
Prevalence and risk factors of dry eye disease in young and middle-aged office employee: a Xi’an Study
2021-04-17 02:44JingWenHuXiuPingZhuShiYinPanHuaYangXiangHuaXiao
Jing-Wen Hu, Xiu-Ping Zhu, Shi-Yin Pan, Hua Yang, Xiang-Hua Xiao
1Department of Cardiology, the First Affiliated Hospital of Xi’an Jiaotong University, Xi’an 710061, Shaanxi Province,China
2Shaanxi Institute of Ophthalmology, Xi’an City First Hospital,Xi’an 710002, Shaanxi Province, China
3Shaanxi Key Lab of Ophthalmology, Xi’an 710002, Shaanxi Province, China
4Clinical Center for Ophthalmology of Shaanxi Province,Xi’an 710002, Shaanxi Province, China
Abstract
● KEYWORDS: dry eye disease; prevalence; office employee; video display terminal; central air conditioning;age; female
INTRODUCTION
Dry eye disease (DED) is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film. DED is accompanied by ocular symptoms whose etiologies include tear film instability and hyperosmolarity,ocular surface inflammation and damage, and neurosensory abnormalities[1]. Previous DED epidemiology studies have found that the prevalence of the disease varies widely, from approximately 5% to over 50% in different parts of the world[2]. Its prevalence distribution is significantly skewed in the Chinese population, with a reported range from 21% to 50.1%[3-5]. Given its high prevalence, DED is one of the most common ocular disorders and reasons for patients seeking eye care, and the disease is becoming a growing public health problem whose consequences remain underestimated.
The global information age is resulting in a dramatic increase in the use of video display terminals (VDTs) and is changing the lifestyles of the general public, including both young and old. The use of a VDT is recognized as a high-risk factor for the onset of ocular symptoms such as eye strain and ache,dryness, irritation, and burning[6]. Prolonged VDT use is associated with a high prevalence of DED[7-8], and it also has a significant negative impact on the quality of life and work productivity[9-10]. Although the use of VDTs is increasing, the prevalence of DED associated with VDT remains unclear[11-12].Cross-sectional surveys of the prevalence of DED among VDT users have found that the prevalence ranges widely, from 9.5% to 87.5%[7-8,10,13-16]. However, only a few studies have investigated the underlying risk factors and estimated the tear function[7,16].
China is one of the fastest-growing economies globally, where VDTs are now used extensively in daily life and work. A report of the China Internet Network information Center indicated that there were 772 million Internet users in China in 2017[17].Many office employee view VDTs daily, but few studies have investigated the prevalence of and risk factors for DED using questionnaires and clinical evaluations in young and middleaged Chinese office employee.
This study aimed to estimate the prevalence of and risk factors for DED, and characterize tear function among Chinese young and middle-aged office employee.
SUBJECTS AND METHODS
Ethical ApprovalThis study was approved by Shaanxi Institute of Ophthalmology Review Board, and all subjects were treated in accordance with the Declaration of Helsinki.Informed consents were obtained from all the subjects who were willing to attend the survey before eye examination.
Study PopulationThe authors arbitrarily selected a hospital,a college of a local university, and a government department in Xi’an, and telephoned the admissions offices of each unit to explain the aim of the study and to request their participation.After acquiring permission from each unit, a printed questionnaire was sent to the admissions office of the units several days before performing eye examinations.
Dry Eye Disease QuestionnaireThe DED questionnaire used in this study comprised two parts. The first part addressed the ocular surface disease index (OSDI), which estimated the ocular surface symptoms and the severity of DED. This part of the questionnaire contained 12 questions on the frequency of DED symptoms experienced during the previous week (light sensitivity, gritty sensation, painful or sore eyes,blurred vision, and poor vision), vision-related daily activities(reading, watching TV, working on computers, and driving at night), and environmental triggers (wind, air conditioning,and low humidity). These 12 items of the OSDI questionnaire were scored on the following 5-point scale: 0, none of the time; 1, sometimes; 2, half of the time; 3, most of the time;and 4, all of the time. The OSDI was calculated using the following formula: OSDI=[(sum of scores for all questions answered)×100]/(total number of questions answered)×4[18].
The second part of the questionnaire addressed potential risk factors for DED. Information was acquired on sex, age,current smoking, VDT usage (number of hours using VDTs daily during the previous week), presence of a central air conditioning system in an office building, current wearing of cornea contact lenses, self-reported dryness of the mouth and nose, and presence of rheumatic disease.
Clinical ExaminationsThe fluorescein tear film break-up time (FTBUT) and Schirmer’s test without local anesthesia were applied to evaluate tear function. One drop of 2% sodium fluorescein was instilled into the lower conjunctival sacs of both eyes, and the subjects were then instructed to blink three times to ensure adequate mixing of the dye with the tears before holding their eyes open. The time taken for a random dark spot to first appear on the cornea was recorded using a stopwatch. Three consecutive evaluations were performed for each eye, and the mean value was recorded.
Schirmer’s test was subsequently performed without local anesthesia. A precalibrated filter strip (Jingming New Technological Development Company, Tianjin, China) was placed temporally in each outer one-third of the temporal lower conjunctival fornix, and left in place for 5min. The patient was asked to keep their eyes close during the test. When the strips had been removed 5min later, the amount of wetting (in millimeters) was recorded based on visual observations of the precalibrated strips.
Diagnosis of Dry Eye DiseaseDED was diagnosed as being present when the following two criteria were satisfied: 1)DED symptom positivity confirmed by an OSDI of >22[19-20],2) presence of tear dysfunction in either or both eyes (FTBUT≤5s[21-22]or a Schirmer’s test result of ≤5 mm/5min[21]).
Statistical AnalysesThe prevalence of DED and the results of clinical evaluations among office employee according to sex, age, and VDT usage time were evaluated using the Chisquare test or one-way ANOVA followed by the LSD test to identify differences among groups. We categorized prolonged daily VDT use as >6h, and we classified age into two groups:≤40 and ≥40y. Univariate and multivariate Logistic regression analysis was used to determine predictive factors of DED and calculate odds ratios (ORs) and 95% confidence intervals (CIs)for demographic, lifestyle, and medical factors related to DED.Univariate binary Logistic regression was carried out as a first step. Then the variables with P<0.20 identified in the univariate binary Logistic regression were considered in the multivariable Logistic regression under the condition of mutual adjustment for all associated factors. Probability values of P<0.05 were considered to indicate statistically significant differences. All of the statistical analyses were performed using SPSS software(version 23.0, SPSS, Chicago, IL, USA).
RESULTS
The characteristics of the participants in this study according to sex are presented in Table 1. They comprised 226 female(46.5%) and 260 male (53.5%) office employee aged from 20 to 59y, and their overall prevalence of DED was 40.3%(95%CI=36.0%-44.7%). Those aged 20-39y accounted for 71.2% of the study population. Many (39.6%) of the males were current smokers, compared with only 0.4% of the females. In addition, 34 (15.0%) females and 5 (1.9%) males wore cornea contact lenses.

Table 1 Characteristics of the participants: DED among the office employee n (%)

Table 2 Detailed findings of ocular symptoms and signs among office employee by sex n (%)
The detailed findings for ocular symptoms and signs among the office employee according to sex are presented in Table 2.The OSDI was higher (t=-2.884, df=484, P<0.01) and FTBUT was shorter (t=3.792, df=484, P<0.01) in females than in males.
The results for OSDI and the ocular evaluations according to age are presented in Table 3. The OSDI (F=2.716,df=3, P<0.05), VDT usage (F=12.355, df=3, P<0.01),and Schirmer’s test value (F=5.237, df=3, P<0.01) varied significantly with age. OSDI increased from 24.4±15.3 in the age group of 20-29y to 31.0±23.4 in the age group of 50-59y(P=0.009). However, the VDT usage time dropped sharply from 6.2±3.3h in the age group of 20-29y to 3.9±2.7h in the age group of 50-59y (P<0.001). Schirmer test also decreased from 13.4±10.3 mm/5min in the age group of 20-29y to 8.4±8.4 mm/5min in the age group of 50-59y (P=0.001).
The results for the DED prevalence and clinical evaluations among the office employee according to VDT usage time are listed in Table 4. The prevalence of DED increased from 33.7% for VDT usage of 0-3h to 49.5% for VDT usage of>6h (χ2=10.918, df=2, P<0.05), while OSDI increased from 20.8±17.7 to 29.6±16.1 (P<0.01). However, the subjects using VDTs for >6h were considerably younger (29.6±16.1y,P=0.000) than those using VDTs for 0-3h daily (37.6±10.9y).The results of the univariate and multivariate binary Logistic regression on the associations between demographic, lifestyle,medical factors, and DED are presented in Table 5. Predictive factors associated with DED at P<0.2 in univariate binary Logistic regression analysis were included in multivariate binary Logistic regression analysis. This model revealed that the possible risk factors for DED were being female(OR=1.592, 95%CI=1.034-2.451, P=0.035), being aged ≥40y(OR=1.593, 95%CI=1.034-2.454, P=0.035), using a VDT daily for >6h (OR=1.990, 95%CI=1.334-2.971, P=0.001), the
presence of central air conditioning (OR=1.548, 95%CI=1.053-2.276, P=0.026), and self-reported dryness of the mouth and nose (OR=1.589, 95%CI=1.071-2.357, P=0.021).

Table 3 DED prevalence and clinical evaluations among office employee by age

Table 4 DED prevalence and clinical evaluations among office employee by VDT usage time
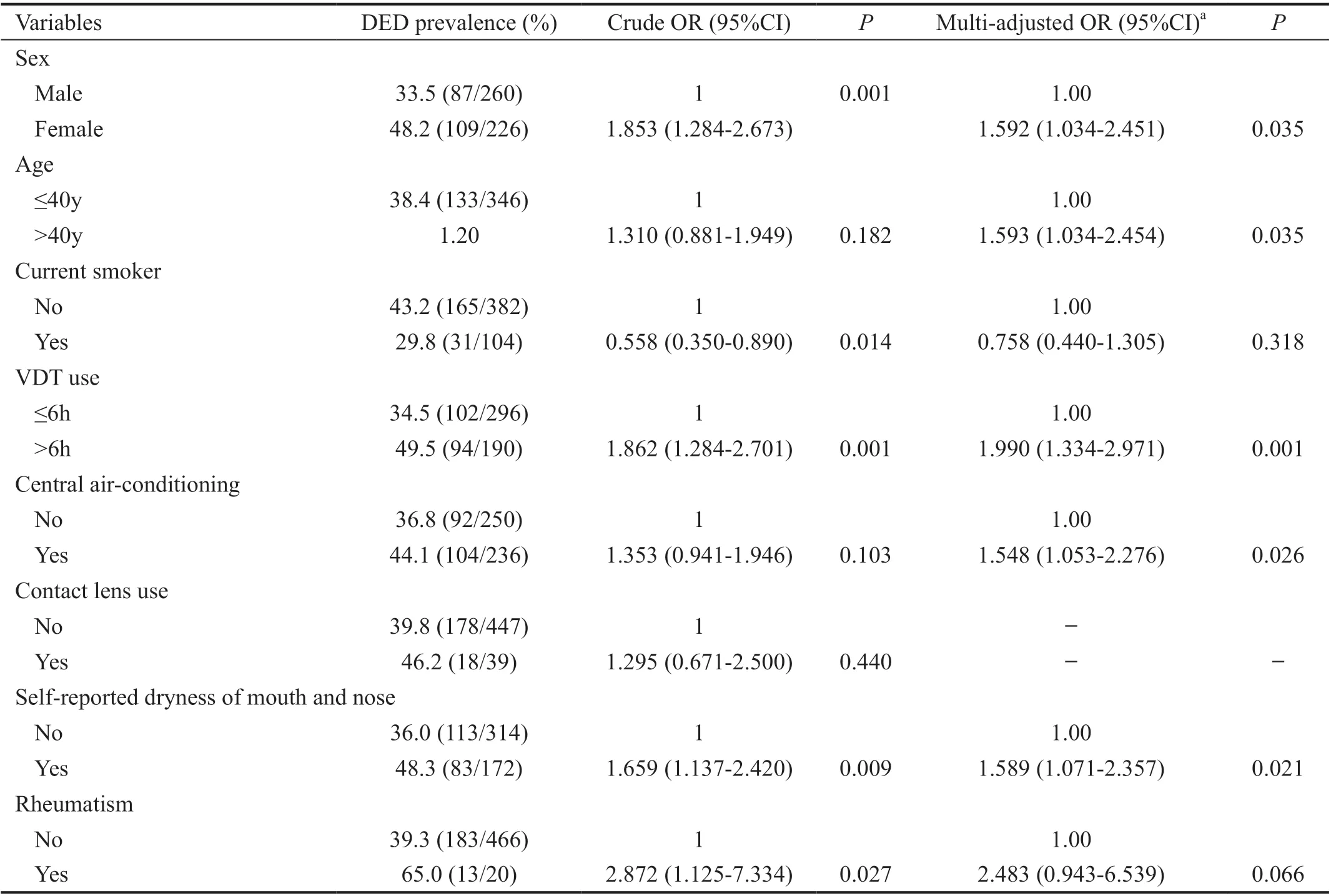
Table 5 Association between demographic, lifestyle, and medical factors and DED
DISCUSSION
To the best of our knowledge, this is the first cross-sectional study of office employee in China that has investigated the prevalence of DED and its associated risk factors.The prevalence of DED in this study was 40.3%, which is within the range of previous reports (21% to 50.1%)[3-5]. The participants were relatively young, at 34.6±9.7 years old,with those aged 20-39y accounting for 71.2% of the study population. The results showed that DED was associated with several risk factors, including being female, being older,prolonged VDT use, central air conditioning, and self-reported dryness of the mouth and nose.
This study found that the prevalence of DED was higher in females (48.2%) than in males (33.5%), which is consistent with previous reports of females being more likely to develop DED[23-24]. The female respondents in this study showed relatively severe symptom scores and worse tear film instability compared with their male counterparts. This might be attributable to androgens having a protective function on the ocular surface[25]. Another risk factor associated with females may be the usage of ocular cosmetics, which could disrupt the homeostasis of the ocular surface and tear film both directly and indirectly[26]. This is consistent with us finding that 75.7% of the female respondents showed tear-film instability,compared with 56.9% of their male counterparts.
This study also found older age to be a risk factor for DED.TFBUT showed no clear trends among the different age groups. However, the OSDI values of all respondents increased and their Schirmer tests decreased with age. These results suggest that DED is an age-related ocular disorder, especially in terms of ocular symptoms and aqueous tear secretions,which might be attributable to the aging process affecting the immune system, cellular metabolic metabolism, and inflammation of the ocular tissue[27].
Several previous studies found that the DED prevalence was higher among current smokers[28-29], but this was not replicated in the current study. The vast majority of the current smokers in this study were males, and the prevalence of DED among current smokers was lower than both among males and the entire investigated population, which is consistent with the findings of a Beijing Eye Study[7,30]. This may be due to smoke reducing the sensitivity of the nerves on the ocular surface,which in turn lessens the perceived symptoms.
This study confirmed that the daily use of VDTs for >6h was a risk factor for DED. However, a previous study in university undergraduate students in Ghana indicated that that using these devices for one hour or more was not associated with dry eye symptoms[31]. This discrepancy implies that daily prolonged usage of VDT for more than 6h increases the risk for DED while an hour or more may not. Therefore, people should spend moderate time on VDT so as to keep their ocular health.Prolonged VDT use is thought to decrease the spontaneous eye blink rate, increase the incomplete blink rate, and promote evaporation of the tear film, thus inducing DED[32-33]. Although the spontaneous eye blink rate and incomplete blinking rate were not measured in this study, the authors of an Osaka Study[9]made similar speculations based on the findings that tear film instability may be affected by blink frequency and patterns among the VDT users. The present results support the presence of an association between prolonged computer use and DED prevalence.
It was particularly interesting that the DED prevalence,OSDI, and Schirmer’s test value increased as the VDT use time increased, whereas TFBUT and age showed opposite trends. These data suggest that prolonged daily VDT use induces deteriorative DED symptoms via reducing the tear film stability, while it might not reduce lacrimal secretion function. This opinion is also supported by the finding that most of those with DED in this study had both DED symptoms and shortened TFBUT, and it is consistent with the results from the Osaka Study[9]. Another aspect of concern was that the respondents who used VDTs for more than 6h showed a high DED prevalence of 52.2%. These subjects showed the mean values of longest Schirmer’s test, shortest TFBUTs, and highest OSDI values among the different VDT-usage-time groups, despite having the lowest mean age.
This study also found that most of the subjects using VDTs had normal lacrimal secretion function, based on the results of Schirmer’s tests. Although lacrimal secretion decreased significantly with increasing age, the Schirmer’s test values of the respondents in the survey all exceeded the diagnostic threshold. Epidemiological surveys performed during the last 20y have produced a significant amount of evidence that most DED cases encountered in daily life, especially among VDT employee, manifest with a short TFBUT[22]. Regarding tear dysfunction, 56.9% of the males and 75.7% of the females had short TFBUT values, while smaller proportions of the respondents (37.3% and 31.0% of males and females,respectively) presented with low aqueous tear secretion.
Central air conditioning was also observed to be significantly related to a higher prevalence of clinically diagnosed DED in this study. This is consistent with Asiedu et al[31]who reported similar findings in their study. Low humidity are proved to increase the ocular evaporative rates under the circumstance in laboratory testing conditions simulating airplane cabin[34],which is similar with central air conditioned rooms. In addition, air conditioning with a high central ventilation unit has been reported to be associated with an increased risk of general symptoms, including eye discomfort[35]. Therefore, the dehydrated air combined with ventilation flow produced by a central air-conditioning system would increase tear evaporation and eye dryness, especially under the circumstance of office employee tending to blink less while they are looking at VDTs.The wearing of contact lenses has been reported to be associated with a higher prevalence of DED[36]. However,the present study found no contact-lens-related trend related to the DED prevalence. This was probably attributable to the respondents who wore contact lenses (28.2±5.0y) being much younger than those who did not wear contact lenses(35.2±9.8y).
Our results indicated that self-reported dryness of the mouth or nose (but not rheumatic disease) was found to be a risk factor for DED after performing mutual adjustment for all associated factors identified in the univariate analyses. Ito et al[37]also found that dry nose was associated with dryness of the eyes and mouth, and considered that dryness in one region was clearly associated with that in other regions. Sjögren’s syndrome is a chronic autoimmune rheumatic disease, in which dryness of the mouth or nose is one of the characteristic symptoms, that affects 10.3 out of 10 000 inhabitants in the USA[38]. Although 13 (65%) of the 20 participants in the present study with rheumatic disease had DED, Logistic regression after adjusting all of the identified associated factors obtained a negative result. However, this is probably due to the smallness of the sample and the low prevalence of Sjögren’s syndrome.This study was subject to some potential limitations. The main limitation was its cross-sectional design, which restricts the ability to infer causality, since only potential associations between DED and identified risk factors could be demonstrated. Hence, prospective follow-up studies involving VDT users without DED are required to identify risk factors for DED during the subsequent follow-up. Moreover, VDTrelated DED includes a myriad of other factors, and this study did not address all of the possible confounding factors. While we investigated the associations of smoking, VDT usage, air conditioning, wearing contact lenses, self-reported dryness of the mouth and nose, and rheumatic disease with DED, many other potential risks factors that could induce DED were not investigated in the study, such as sleep quality, blinking pattern, and environment pollution. Another possible limitation is the restricted age range of our study involving a working population, with most (71.2%) of the respondents being aged 20-39y, and none of them being older than 60y.
In summary, this cross-sectional study performed in Xi’an(a city in northwest China) has revealed a high prevalence of DED among young and middle-aged VDT users by applying a combination of a DED questionnaire and clinical
DED evaluations. Most of the respondents showed a short TFBUT and normal tear secretion. Being female, being older,prolonged VDT use, presence of central air conditioning, and experiencing a dry mouth and nose were confirmed as possible risk factors for DED. We anticipate that the results of our study will raise concerns about the high prevalence of the disease and its long-term consequences being underestimated. Thus,public health education and precautions are necessary against modifiable risk factors in order to prevent the occurrence and development of DED in office employee.
ACKNOWLEDGEMENTS
Authors’ contributions:Conception or design of the work:Xiao XH and Zhu XP; Data collection: Xiao XH, Pan SY and Yang H; Data analysis and interpretation: Hu JW and Xiao XH; Drafting the article: Hu JW; Critical revision of the article: Hu JW and Xiao XH.
Foundations:Supported by Science and Technology Major Projects of Shaanxi Province, China (No.2017ZDXMSF-070); Science Foundation of Shaanxi Province, China(No.2010JM4011); Xi’an Science and Technology Bureau,China (No.2019115913YX014SF047).
Conflicts of Interest: Hu JW,None;Zhu XP,None;Pan SY,None;Yang H,None;Xiao XH,None.
 International Journal of Ophthalmology2021年4期
International Journal of Ophthalmology2021年4期
- International Journal of Ophthalmology的其它文章
- Cost-effectiveness analysis of tele-retinopathy of prematurity screening in lran
- YM155 inhibits retinal pigment epithelium cell survival through EGFR/MAPK signaling pathway
- Clinical features and treatment outcomes of intraocular lymphoma: a single-center experience in China
- Trends in research related to high myopia from 2010 to 2019: a bibliometric and knowledge mapping analysis
- A simple new technique for the induction of residual posterior vitreous cortex removal and membrane peeling
- Differential degeneration of rod/cone bipolar cells during retinal degeneration in Royal College of Surgeons rats