
Surgery at early versus late for intermittent exotropia: a Meta-analysis and systematic review
2021-04-17 02:43YiDongLiNanYuYanLiu
Yi Dong, Li Nan, Yu-Yan Liu
Tianjin Eye Hospital, Tianjin Key Lab of Ophthalmology and Visual Science, Tianjin Eye Institute, Clinical College of Ophthalmology Tianjin Medical University, Tianjin 300020,China
Abstract
● KEYWORDS: Meta-analysis; intermittent exotropia;surgery; timing
INTRODUCTION
I ntermittent exotropia (IXT) is a common form of childhood exotropia, which accounts for ~50%-90% of all exotropia cases and affects ~1% of the general population[1-3]. It is characterized by the intermittent outward deviation of either eye that, if untreated, can gradually become constant in about one-third of the cases[4]. The age of onset for IXT coincides with the age of the visual maturation in children, which is between 3 and 6y[5]. This condition may lead to poor binocular functions, such as poor stereopsis, vision suppression and/or amblyopia[6].
Surgery is the mainstay approach for restoring binocular single vision and enhancing cosmetic appearance in patients with IXT[7]. However, studies focused on the relationship between age at surgery and the surgical response have shown contradictory results. In general, three distinct recommendations have been reported about the proper timing for a surgical procedure. Some researchers support delayed surgery since it may enable an accurate measurement of the deviation as well as adequate monitoring of its progression[8-11].Other studies have recommended early surgical procedures,before the occurrence of intractable sensory changes, since a greater chance of maintaining high-grade stereopsis can be achieved[12-15]. However, other reports have concluded that age at surgery might be irrelevant to the pathological outcome[16-18].Therefore, we have presently performed a thorough and comprehensively database search and further Meta-analysis to determine whether IXT surgery should be done early or late during disease progression. Based on this work, we aimed to obtain more conclusive results and provide references for future trials.

Table 1 Main characteristics of studies included in this Meta-analysis

Table 2 The outcomes of each study
MATERIALS AND METHODS
Search Strategy The PRISMA guidelines for Meta-analysis were followed on this study[19]. We conducted a systematic literature search in the PubMed, Embase, Web of Science,Cochrane and China National Knowledge Infrastructure(accessed December 16, 2019) with the following free words and MeSH terms: “intermittent exotropia”, “X(T)”, “surgery”,“age factors”, “early”, “late”. We also supplemented our search by screening the reference lists of all retrieved studies.Potential articles were first reviewed according to their title and abstract only, followed by the full text and, finally, by analyzing eligible studies in details. The language was not limited to English. Bibliographies of all included articles were reviewed to identify additional citations. The search was performed by two authors independently.
Inclusion and Exclusion Criteria Studies with the following criteria were reviewed: 1) patients grouped by the age at surgery; 2) availability of precise date for early or late surgery; 3) the criteria of the success was explicitly defined; 4)patients with specific inclusion criteria and excluded paralytic or restrictive strabismus, congenital systemic anomalies,neurological disorders, history of previous strabismus surgery.Studies were excluded if other types of strabismus were detected, in which the surgical outcomes for IXT could not be extracted separately.
Data Extraction and Clinical Outcome Data were carefully and independently extracted by two independent investigators(Dong Y and Nan L). Disagreements regarding the inclusion of studies were resolved after discussion with other authors(Liu YY). As shown in Tables 1 and 2, the following information was extracted from all included articles: first author, publication year, country, type of surgery, follow-up period, definition of success, the boundary of age at surgery,and detailed outcome(s) of early and late surgery. As a point of clarification for the boundary of age at surgery, doing surgery younger than boundary age is early surgery group. On the contrary, doing surgery at the boundary age or older is late surgery group. For studies with more than one control group,we combined groups to create a single pairwise comparison as recommended by the Cochrane Handbook for Systematic Reviews of Interventions[20]. The mean age of patients in these studies was not available for we didn’t have raw data.
Quality AssessmentMethodological quality was assessed using an 11-item checklist, based on a pre-established scale provided by the Agency for Healthcare Research and Quality(AHRQ)[21]. An item would be scored “0” if the answer was“NO” or “UNCLEAR”. If the answer was “YES”, then the item would be scored “1”. The article quality was assessed as it follows: low quality: 0-3; moderate quality: 4-7; and high quality: 8-11.
Statistical AnalysisAnalyses were performed using STATA version 16.0 (Stata Corp LP, College Station, TX, USA).A P-value <0.05 was considered statistically significant.Forest plots were created to summarize the composite data,generating odds ratios and corresponding 95% confidence intervals (CIs) for the outcome of the first and the last followup[22]. The heterogeneity among the studies included in the Meta-analysis was assessed and quantified using the Chisquare based Q statistic test and the I2metric. Findings were considered statistically significant if PQ≤0.10 or I2>50%. If there was statistically significant heterogeneity among the studies, a random-effect model would be used. If not, data would be pooled using a fixed-effect model. The sensitivity of the pooled results was assessed by omitting each study once at a time. In addition, publication bias was evaluated by Begg’s rank correlation and Egger’s linear regression tests. Twotailed P-values <0.05 were also considered to be statistically significant[23-24].
RESULTS
Search and Selection of StudiesLiterature searches yielded 181 potential articles and left 85 articles after removal of duplicates. After screening titles and abstracts, 12 full articles were retrieved for full-text evaluation. After application of exclusion criteria, 11 articles met criteria for final inclusion[10,12-16,25-29]. A PRISMA flow diagram showing the process of study selection is presented in Figure 1.

Figure 1 PRISMA flow diagram of studies included in the Metaanalysis.
Characteristics and Quality of TrialsAmong the 11 enrolled publications, different thresholds were used to establish the timing between early and late surgeries. Four studies set this boundary as 4y, while two studies set it as 5y and five additional studies set it as 6y. In terms of the surgical method,four studies prescribed bilateral lateral rectus recession (BLR),while seven studies prescribed both bilateral lateral rectus recession (BLR) and unilateral recession-resection (R&R).Most of the studies defined success as the achievement of motor success, which meant orthotopic or limited deviation.However, Pratt-Johnson et al[12]have adopted a more strict criteria for success, which contained six distinct principles.The follow-up duration of all the studies here analyzed were,at least, of 6mo. Details of each study are presented in Tables 1 and 2.
Meta-analysis ResultsAs there was a high heterogeneity among the studies, we performed a random effect model for the pool of the first follow-up and the final follow-up results.As shown in Figures 2 and 3, no significant difference was observed when comparing early and late surgical procedures in IXT patients (ORFirstfollow-up=0.88, 95%CI 0.53-1.44, P=0.61;ORFinalfollow-up=1.48, 95%CI 0.94-2.31, P=0.09). However,these results did not withstand the sensitivity analysis (Figure 4).After omitting the study of Chia et al[26], the pooled results of the final follow-up were more promising for early surgery(OR=1.71, 95%CI 1.17-2.49). In fact, subgroup analyses revealed that early surgery has a better outcome in the 4-year boundary subgroup and the BLR subgroup related to the final follow-up (OR4y=2.64, 95%CI 1.57-4.44, P=0.00; ORBLR=2.25,95%CI 1.36-3.74, P=0.00). According to Begg’s and Egger’s tests, no obvious evidence of publication bias was detected(Figure 5).

Figure 2 Forest plot of the outcome in the first follow-up (random effect model) A: The different boundaries of age at surgery subgroup analysis; B: The different surgery methods subgroup analysis.
DISCUSSION
In this study, we enrolled 11 retrospective cohort studies (with total 1122 patients) and further Meta-analysis to confirm whether IXT surgery should be performed at early or late stages. In terms of early postoperative eye position, our study has indicated no differences between early and late surgical procedures. Nevertheless, no conclusion was obtained from the pooled results related to long time surgery outcome. The final follow-up pooled result was also negative and, however,could not withstand sensitivity analysis. The result favored early surgical procedures after omitting one study of the enrolled study. A high heterogeneity among the studies could be noticed, so conducting subgroup analyses were necessary to find the source of this heterogeneity. As shown in Figure 3, the heterogeneity originated from the 6-year subgroup (I2=61.8%,P=0.03) as well as the BLR and R&R subgroups (I2=71.7%,P=0.00). The results from the 4-year and BLR subgroups suggested that an early surgical procedure was significantly better than a late procedure.
Some studies have indicated that early surgery might be difficult in measuring deviation, particularly in young patients that cannot cooperate well with their physicians[8-9]. However,based on our analysis, better results could not be accomplished at the first follow-up, even in the late-surgery cases. Therefore,the particular concern of difficult evaluation in early cases might not be worth consideration.
As shown in Figure 3, early surgery could mostly double the success rate when compared to late surgery in the 4-year subgroup. Many studies have concluded that early surgical intervention can restore fusion and stereo acuity in patients with IXT[30-32]. The fusion and stereo acuity has been associated with better surgical success in IXT[31]. Hence, surgery at early stages could lead to a better long-term result. However, most of the studies have only concerned motor success without including sensorial results, including good stereopsis and fusion. Pratt-Johnson et al[12]have introduced a comprehensive criterion of success, which contained both motor and sensorial achievements. According to their study, surgery for exotropia in patients below 4y of age resulted in better outcomes when compared to the result in patients above 4 years old (61% vs 28%, respectively). This result is consistent with our current observations. However, they also found that strabismic amblyopia due to persistent overcorrection only occurred in the early surgery group. In subsequent studies, it was concluded that age at surgery of patients does not affect the incidence of consecutive esotropia[13-14]. Since there are controversies for whether early surgery leads to higher risks of consecutive esotropia, more in-depth studies are further required.Furthermore, two particular studies have independently defined sensorial success. Jeon and colleagues[13]defined sensorial success when the stereoacuity was better than 60 seconds of arc during final examination. Issaho et al[15]have also taken in to consideration change in stereoacuity as a sensorial marker. In this case, it was also observed a better stereoacuity due to early surgery in patients younger than 4 years old. Still, since these patients had not been evaluated for preoperative stereoacuity, it was not clear whether the subnormal stereoacuity was related to the surgical procedure and/or the natural exotropic progression. In fact, preoperative stereoacuity in children might be variable and, therefore,risky to be correctly measured. So, it is not straightforward to conclude whether early surgery before 4 years of age would be a more effective route to achieve sensorial success.
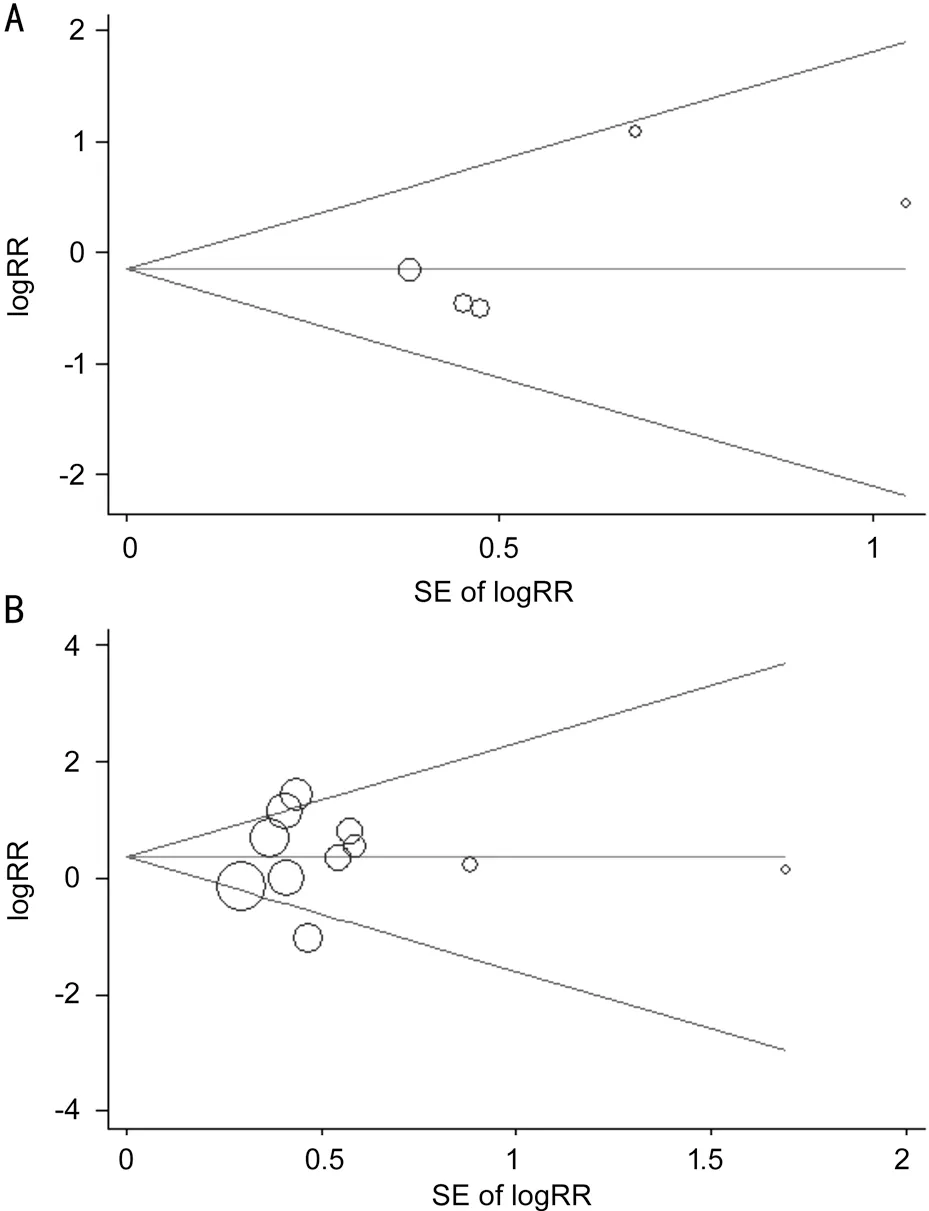
Figure 5 Funnel plot of the studies A: The first follow-up; B: The final follow-up.
Our current study has not identified any superior effect for early surgery in either 5- or 6-year subgroups. A possible reason could be related to the limited development of stereopsis and fusion after 4 years old. According to the observation 666 cases, Maruo et al[18]have also discovered that early surgery is not necessary when surgery was done over 4 years old of patients. As indicated, our study solely contained three boundary sets related to age at surgery. Therefore, we were unable to come across same conclusion like Maruo’s study but, nevertheless, early surgery appears not be necessary in patients between 4 to 6 years old. The pooled results of our study could not provide evidence for whether surgery should be done early or late when patients are older than 6y.
Our observations support early surgery in the BLR subgroup but, contrarily, results could not indicate any benefit with early surgery in the BLR and R&R subgroups. This contrasting effect might be due to the high heterogeneity of the BLR and R&R subgroups (I2=66.4%, P=0.01). Hence, we suggest that surgical procedures should be evenly maintained for further studies.
Due to the small number of cases and low prevalence of the pathology, the timing of surgery for IXT was quite variable among the studies. Here we conducted a Meta-analysis to validate the impact of age at surgery in IXT. Nonetheless,some limitations were noticeable in this study. First, the studies here evaluated were retrospective study. Second, most of the selected studies focused on motor success and overlooked any sensorial achievement. Therefore, more attention should be devoted to sensorial success in further studies. Third, most of studies excluded A-V type strabismus, dissociated vertical deviation and other accompanying strabismus types, but there were three studies exceptions[13,16,28]. The rate of other accompanying strabismus types had no difference between the early surgery group and the late surgery group in Koo et al’s[28]and Jeon et al’s[13]study. Na and Kim’s[16]study included dissociated vertical deviation and inferior oblique overaction patients, and the statistical comparison between the early surgery group and the late surgery group was not conducted.Although the sensitivity analysis indicated that it didn’t change the pooled results after omitting this study, it might be a source of heterogeneity in our Meta-analysis. Future studies should try to avoid this problem.
In conclusion, age at surgery might not affect the early postoperative alignment of IXT. Besides, early surgery was able to provide a better long-term postoperative outcome when patients were younger than 4 years old or patients chose the BLR surgical method. Broader studies, including more extensive cohorts, are required to further validate our conclusions.
ACKNOWLEDGEMENTS
Foundation:Supported by the Natural Science Foundation of Tianjin (No.18JCZDJC36400).
Conflicts of Interest: Dong Y,None;Nan L,None;Liu YY,None.
 International Journal of Ophthalmology2021年4期
International Journal of Ophthalmology2021年4期
- International Journal of Ophthalmology的其它文章
- Prevalence and risk factors of dry eye disease in young and middle-aged office employee: a Xi’an Study
- YM155 inhibits retinal pigment epithelium cell survival through EGFR/MAPK signaling pathway
- Clinical features and treatment outcomes of intraocular lymphoma: a single-center experience in China
- Trends in research related to high myopia from 2010 to 2019: a bibliometric and knowledge mapping analysis
- A simple new technique for the induction of residual posterior vitreous cortex removal and membrane peeling
- Differential degeneration of rod/cone bipolar cells during retinal degeneration in Royal College of Surgeons rats