
年龄相关性血管硬度与血压的关系研究
2016-09-05 03:04房加雄李敬华
实用心脑肺血管病杂志 2016年2期
姬 乐,房加雄,郁 鹏,李敬华
·论著·
年龄相关性血管硬度与血压的关系研究
姬 乐,房加雄,郁 鹏,李敬华
目的探讨年龄相关性血管硬度与血压的关系。方法选取2014年6月—2015年6月在天津市西青医院进行健康体检者504例,根据年龄分为青年组(≤44岁,n=82)、中年组(45~59岁,n=230例)、老年组(60~79岁,n=135例)和高龄组(≥80岁,n=57)。比较各组受试者血压及血管硬度,并分析血管硬度与血压的关系。结果青年组高血压检出率为20.73%(17/82),中年组为32.61%(75/230),老年组为42.22%(57/135),高龄组为43.86%(25/57)。高龄组、老年组和中年组受试者收缩压和脉压高于青年组,高龄组和老年组受试者收缩压和脉压高于中年组(P<0.05);但老年组和高龄组受试者收缩压和脉压比较,差异无统计学意义(P>0.05);各组受试者舒张压比较,差异无统计学意义(P>0.05)。高龄组、老年组和中年组受试者左侧踝臂脉搏波传导速度(baPWV)和右侧baPWV均高于青年组,高龄组和老年组受试者左侧baPWV和右侧baPWV均高于中年组,高龄组受试者左侧baPWV和右侧baPWV均高于老年组(P<0.01);高龄组、老年组和中年组受试者左侧踝臂指数(ABI)和右侧ABI均高于青年组,高龄组受试者左侧ABI高于中年组、老年组(P<0.01)。Pearson相关性分析结果显示,年龄与左侧baPWV和右侧baPWV均呈正相关(r值分别为0.531、0.556,P<0.01);而年龄与左侧ABI和右侧ABI均无直线相关性(r值分别为0.137、0.004,P>0.05)。Mantel-Haenszel卡方检验结果显示,右侧baPWV与高血压分级无关(χ2=1 229.67,P=0.355),左侧baPWV与高血压分级亦无关(χ2=1 239.35,P=0.277);右侧ABI(χ2=419.81)和左侧ABI(χ2=351.59)均与高血压分级有关(P<0.001)。结论随着年龄增长,血管硬度增加、收缩压升高,且血管硬度与血压有关。
血管硬化;年龄因素;血压;踝臂脉搏波传导速度;踝臂指数
姬乐,房加雄,郁鹏,等.年龄相关性血管硬度与血压的关系研究[J].实用心脑肺血管病杂志,2016,24(2):32-35.[www.syxnf.net]
Ji L,Fang JX,Yu P,et al.Relationship between age-related vascular hardness and blood pressure[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2016,24(2):32-35.
年龄是心血管疾病的独立危险因素,且随着年龄增加高血压患病率明显升高。有研究显示,60~69岁人群高血压患病率为50%以上,70岁以上人群高血压患病率为75%;55~65岁血压正常者到80岁以后90%患有高血压[1]。临床研究显示,高血压与动脉粥样硬化(atherosclerosis,AS)存在明显相关性,且与年龄相关的大动脉顺应性减低、血管硬度增加是老年收缩期高血压的危险因素之一[2]。本研究旨在探讨年龄相关性血管硬度与血压的关系,旨在为老年高血压患者的治疗及预防提供参考。
1 资料与方法
1.1一般资料选取2014年6月—2015年6月在天津市西青医院进行健康体检者504例,排除继发性高血压、大动脉炎、下肢动脉硬化性闭塞、慢性肝肾功能不全、结缔组织疾病、糖尿病神经病变及其他周围血管疾病患者。其中男242例,女262例;年龄17~84岁,平均年龄(55.3±11.8)岁。根据年龄将受试者分为青年组(≤44岁,n=82)、中年组(45~59岁,n=230例)、老年组(60~79岁,n=135例)和高龄组(≥80岁,n=57)。
1.2检测方法
1.2.1一般资料采集记录受试者性别、身高、体质量、体质指数(BMI)及心率。受试者穿薄衣物,不穿鞋,用已校准的台式身高体重称〔精度:±1 cm(身高),±0.5 kg(体质量)〕测量身高、体质量,测量两次后取平均值,并计算BMI。
1.2.2血压检测方法受试者休息15 min 后采用标准袖带水银柱式血压计测量坐位右臂血压,以Korotkoff Ⅰ音的血压读数作为收缩压,Korotkoff Ⅴ音的血压读数作为舒张压,间隔2 min 测量1次,测量3次取平均值。
1.2.3踝臂脉搏波传导速度(baPWV)检测方法受试者休息5 min后戴好上臂箍带、脚踝箍带、心电图夹和心音传感器,输入受检者年龄、性别、身高、体质量,使用欧姆龙/科林动脉硬化检测仪(VP-1000),采用振荡法,使用线性膨胀技术,准确检出四肢的脉搏波形并测出左侧baPWV和右侧baPWV。
1.2.4踝臂指数(ABI)检测方法受试者休息5 min后使用欧姆龙/科林动脉硬化检测仪(VP-1000),采用示波测量技术同步测量双上肢动脉和双侧胫后动脉和/或足背动脉的收缩压,并计算左侧ABI和右侧ABI。
1.3观察指标比较各组受试者一般资料、血压及血管硬度,并分析血管硬度与血压的关系。

2 结果
2.1一般资料各组受试者性别、身高、BMI、体质量比较,差异有统计学意义(P<0.05);但心率比较,差异无统计学意义(P>0.05,见表1)。
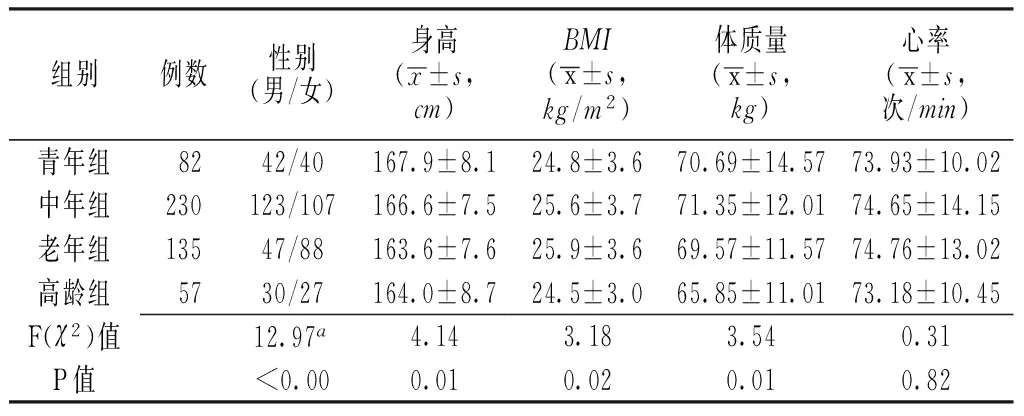
表1 各组受检者一般资料比较
注:a为χ2值;BMI=体质指数
2.2血压变化青年组高血压检出率为20.73%(17/82),中年组为32.61%(75/230),老年组为42.22%(57/135),高龄组为43.86%(25/57)。各组受试者高血压检出率、高血压分级、收缩压及脉压比较,差异有统计学意义(P<0.05);但舒张压比较,差异无统计学意义(P>0.05)。高龄组、老年组和中年组受试者收缩压和脉压高于青年组,高龄组和老年组受试者收缩压和脉压高于中年组,差异有统计学意义(P<0.05);但老年组和高龄组受试者收缩压和脉压比较,差异无统计学意义(P>0.05,见表2)。
表2各组受试者高血压分级及血压比较
Table 2Comparison of hypertension grading and blood pressure in each group
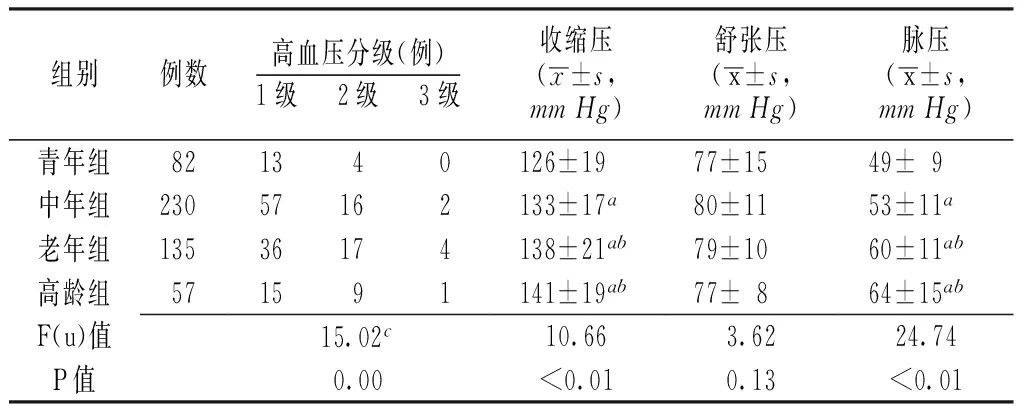
组别例数高血压分级(例)1级 2级 3级收缩压(x±s,mmHg)舒张压(x±s,mmHg)脉压(x±s,mmHg)青年组821340126±1977±1549±9中年组23057162133±17a80±1153±11a老年组13536174138±21ab79±1060±11ab高龄组571591141±19ab77±864±15abF(u)值15.02c10.663.6224.74P值0.00<0.010.13<0.01
注:与青年组比较,aP<0.05;与中年组比较,bP<0.05;c为u值;1 mm Hg=0.133 kPa
2.3血管硬度指标各组受试者左侧baPWV、右侧baPWV、左侧ABI及右侧ABI比较,差异有统计学意义(P<0.05)。高龄组、老年组和中年组受试者左侧baPWV和右侧baPWV均高于青年组,高龄组和老年组受试者左侧baPWV和右侧baPWV均高于中年组,高龄组受试者左侧baPWV和右侧baPWV均高于老年组,差异有统计学意义(P<0.01);高龄组、老年组和中年组受试者左侧ABI和右侧ABI均高于青年组,高龄组受试者左侧ABI高于中年组、老年组,差异有统计学意义(P<0.01,见表3)。Pearson相关性分析结果显示,年龄与左侧baPWV和右侧baPWV均呈正相关(r值分别为0.531、0.556,P<0.01,见图1);而年龄与左侧ABI和右侧ABI均无直线相关性(r值分别为0.137、0.004,P>0.05,见图2)。
表3 各组受试者baPWV和ABI比较
注:baPWV=踝臂脉搏波传导速度,ABI=踝臂指数;与青年组比较,aP<0.05;与中年组比较,bP<0.05;与老年组比较,cP<0.05

注:baPWV=踝臂脉搏波传导速度
图1年龄与双侧baPWV相关性的散点图
Figure 1Scatter diagram for correlation between age and bilateral baPWV

注:ABI=踝臂指数
图2年龄与双侧ABI相关性的散点图
Figure 2Scatter diagram of for correlation between age and bilateral ABI
2.4血管硬度与血压的关系Mantel-Haenszel卡方检验结果显示,右侧baPWV与高血压分级无关(χ2=1 229.67,P=0.355),左侧baPWV亦与高血压分级无关(χ2=1 239.35,P=0.277);右侧ABI(χ2=419.81)和左侧ABI(χ2=351.59)均与高血压分级有关(P<0.001)。
3 讨论
随着年龄增长机体功能逐渐下降,尤其是老年人,随着年龄增长易导致心血管系统发生病变,因此了解年龄相关性心血管疾病及其防治措施具有重要的临床意义[1-2]。ABI是足踝动脉收缩压与肱动脉收缩压的比值[3],是反映AS的重要指标之一,正常情况下该值大于1.0,当ABI<0.9时提示下肢血管通畅性受阻,即发生末梢血管疾病(peripheral arterial disease)[4-5]。baPWV是脉搏波传导速度(PWV)的检测方法之一,其能反映中央弹性动脉的僵硬度。临床研究显示,baPWV和ABI能有效反映动脉硬化情况,且两者对AS[6-7]、末梢血管病变[3-4,8-9]、脑卒中[10]及单纯收缩期高血压[11]等具有预测价值。
本研究选择504例健康体检者作为研究对象,旨在探讨年龄相关性血管硬度与血压的关系。结果显示,各组受试者高血压检出率、高血压分级、收缩压及脉压比较有差异,但舒张压间无差异,随着年龄增长baPWV逐渐增加,且年龄与左、右两侧baPWV呈正相关,提示与年龄相关的血压变化多为收缩期高血压,且年龄增加可导致血管硬化。Gu等[9]研究显示,高血压患者baPWV高于正常人群,且左右侧ABI与血压变化相关。本研究结果亦显示,左侧baPWV和右侧baPWV与高血压分级间无关系;左侧ABI和右侧ABI与高血压分级间有关系,提示血管硬度与血压有关。分析原因可能为随着年龄增长,动脉管壁结构、功能发生改变,导致管壁硬度增加,血管顺应性及弹性降低,致使收缩压升高、舒张压下降。血管硬度增加导致收缩期高血压的主要原因如下:(1)血管壁结构发生变化,主动脉及其主要分支动脉内膜增厚,胶原蛋白增多,弹力纤维发生变性和断裂,血管中层出现钙和脂质沉积,导致血管壁硬度增高,血管顺应性下降。当心室收缩射血时,主动脉不能有效扩张,对血压升高的缓冲降低,致使收缩期血压升高。(2)血管壁功能改变主要表现为大动脉弹性减退、脉搏波传导速度增快、反射波抵达中心大动脉的时相从舒张期提前到收缩期,出现收缩期延迟压力波峰,从而导致收缩压升高、舒张压降低、脉压增大。无论是单纯动脉血压升高引起功能性动脉管壁张力增加,还是动脉结构改变,其共同结果是导致动脉弹性降低、收缩压峰值增大、舒张压降低、脉压增大。
综上所述,随着年龄增长血管硬度逐渐增加,且血管硬度变化与血压有一定关系,血管硬度增加可能是老年单纯收缩期高血压的高发原因之一。因此,干预年龄相关性血管硬度可能对预防老年收缩期高血压具有一定作用。但由于老年人血压升高还可能受遗传、饮食习惯、生活环境、压力等多种因素影响,因此临床应排除其他因素的干扰进一步探究年龄相关性血管硬度变化影响血压变化的作用机制。
作者贡献:姬乐进行实验设计与实施、资料收集整理、撰写论文、成文并对文章负责;房家雄、郁鹏进行实验实施、评估、资料收集;李敬华进行质量控制及审校。
本研究所纳入的研究对象为姬乐在天津市西青医院实习时收集,并获得天津市西青医院伦理委员会批准实施,无利益冲突。
[1]李贺,李郭,李钟,等.老年人群心、脑血管病的特殊性及防治[J].武警医学,2010,21(2):163-166.
[2]李贺,李玉明,周欣.老年人心血管系统变化及对心血管疾病防治的影响[J].中华老年心脑血管病杂志,2009,11(5):389-391.
[3]Aboyans V,Criqui MH,Abraham P,et al.Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association[J].Circulation,2012,126(24):2890-2909.
[4]Nexoe J,Damsbo B,Lund JO,et al.Measurement of blood pressure,ankle blood pressure and calculation of ankle brachial index in general practice[J].Fam Pract,2012,29(3):345-351.
[5]Jones DW,Hall JE.Seventh report of the Joint National Committee on prevention,detection,evaluation,and treatment of high blood pressure and evidence from new hypertension trials[J].Hypertension,2003,42(6):1206-1252.
[6]刘严,齐丽彤,马为,等.中老年人体测量学指标与动脉硬化指标的关系[J].北京大学学报,2014,46(3):455-459.
[7]张继英 郇志华,庞志刚,等.心-踝血管指数——动脉粥样硬化无创检测指标:845例分析[J].中华老年多器官疾病杂志,2012,11(2):122-125.
[8]Chen PY,Lawford KM,Shah N,et al.Perceptions of the ankle brachial index amongst podiatrists registered in Western Australia[J].J Foot Ankle Res,2012,5(1):19.
[9]Gu X,Zhao L,Zhu J,et al.Serum Mimecan Is Associated With Arterial Stiffness in Hypertensive Patients[J].J Am Heart Assoc,2015.pii: e002010.doi: 10.1161/JAHA.115.002010.
[10]Zhang Y,Chen J,Zhang K,et al.Combination of high ankle-brachial index and hard coronary heart disease Framingham Risk Score in predicting the risk of ischemic stroke in general population[J].PLoS One,2014,9(9):e106251.
[11]Zhang Y,Chen J,Zhang K,et al.Inflammation and oxidative stress are associated with the prevalence of high aankle-brachial index in metabolic syndrome patients without chronic renal failure[J].Int J Med Sci,2013,10(2):183-190.
(本文编辑:谢武英)
Relationship Between Age-related Vascular Hardness and Blood Pressure
JILe,FANGJia-xiong,YUPeng,etal.
TianjinUniversityofTraditionalChineseMedicine,Tianjin300193,China
ObjectiveTo investigate the relationship between age-related vascular hardness and blood pressure.MethodsFrom June 2014 to June 2015,a total of 504 cases admitted to Xiqing Hospital for physical examination were collected,and they were divided into A group(below or equal 44 years old,n=82),B group(between 45 and 59 years old,n=230),C group(between 60 and 79 years old,n=135)and D group(equal or over 80 years old,n=57)according to age.Blood pressure and vascular hardness were compared among the four groups,and relationship between vascular hardness and blood pressure was analyzed.ResultsThe detection rate of hypertension of A group was 20.73%(17/82),of B group was 32.61%(75/230),of C group was 42.22%(57/135),of D group was 43.86%(25/57).SBP and pulse pressure of B group,C group and D group were statistically significantly higher than those of A group,SBP and pulse pressure of C group and D group were statistically significantly higher than those of B group(P<0.05);while no statistically significant differences of SBP or pulse pressure was found between C group and D group,nor was DBP among the four groups(P>0.05).Left-side baPWV and right-side baPWV of B group,C group and D group were statistically significantly higher than those of A group,left-side baPWV and right-side baPWV of C group and D group were statistically significantly higher than those of B group,left-side baPWV and right-side baPWV of D group were statistically significantly higher than those of C group(P<0.01).Left-side ABI and right-side ABI of B group,C group and D group were statistically significantly higher than those of A group,left-side ABI and right-side ABI of D group were statistically significantly higher than those of B group and C group(P<0.01).Pearson correlation analysis showed that,age was positively correlated with left-side baPWV(r=0.531,P<0.01)and right-side baPWV(r=0.556,P<0.01),while age was not linearly correlated with left-side ABI(r=0.137,P>0.05)or right-side ABI(r=0.004,P>0.05).Mantel-Haenszel chi-square test results showed that,right-side baPWV(χ2=1 229.67,P=0.355)or left-side baPWV(χ2=1 239.35,P=0.277)was not correlated with hypertension grading,while right-side ABI(χ2=419.81) and left-side ABI(χ2=351.59)were correlated with hypertension grading(P<0.001).ConclusionAs the increasing of age,the vascular hardness and SBP elevated,and vascular hardness has certain correlation with blood pressure.
Vascular stiffness;Age factors;Blood pressure;Ankle brachial pulse wave velocity;Ankle brachial index
300193天津市,天津中医药大学(姬乐,郁鹏);武警后勤学院附属医院(姬乐,房加雄,郁鹏,李敬华)
李敬华,300162天津市,武警后勤学院附属医院;E-mail:lijingh1020@163.com
R 544
A
10.3969/j.issn.1008-5971.2016.02.009
2015-10-18;
2016-01-12)
猜你喜欢
心肺血管病杂志(2019年1期)2019-04-22
家庭科学·新健康(2018年5期)2018-06-08
中国新闻周刊(2017年16期)2017-06-15
中国循证心血管医学杂志(2017年11期)2017-01-12
冰雪运动(2016年4期)2016-04-16
中国循环杂志(2015年10期)2015-12-24
中国当代医药(2015年7期)2015-03-01
中国民族民间医药·下半月(2014年1期)2015-02-02
重庆医学(2014年14期)2014-08-14
中国全科医学(2014年15期)2014-02-27
