liu KH,Chuang CS,Su HL,Wei YH,Kuo SJ,Liu CS.Treatment of human cells derived from MERRF syndrome by peptide ⁃mediated mitochondrial delivery[J].Cytotherapy,2013,15:1580⁃1596.
[19]Chuang YC,Liou CW,Chen SD,Wang PW,Chuang JH,Tiao MM,Hsu TY,Lin HY,Lin TK.Mitochondrial transfer from wharton'sjelly mesenchymalstem cellto MERRF cybrid reduces oxidative stress and improves mitochondrial bioenergetics[J].Oxid Med Cell Longev,2017:ID5691215.
[20]Finsterer J,Zarrouk⁃Mahjoub S.Management of epilepsy in MERRF syndrome[J].Seizure,2017,50:166⁃170.
[21]KoskiniemiM,VanVleymenB,HakamiesL,LamusuoS,Taalas J.Piracetam relieves symptoms in progressive myoclonus epilepsy:a multicentre,randomised,double blind,crossover study comparing the efficacy and safety of three dosages of oralpiracetam with placebo[J].J Neurol Neurosurg Psychiatry,1998,64:344⁃348.
[22]Fedi M,Reutens D,Dubeau F,Andermann E,D'Agostino D,Andermann F.Long⁃term efficacy and safety of piracetam in the treatment of progressive myoclonus epilepsy[J].Arch Neurol,2001,58:781⁃786.
[23]Ikeda A,Shibasaki H,Tashiro K,Mizuno Y,Kimura J;The Myoclonus/Piracetam Study Group.Clinical trial of piracetam in patients with myoclonus:nationwide multiinstitution study in Japan[J].Mov Disord,1996,11:691⁃700.
猜你喜欢
中国临床医学影像杂志(2022年6期)2022-07-26
中国临床医学影像杂志(2022年5期)2022-07-26
中国典型病例大全(2022年11期)2022-05-13
昆明医科大学学报(2021年10期)2021-12-02
国际放射医学核医学杂志(2021年10期)2021-02-28
科技资讯(2020年32期)2020-12-28
中华养生保健(2020年1期)2020-11-16
中国现代神经疾病杂志(2020年9期)2020-01-09
中国心血管杂志(2020年4期)2020-01-09
食品安全导刊(2018年36期)2018-05-25
