免疫球蛋白G4鉴别诊断自身免疫性胰腺炎与胰腺癌价值的荟萃分析
2016-05-19 08:15:59蒋晓涵胡乃中陈丽红
中华胰腺病杂志 2016年2期
蒋晓涵 胡乃中 陈丽红
230022 合肥,安徽医科大学第一附属医院消化内科
·论著·
免疫球蛋白G4鉴别诊断自身免疫性胰腺炎与胰腺癌价值的荟萃分析
蒋晓涵胡乃中陈丽红
230022合肥,安徽医科大学第一附属医院消化内科
【摘要】目的系统评价血清免疫球蛋白G4(IgG4)鉴别诊断自身免疫性胰腺炎(AIP)与胰腺癌的价值。方法计算机检索2015年4月1日前在Medline、EMBASE、Science Direct、Springer link、CBM、万方、维普以及中国知网数据库公开发表的有关血清IgG4鉴别诊断AIP与胰腺癌价值的英文文献,按照严格的纳入、排除标准筛选文献并提取数据,采用QUADAS量表进行文献质量评估,Stata12.0软件评估文献发表偏倚,用Meta-Disc 1.4统计软件进行异质性分析和综合定量合成,计算汇总的灵敏度、特异度、阳性似然比、阴性似然比,并绘制汇总受试者工作特征(SROC)曲线评估诊断效能。结果共纳入13篇英文文献1 403例患者,其中AIP患者448例,胰腺癌患者955例。IgG4鉴别诊断AIP及胰腺癌的汇总灵敏度为74%(95%CI70%~78%),汇总特异度为93%(95%CI91%~95%),阳性似然比为10.74(95%CI7.16~16.11),阴性似然比为0.25(95%CI0.17~0.35),SROC曲线下面积为0.9340。结论血清IgG4鉴别诊断AIP与胰腺癌的诊断效能较高,误诊率低,可以作为早期诊断AIP的辅助指标之一。
【关键词】胰腺炎;自身免疫疾病;免疫球蛋白G4;诊断,鉴别;Meta分析
自身免疫性胰腺炎(autoimmune pancreatitis,AIP)是慢性胰腺炎的一种特殊类型,临床表现与胰腺癌相似且少见[1-2], 约2.6%的AIP患者在出现胰腺肿大、胰胆管扩张等表现时被误诊为胰腺癌而行不必要的手术治疗[3],影响预后。有研究表明,AIP是胰胆癌的危险因素之一[4],故早期诊断AIP是治疗及改善预后的关键。目前世界范围内AIP的诊断标准主要有4个[5-9],但它们均复杂而不适用于临床应用,因此需要寻找方法简单且诊断价值较高的标志物。血清IgG4作为单独诊断AIP的指标具有较高的敏感度和特异度[10-11],但现有研究多为单中心、小样本,结果存在较大差异。本研究采用循征医学方法对血清IgG4诊断AIP的价值进行荟萃分析。
资料与方法
一、文献检索
计算机检索Medline、EMBASE、Science Direct、Springer link、CBM、万方、维普以及中国知网等数据库,收集自建库至2015年4月1日间公开发表的所有以患者为对象,以血清IgG4鉴别诊断AIP与胰腺癌价值为目的的英文文献。按照Cochrane协作网手工手册要求制定检索策略,检索词为“immunoglobulin G4”、“IgG4”、“autoimmune pancreatitis”、“AIP”、“pancreatitis”、“pancreatic cancer”,并追查已纳入文献或综述文献的参考文献以尽可能全面收集资料。
二、纳入及排除标准
纳入标准:(1)AIP的诊断应为下列公认标准之一,即日本胰腺协会(JPS)2006年修改版标准[5]、美国2006年的HISORt标准[6]、韩国Kim标准[7-8]、2008年亚洲标准[9]及误行手术后的病理结果;(2)AIP和胰腺癌诊断明确,各组样本数不少于10个;(3)研究的试剂来源、试验方法、IgG4检测方法明确,检测标本为血清;(4)研究中应给出或可计算出四格表相关数据的值,包括真阳性(true positive, TP)、假阳性(false positive, FP)、假阴性(false negative, FN)、真阴性(true negative, TN)。
排除标准:(1)非诊断性试验研究;(2)同作者重复文献中发表较早、样本量较小或文章质量较低的文献;(3)试验设计缺乏严格对照的文献,评述类文献、文摘、讲座等非原始研究,动物实验研究及学位论文、会议论文等;(4)资料不全或无法从文献中获得完整数据的研究。
三、文献筛选及资料提取
由两位研究者遵循盲法原则独立进行文献筛选和资料提取。筛选和提取过程中有分歧的文献通过讨论或由第三个研究者决定。提取信息包括:作者、国家、发表时间、样本量及诊断试验的各项参数信息(敏感度、特异度、TP、FP、FN、TN、Cut off值等),对文章中不详细或者不确定的数据结果联系作者或者检索相关文献予以补充。
四、文献质量评估
由两位研究者独立进行文献质量评估,有异议时通过协商解决。根据QUADAS质量标准[12]的14个条目,对每条标准划分为“是”、“否”、“不明确”3个结果。“是”表示入选文献符合该项条目,计2分;“否”表示不满足,计0分;无法提取足够的信息判定为“不明确”,计1分。总分0~15分表示文献质量较低,16~28分表示文献质量较高。
四、统计学处理
采用Meta-Disc1.4软件及Stata12.0软件进行统计学分析。由于纳入研究Cut off值不同可导致诊断试验的敏感性、特异性、诊断优势比(diagnostic odds ratio,DOR)变化,继而产生阈值效应,通过观察汇总受试者工作特征(summary receiver operating characteristic,SROC)曲线是否有“肩臂状”分布及Spearman相关系数分析判断有无阈值效应导致的异质性。非阈值效应导致的异质性采用CochranQ检验,用I2值表示异质性大小,I2≤50%表明异质性较小,选择固定效应模型进行合并计算,I2>50%表明高度异质性,选择随机效应模型合并效应量。显著性水平设定为P=0.05。应用Stata12.0软件,通过观察Deek′s图识别纳入文献是否存在发表偏倚。
荟萃分析计算汇总的敏感度、合并特异度、阳性似然比、阴性似然比及SROC曲线下面积(area under curve, AUC),并应用约登指数(Youden Index)=Sen+Spe-1评估试验的准确精度。所有的结果用95%可信区间(95%CI)表示。
结果
一、文献检索结果及质量评价
经过计算机及手工检索共获取相关文献864篇,筛选后最终纳入13篇文献[10,11,13-23],1 403例患者,其中AIP患者448例,胰腺癌患者955例(表1)。文献筛选的PRISMA流程图见图1。
按照QUADAS量表,纳入文献的质量评分为14~26分,平均21.8分,其中16~28分的文献9篇,14~15分的文献4篇,文献的整体质量较高。

表1 13篇文献IgG4诊断AIP及胰腺癌阳性率的比较

图1 PRISMA文献筛选流程
二、异质性检验
Spearman相关系数为0.033,P=0.915,不具有统计学意义,SROC曲线也不存在“肩臂状”分布,因此无阈值效应。对13篇文献的四格表数据(TP、FP、FN、TN)进行荟萃分析, IgG4鉴别诊断AIP及胰腺癌的合并敏感度、特异度、诊断优势比的I2依次为76.2%、65.4%、51.3%,均存在较高程度的异质性,故合并效应量时采用随机效应模型。
三、发表偏倚检验
13篇文献的IgG4鉴别诊断AIP与胰腺癌的差异无统计学意义(t=0.50,P=0.625), Deek′s漏斗图为对称(图2),故不存在发表偏倚。

图2 IgG4鉴别诊断AIP与胰腺癌的Deek′s图
四、合并效应量分析
IgG4鉴别诊断AIP与胰腺癌的灵敏度、特异度、阳性似然比、阴性似然比分别为74%(70%~78%,图3)、93%(91%~95%,图4)、10.74(7.16~16.11)、0.25(0.17~0.35),约登指数为0.67,SROC曲线下面积为0.9340(图5)。IgG4鉴别诊断AIP与胰腺癌时的诊断效能高,特异度高。
讨论
AIP是慢性胰腺炎的特殊类型,约占2%~6%[24],1995年由Yoshida等[25]提出后,报道的病例逐渐增多。由于其腹痛、黄疸、胰腺肿大等临床表现[26-27]不具有特异性,因此易误诊为胰腺癌而治疗过度,给患者带来生理、精神及经济上的伤害。且AIP作为胰腺癌危险因素之一[7],不能早期诊断和治疗会增加患癌风险,影响预后。因此,早期诊断AIP,正确辨别AIP与胰腺癌对提高临床胰腺疾病患者的预后至关重要。研究表明, AIP患者血清IgG4水平升高[28-29], IgG4阳性率显著高于胰腺癌患者,故随着AIP研究的不断进展,近年来众多学者提出IgG4可作为AIP的诊断指标之一,但各研究结果差异较大,其诊断价值存在争议。因此,本文对血清IgG4鉴别诊断AIP与胰腺癌的价值进行荟萃分析。

图3 IgG4诊断AIP的合并灵敏度
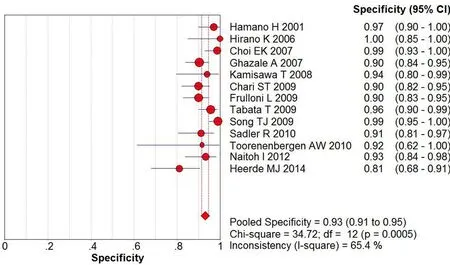
图4 IgG4诊断AIP的合并特异度

图5 IgG4诊断AIP与胰腺癌鉴别时的SROC曲线
目前认为对于存在明显异质性的试验,较之加权汇总的敏感度和特异性,SROC和AUC是更为合理的荟萃分析方法[30],具有更加稳健的效能。对某一存在较明显异质性的诊断试验,AUC>0.9时准确性最好。本荟萃分析结果显示,IgG4诊断AIP的阳性率为74%,鉴别诊断AIP及胰腺癌的特异度为93%,仅7%的患者误诊为胰腺癌,且AUC=0.9340,表明IgG4具有较高的准确性,有助于AIP患者的早期诊断及治疗,降低误诊率,避免过度治疗及患癌风险,显著改善预后,值得临床推广。
本荟萃分析的异质性检验已提示不存在阈值效应,因此,非阈值效应产生的异质性应结合临床分析。导致异质性的各种因素有:(1)纳入研究中AIP的诊断标准不同,且存在差异;(2)研究纳入对象的地理区域不同,人口统计学资料存在差异;(3)文献中未指出血清样本的采集时间,也未明确指出采集时间与检测时间的间隔长短;(4)纳入研究的IgG4检测方法不同和试剂盒的生产制造商的不同(包括cut off值选择的不同)。这些因素都可能导致本荟萃分析的异质性,影响系统评价结果。
本荟萃分析也存在一些不足之处。主要表现在:(1)检索文献的语种仅限于英文,会造成漏检其他语种的相关研究;(2)纳入研究的质量不同,难免会影响结果的可靠性;(3)检测IgG4对AIP的诊断效能受现有研究试验组分型不细致限制,仅对IgG4阳性的AIP患者进行讨论,会对结果造成偏倚。
由于对IgG4诊断AIP的研究仍较少,因此未来仍需要更多前瞻性的高质量诊断试验研究来验证。
参考文献
[1]Bednar F, Simeone DM. Pancreatic cancer stem cell biology and its therapeutic implications[J]. J Gastroenterol, 2011, 46(12):1345-1352.DOI: 10.1007/S00535-011-0494-7.
[2]Nishimori I, Tamakoshi A, Otsuki M, et al. Prevalence of autnimmune pancreatitis in Japan from a nationwide survey in 2002[J].J Gastroenteml, 2007,42(18):6-8.DOI:10.1007/S00535-007-2043-y.
[3]van Heerde MJ, Biermann K, Zondervan PE, et al. Prevalence of autoimmune pancreatitis and other benign disorders in pancreatoduodenectomy for presumed malignancy of the pancreatic head[J]. Dig Dis Sci, 2012,57(9):2458-2465.DOI:10.1007/S10620-012-2191-7.
[4]Kamisawa T, Tsuruta K, Okamoto A, et al. Frequent and significant K-ras mutation in the pancreas, the bile duct, and the gallbladder in autoimmune pancreatitis[J]. Pancreas, 2009, 38(8):890-895.DOI:10.1097/MPA.0b013e3181b65aic.
[5]Okazaki K, Kawa S, Kamisawa T, et al.Clinical diagnostic criteria of autoimmune pancreatitis:revised proposal[J].J Gastroenterol, 2006,41(7):626-631.DOI:10.1007/S00535-006-1868-0.
[6]Kim KP, Kim MH,Kim JC, et al. Diagnostic criteria for autoimmune chronic pancreatitis revisited[J].World J Gastroenterol,2006,12(16):2487-2496.
[7]Kim MH, Lee TY. Diagnostic criteria for autoimmune pancreatitis(AIP):a proposm of revised Kim criteria[J].J Gastroenterol Hepatol,2007,22(2):104.
[8]Chari ST, Smyrk TC, Levy MJ, et al.Diagnosis of autoimmune pancreatitis:the Mayo Clinic experience[J].Clin Gastroenterol Hepatol,2006,4(8):1010-1016.
[9]Otsuki M, Chung JB, Okazaki K, et al. Asian diagnostic criteria for autoimmune pancreatitis:consensus of the Japan-Korea symposium on autoimmune pancreatitis[J].J Gastroenterol,2008,43(6):403-408.DOI:10.1007/S00535-008-2205-6.
[10]Hirano K, Kawabe T, Yamamoto N, et al. Serum IgG4 concentrations in pancreatic and biliary diseases[J]. Clin Chim Acta, 2006, 367(1-2): 181-184.DOI:10.1016/j.cca.2005.11.031.
[11]Choi EK, Kim MH, Lee TY, et al. The sensitivity and specificity of serum immunoglobulin G and immunoglobulin G4 levels in the diagnosis of autoimmune chronic pancreatitis: Korean experience[J]. Pancreas, 2007, 35(2): 156-161.DOI:10.1097/MPA.0b013e318053eacc.
[12]Whiting P, Rutjes AW, Reitsma JB, et al.The development of QUADAS:a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews[J].BMC Med Res Methodol, 2003,3:25.
[13]Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis[J]. N Engl J Med, 2001, 344(10): 732-738.
[14]Ghazale A, Chari ST, Smyrk TC, et al. Value of serum IgG4 in the diagnosis of autoimmune pancreatitis and in distinguishing it from pancreatic cancer[J].Am J Gastroenterol, 2007, 102(8): 1646-1653.
[15]Kamisawa T, Imai M,YuiChen P, et al, Strategy for differentiating autoimmune pancreatitis from pancreatic cancer[J]. Pancreas, 2008,37(3):e62-e67.DOI:10.1097/MPA.0b013e318175e3ao.
[16]Chari T, Takahashi N, Levy MJ,et al. A diagnostic strategy to distinguish autoimmune pancreatitis from pancreatic cancer[J]. Clin Gastroenterol Heratol, 2009, 7(10):1097-1103.DOI:10.1016/j.cgh.2009.04.020.
[17]Frulloni L, Lunardi C, Simone R, et al. Identification of a novel antibody associated with autoimmune pancreatitis[J]. N Engl J Med, 2009,361(22):2135-2142.DOI:10.1056/NEJMOa0903068.
[18]Tabata T, Kamisawa T, Takuma K, et al. Serum IgG4 concentrations and IgG4-related sclerosing disease[J]. Clin Chim Acta, 2009, 408(1-2): 25-28.DOI:10.1016/j.cca.2009.06.036.
[19]Song TJ, Kim MH, Moon SH, et al. The combined measurement of total serum IgG and IgG4 may increase diagnostic sensitivity for autoimmune pancreatitis without sacrifi cing specifi city, compared with IgG4 alone[J]. Am J Gastroenterol, 2010, 105(7):1655-1660.DOI:10.1038/ajg.2009.689.
[20]Sadler R, Chapman RW, Simpson D, et al. The diagnostic significance of serum IgG4 levels in patients with autoimmune pancreatitis: a UK study[J]. Eur J Gastroenterol Hepatol, 2011,23(2):139-145.
[21]Toorenenbergen AW, Heerde MJ, Buuren HR. Potential value of serum total IgE for differentiation between autoimmune pancreatitis and pancreatic cancer[J]. Scandinavian Journal of Immunology, 2010,72(5): 444-448.DOI:10.1111/j.1365-3083.2010.02453.X.
[22]Naitoh I, Nakazawa T, Hayashi K, et al. Clinical differences between mass forming autoimmune pancreatitis and pancreatic cancer[J]. Scand J Gastroenterol, 2012, 47(5): 607-613.DOI:10.3109/00365521.2012.667147.
[23]van Heerde MJ, Buijs J, Hansen BE, et al. Serum level of Ca19-9 increases ability of IgG4 test to distinguish patients with autoimmune pancreatitis from those with pancreatic carcinoma[J]. Dig Dis Sci, 2014, 59(6):1322-1329.DOI:10.1007/S10620-013-3004-3.
[24]Sah RP, Pannala R, Chari ST, et al. Prevalence, diagnosis, and profile of autoimmune pancreatitis presenting with features of acute or chronic pancreatitis[J]. Clin Gastroenterol Hepatol, 2010, 8(1): 91-96.DOI:10.1016/j.cgh.2009.09.024.
[25]Yoshida K, Toki F, Takeuchi T, et al. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis[J].Dig Dis Sci, 1995, 40(7): 1561-1568.
[26]Proctor RD, Rofe CJ, Bryant TJ, et al.Autoimmune pancreatitis: anillustrated guide to diagnosis[J].Clin Radial, 2013, 68(4):422-432.DOI:10.1016/j.crad.2012.08.016.
[27]Kamisawa T, Kim MH, Liao WC, et al.Clinical characteristics of 327 Asian patients with autoimmune pancreatitis based on Asian diagnostic criteria[J].Pancreas, 2011, 40(2):200-205.
[28]Chari ST, Kloeppel G, Zhang L, et al. Histopathologic and clinical subtypes of autoimmune pancreatitis:the honolulu consensus document[J]. Pancreatology, 2010, 10(6): 664-672.DOI:10.1159/000318809.
[29]Pezzilli R. New insights into the pathology and treatment of autoimmune pancreatitis[J]. JOP, 2005, 6(2): 197-199.
[30]Walter SD. Properties of the summary receiveroperating characteristic(SROC) curve for diagnostic test data[J]. Stat Med,2002,21(9):1237-1256.DOI:10.1002/sim.1099.
(本文编辑:吕芳萍)
Immunoglobulin G4 in differentiating autoimmune pancreatitis from pancreatic cancer: a systemic review and meta-analysis
JiangXiaohan,HuNaizhong,ChenLihong.DepartmentofGastroenterology,theFirstAffiliatedHospitalofAnhuiMedicalUniversity,Hefei230022,China
【Abstract】ObjectiveTo evaluate the role of serum immunoglobulin G4 (IgG4) in differentiating autoimmune pancreatitis (AIP) from pancreatic cancer(PC). MethodsThe database, including Medline, EMBASE, Science Direct, Springer link, CBM, Wanfang ,VIP and Cnki were searched by computer and the publication date was before April 1, 2015. The studies on evaluating the accuracy of IgG4 in differentiating AIP from PC were screened and selected according to strict determined inclusion and exclusion criteria. Quality assessment was made by QUADAS scale. The publication bias were assessed by Stata12.0 software . The heterogeneity of included articles, calculate the pooled sensitivity, specificity, positive likelihood, negative likelihood were anylyzed by Meta-Disc1.4 software, respectively, and draw the summary ROC (SROC) curve. ResultsA total of 13 English articles were included and 1 403 patients were involved. The pooled sensitivity was 74% (95% CI 70%~78%), the pooled specificity was 93% (95% CI 91%~95%), the positive likelihood ratio was 10.74 (95% CI 7.16~16.11), the negative likelihood ratio was 0.25(95% CI 0.17~0.35) and the area under SROC curve was 0.9340. ConclusionsIgG4 has high diagnostic efficacy but low misdiagnosis rate in differentiating AIP from PC, which can be used as one of early diagnostic markers for AIP.
【Key words】Pancreatitis;Autoimmune diseases;Immunoglobulin G4;Diagnosis differential;Meta-analysis
(收稿日期:2015-07-30)
Corresponding author:Hu Naizhong, Email: hnz1956@msn.com
通信作者:胡乃中,Email: hnz1956@msn.com
DOI:10.3760/cma.j.issn.1674-1935.2016.02.010
猜你喜欢
新教育时代·教师版(2016年30期)2016-12-05 12:54:21
中外医学研究(2016年26期)2016-11-30 02:38:27
风湿病与关节炎(2016年10期)2016-11-23 07:06:16
中国中药杂志(2016年20期)2016-11-19 13:25:02
中国中药杂志(2016年20期)2016-11-19 12:33:47
今日健康(2016年12期)2016-11-17 19:20:27
今日健康(2016年12期)2016-11-17 14:47:33
中国现代医生(2016年23期)2016-11-15 03:22:39
中国科技博览(2016年19期)2016-10-19 13:05:18
中国科技博览(2016年18期)2016-10-19 10:10:52