不同肠道病毒感染手足口病患儿病毒载量及临床特征对比分析
2016-07-19 11:31杜潘艳王宝林高翠红
中国全科医学 2016年18期
关键词:手足口病
陈 苏,杜潘艳,郑 红,王宝林,高翠红,张 双
不同肠道病毒感染手足口病患儿病毒载量及临床特征对比分析
陈 苏,杜潘艳,郑 红,王宝林,高翠红,张 双
063000河北省唐山市第四医院检验科(陈苏);唐山市妇幼保健院检验科(杜潘艳,郑红,王宝林,高翠红,张双)
【摘要】目的对比分析肠道病毒71型(EV71)与柯萨奇A组16型(CoxA16)感染手足口病(HFMD)患儿的病毒载量及临床特征。方法收集2015年5—9月唐山市妇幼保健院儿科确诊的HFMD患儿430例,根据临床症状、体征和病毒种类将患儿分为EV71轻度组162例、EV71重度组87例、CoxA16轻度组158例、CoxA16重度组23例。采用实时荧光定量反转录PCR技术检测患儿咽拭子EV71、CoxA16 RNA,计算病毒载量;记录患儿的病程、体温、热程、口腔溃疡、流涎、咳嗽、手部出疹、足部出疹、嗜睡、惊厥、呕吐、意识改变、肢体抖动、肌痉挛情况。结果标准曲线显示循环阈值(Ct值)与病毒载量的对数呈高度负相关(r=-1.000,P<0.01)。Ct值(X)与病毒载量的对数(Y)的关系为Y=-0.29X+13.03。CoxA16轻度组、CoxA16重度组HFMD患儿Ct值较EV71轻度组、EV71重度组降低(P<0.05);EV71轻度组与EV71重度组、CoxA16轻度组与CoxA16重度组HFMD患儿Ct值比较,差异无统计学意义(P>0.05)。EV71重度组、CoxA16重度组HFMD患儿病程较EV71轻度组、CoxA16轻度组延长(P<0.05);EV71重度组HFMD患儿病程较CoxA16重度组延长(P<0.05)。4组HFMD患儿体温≥38.5 ℃、口腔溃疡、流涎、手部出疹、足部出疹发生率比较,差异均无统计学意义(P>0.05)。EV71重度组、CoxA16重度组HFMD患儿热程≥3 d发生率较EV71轻度组、CoxA16轻度组升高(P<0.007);EV71重度组、CoxA16重度组HFMD患儿体温≥38.5 ℃+热程≥3 d发生率较EV71轻度组、CoxA16轻度组升高,EV71轻度组HFMD患儿体温≥38.5 ℃+热程≥3 d发生率较CoxA16轻度组升高,EV71重度组HFMD患儿体温≥38.5 ℃+热程≥3 d发生率较CoxA16重度组升高(P<0.007);CoxA16轻度组、CoxA16重度组HFMD患儿咳嗽、手部出疹数≥15个(双手)、足部出疹数≥15个(双足)发生率较EV71轻度组、EV71重度组升高(P<0.007)。EV71重度组、CoxA16重度组HFMD患儿嗜睡、呕吐发生率较EV71轻度组升高,EV71重度组HFMD患儿嗜睡发生率较CoxA16重度组升高(P<0.01)。结论HFMD患儿病毒载量与感染病毒相关,但不同病情程度间病毒载量无差别。不同病毒感染及病情程度患儿间热程≥3 d、体温≥38.5 ℃+热程≥3 d、咳嗽、手部出疹数≥15个(双手)、足部出疹数≥15个(双足)、嗜睡、惊厥、呕吐、意识改变、肢体抖动、肌阵挛发生率有差异。
【关键词】手足口病;肠道病毒属;柯萨奇病毒感染;病毒载量;体征和症状
陈苏,杜潘艳,郑红,等.不同肠道病毒感染手足口病患儿病毒载量及临床特征对比分析[J].中国全科医学,2016,19(18):2211-2215.[www.chinagp.net]
Chen S,Du PY,Zheng H,et al.Analysis of the viral load and clinical features of children with hand,foot and mouth disease by different enteroviruses[J].Chinese General Practice,2016,19(18):2211-2215.
手足口病(hand,foot and mouse disease,HFMD)是一种易感染低龄儿童的急性传染病,病原体以肠道病毒71型(enterovirus 71,EV71)和柯萨奇A组16型(coxsackievirus,CoxA16)最为常见,而EV71感染常会引起严重的神经系统症状[1]。两种病原体感染与病毒载量及引起的临床特征是否有关,目前关于此方面的研究较少。因此,本研究分析EV71和CoxA16感染HFMD患儿病毒载量及临床特征的差异,旨在为临床诊疗和致病机制的研究提供依据。
1资料与方法

1.2方法
1.2.1标本采集及处理规范采集患儿入院当日咽拭子标本,在装有3~5 ml 0.9%氯化钠溶液采样管中充分搅动,得液态标本,密封,用于EV71、CoxA16 RNA检测。
1.2.2EV71、CoxA16 RNA检测EV71、CoxA16 RNA检测引物和试剂盒均采用上海科华生物工程股份有限公司产品。严格按说明书分别对液态标本进行预处理,EV71、CoxA16 RNA提取及PCR扩增检测。设置循环条件为:反转录50 ℃ 25 min,1个循环;预变性94 ℃ 2 min,1个循环; 预扩增95 ℃ 10 s→55 ℃ 15 s→72 ℃ 15 s,5个循环;扩增、检测95 ℃ 10 s→60 ℃ 40 s,40个循环。实时荧光定量反转录PCR(RT-qPCR)法扩增曲线阳性结果判定标准:在阴性、阳性质控均满足要求的条件下,阳性标本扩增曲线呈典型S型且循环阈值(Ct值)<36.0,阴性标本无典型的S型扩增曲线或无Ct值。
1.2.3病毒载量检测检测已知浓度标准品的Ct值,在对数坐标纸上以标准品的浓度为纵坐标,标准品的Ct值为横坐标,绘制标准曲线。通过标本的Ct值在标准曲线上得出各待测标本的浓度即为标本的病毒载量。
1.2.4临床资料采用回顾性分析方法,记录患儿的病程、体温、热程、口腔溃疡、流涎、咳嗽、手部出疹、足部出疹、嗜睡、惊厥、呕吐、意识改变、肢体抖动、肌痉挛情况。

2结果
2.1EV71、CoxA16 RNA检测结果HFMD患儿RT-qPCR法扩增曲线及标准曲线见图1。标准曲线显示,Ct值与病毒载量的对数呈高度负相关(r=-1.000,P<0.01)。Ct值(X)与病毒载量的对数(Y)的关系为:Y=-0.29X+13.03。阳性临界对照循环曲线呈S型,Ct值为34.6,病毒载量为1.02×103copies/ml;阳性标本Ct值为20.8,病毒载量为1.01×107copies/ml;阴性标本未检出病毒,Ct值>40.0。
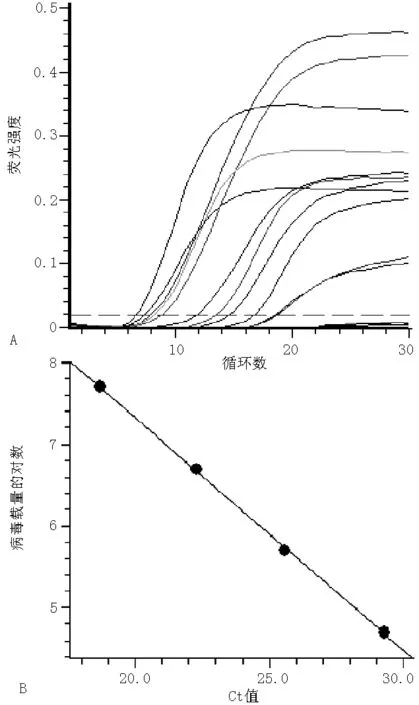
注:Ct值=循环阈值;A为扩增曲线,B为标准曲线
图1HFMD患儿RT-qPCR法扩增曲线及标准曲线
Figure 1Amplification and standard curve of real-time fluorescent quantitative RT-PCR on children with HFMD
2.2不同组间Ct值比较EV71轻度组、EV71重度组、CoxA16轻度组、CoxA16重度组HFMD患儿Ct值比较,差异有统计学意义(P<0.05);其中CoxA16轻度组、CoxA16重度组HFMD患儿Ct值较EV71轻度组、EV71重度组降低,差异有统计学意义(P<0.05);EV71轻度组与EV71重度组、CoxA16轻度组与CoxA16重度组HFMD患儿Ct值比较,差异无统计学意义(P>0.05,见表1)。
2.3不同组间患儿临床特征比较EV71轻度组、EV71重度组、CoxA16轻度组、CoxA16重度组HFMD患儿病程分别为(9.0±3.1)d、(14.6±3.2)d、(8.7±2.2)d、(12.6±3.0)d,差异有统计学意义(F=101.59,P<0.001);其中EV71重度组、CoxA16重度组HFMD患儿病程较EV71轻度组、CoxA16轻度组延长,差异有统计学意义(P<0.05);EV71重度组HFMD患儿病程较CoxA16重度组延长,差异有统计学意义(P<0.05)。4组HFMD患儿体温≥38.5 ℃、口腔溃疡、流涎、手部出疹、足部出疹发生率比较,差异均无统计学意义(P>0.05)。EV71重度组、CoxA16重度组HFMD患儿热程≥3 d发生率较EV71轻度组、CoxA16轻度组升高,差异有统计学意义(P<0.007);EV71重度组、CoxA16重度组HFMD患儿体温≥38.5 ℃+热程≥3 d发生率较EV71轻度组、CoxA16轻度组升高,EV71轻度组HFMD患儿体温≥38.5 ℃+热程≥3 d发生率较CoxA16轻度组升高,EV71重度组HFMD患儿体温≥38.5 ℃+热程≥3 d发生率较CoxA16重度组升高,差异有统计学意义(P<0.007);CoxA16轻度组、CoxA16重度组HFMD患儿咳嗽、手部出疹数≥15个(双手)、足部出疹数≥15个(双足)发生率较EV71轻度组、EV71重度组升高,差异有统计学意义(P<0.007)。EV71重度组、CoxA16重度组HFMD患儿嗜睡、呕吐发生率较EV71轻度组升高,EV71重度组HFMD患儿嗜睡发生率较CoxA16重度组升高,差异有统计学意义(P<0.01)。EV71重度组HFMD患儿惊厥、意识改变、肢体抖动、肌阵挛发生率与CoxA16重度组比较,差异无统计学意义(P>0.05,见表2)。
3讨论
HFMD一年四季均可发病,以夏季及秋季高发。传染源为患者和病毒携带者,病毒主要通过呼吸道和消化道传播。迄今为止发现能够引发HFMD的肠道病毒有20余种,而实验室多以检测EV71和CoxA16两种病毒为主。目前,病毒核酸检测多采用PCR技术,而本研究所采用的反转录PCR(RT-qPCR)方法较普通RT-PCR方法更灵敏、快捷,且能够直观地显示病毒载量[3]。本研究根据临床症状、体征和病毒种类将患儿分为EV71轻度组162例、EV71重度组87例、CoxA16轻度组158例、CoxA16重度组23例,CoxA16轻度组、CoxA16重度组HFMD患儿Ct值较EV71轻度组、EV71重度组降低,EV71轻度组与EV71重度组、CoxA16轻度组与CoxA16重度组HFMD患儿Ct值无差异,提示病毒载量与感染病毒相关,而与病情程度无关,与已有研究相符[4-5]。
表1 不同组间HFMD患儿Ct值比较
注:EV71=肠道病毒71型,CoxA16=柯萨奇A组16型,Ct值=循环阈值;与EV71轻度组比较,aP<0.05;与EV71重度组比较,bP<0.05
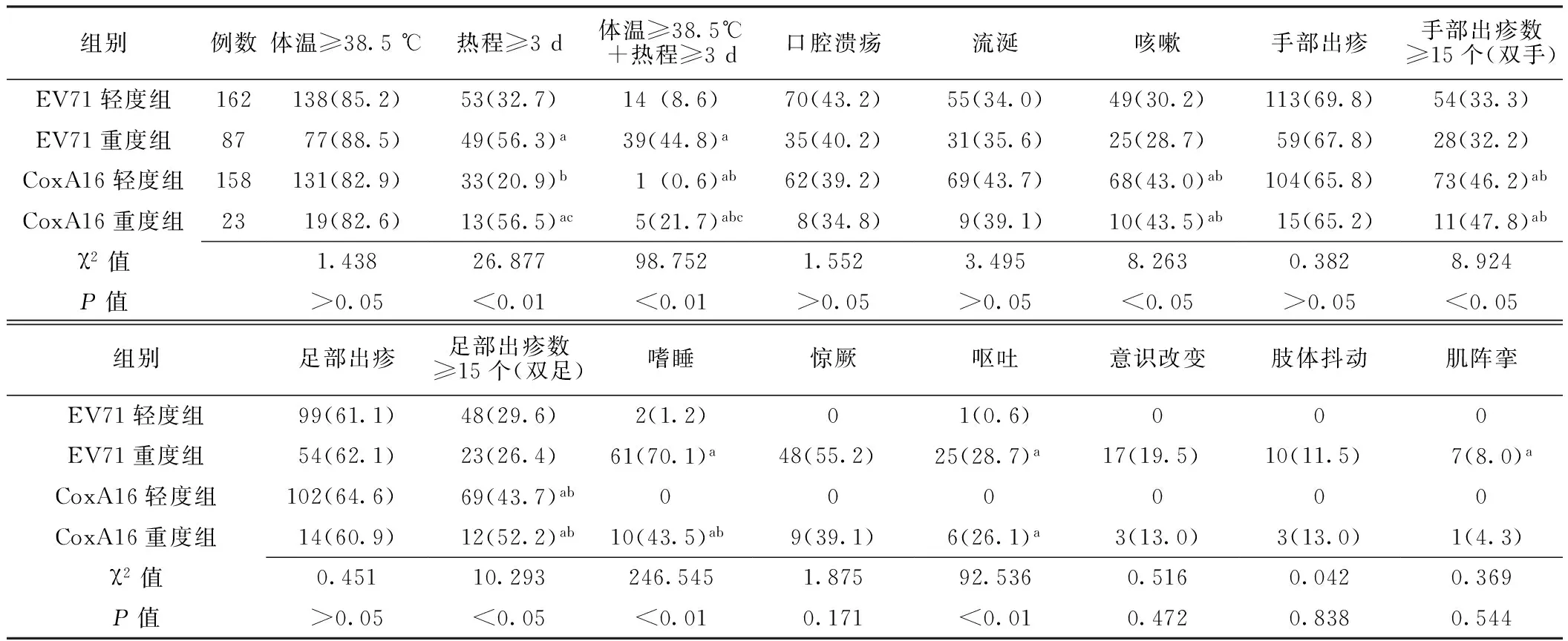
表2 不同组间HFMD患儿临床特征比较〔n(%)〕
注:与EV71轻度组比较,aP<0.007;与EV71重度组比较,bP<0.007;与CoxA16重度组比较,cP<0.007
HFMD起病急、病情发展迅速、临床表现多样,重度患儿可合并无菌性脑膜炎、脑炎、脊髓灰质炎性麻痹、神经源性肺水肿等中枢神经系统疾病,如不及时治疗,极易危及生命[6]。国内外学者将临床特征作为判断重度患儿的危险因素,以及时发现和控制重症的发生发展[7-8]。本研究通过病例资料整理分析发现,两种病毒感染均有发热、口腔溃疡、流涎、手部出疹、足部出疹等临床症状。而重度患儿可出现嗜睡、惊厥、呕吐、意识改变、肢体抖动、肌阵挛等早期神经系统受累表现[9],病程和热程均较长,而体温≥38.5 ℃+热程≥3 d在EV71重度患儿表现尤为明显,可作为重度患儿的危险因素之一;CoxA16感染患儿的临床表现主要是咳嗽,手、足部出疹数多,提示CoxA16感染对皮肤黏膜的损伤较明显,少数CoxA16感染患儿也可出现神经系统受累表现。既往研究发现,病毒载量与临床特征无关,临床表现的复杂性与所感染病毒的种类存在一定的关联性[9-10]。
综上所述,尽管病毒载量与病情程度无关,但病毒载量的监测有助于临床及时掌握患儿的病毒复制情况,本研究发现不同的病毒种类引起宿主不同的临床表现,因此对病毒种类及病毒载量的及时检测对临床诊疗、病情监测和重度患儿的预防控制有重要意义。有研究表明,HFMD患儿复杂的临床表现可能与宿主的免疫防御功能和病毒的生物学特性有关[11],而同一肠道病毒中包括不同基因型,本课题组将进一步扩大样本量,分析HFMD患儿不同的临床特征与肠道病毒基因型间的关系。
作者贡献:陈苏、杜潘艳进行试验设计与实施、资料收集整理、撰写论文、成文并对文章负责;郑红、王宝林、高翠红进行试验实施、评估、资料收集;张双进行质量控制及审校。
本文无利益冲突。
参考文献
[1]Ma E,Chan KC ,Cheng P,et al.The enterovirus 71 epidemic in 2008--public health implications for Hong Kong[J].Int Infection Dis,2010,14(9):e775-780.
[2]卫生部办公厅关于印发《手足口病诊疗指南(2010年版)》的通知[EB/OL].(2010-04-06)[2010-06-01].http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohyzs/s3586/202004/46884.htm.
[3]Zhang S,Wang J,Yan Q,et al.A one-step,triplex,real-time RT-PCR assay for the simultaneous detection of enterovirus 71,coxsackie A16 and pan-enterovirus in a single tube[J].PLoS One,2014,9(7):e102724.
[4] Deng HL,Zhang Y,Xie Y,et al.Virus load of enterovirus 71 and the severity of hand-foot-mouth disease caused by enterovirus 71[J].Journal of Applied Clinical Pediatrics,2014,29(22):1700-1702.(in Chinese)
邓慧玲,张瑜,谢燕,等.肠道病毒71型病毒载量与手足口病严重程度分析[J].中华实用儿科临床杂志,2014,29(22):1700-1702.
[5] Wang ZM,Teng S,Shao QM,et al.Correlation of virus load of enterovirus 71 and the severity of hand-foot-mouth disease [J].Zhejiang Clinical Medical Journal,2014,16(11):1723-1725.(in Chinese)
王忠敏,滕淑,邵启民,等.EV71病毒载量与手足口病病情严重程度的相关性[J].浙江临床医学,2014,16(11):1723-1725.
[6]Xie GJ,Xie FY,Zhang GF,et al.Comparison of the main clinical manifestations and outcomes of hand,foot,and mouth disease caused by enterovirus 71 and coxsackievirus A16 infection [J].ACTA Medicinalis Universitatis Nanjing(Natural Science),2011,31(10): 1436-1439.(in Chinese)
谢国锦,谢芳艺,张国锋,等.人肠道病毒71型和科萨奇病毒A组16型所致手足口病的主要临床表现和预后[J].南京医科大学学报:自然科学版,2011,31(10): 1436-1439.
[7] Wang Q,Zhang W,Zhang Y,et al.Clinical features of severe cases of hand,foot and mouth disease with EV71 virus infection in China[J].Arch Med Sci,2014 ,10(3):510-516.
[8] Nguyen NT,Pham HV,Hoang CQ,et al.Epidemiological and clinical characteristics of children who died from hand,foot and mouth disease in Vietnam,2011[J].BMC Infect Dis,2014,14: 341.
[9] Gao YY,Yang SD,Tao JP,et al.Clinical features and critical illness risk factors of children with hand,foot and mouth disease of neurological invovment [J].Chinese Journal of Evidence-based Pediatrics,2010,5(2):135-140.(in Chinese)
高媛媛,杨思达,陶建平,等.累及神经系统手足口病患儿临床特征及危重症危险因素分析[J].中国循证儿科杂志,2010,5(2):135-140.
[10] Huang Y,Zhou Y,Lu H,et al.Characterization of severe hand,foot and mouth disease in Shenzhen,China,2009-2013[J].J Med Virol,2015,87(9):1471-1479.
[11]Bian PF.Etiology,clinical characteristics and immunological studies in severe patients with hand,foot and mouth disease [D].Ji′nan:Shandong University,2012.(in Chinese)
边鹏飞.重症手足口病病原学与临床特征、机体免疫状态关系的研究[D].济南:山东大学,2012.
(本文编辑:陈素芳)
Analysis of the Viral Load and Clinical Features of Children With Hand,Foot and Mouth Disease by Different Enteroviruses
CHENSu,DUPan-yan,ZHENGHong,etal.
DepartmentofLaboratory,theFourthHospitalofTangshan,Tangshan063000,China
【Abstract】ObjectiveTo analyze the viral load and clinical features of children with hand,foot and mouth disease(HFMD) by EV71 and CoxA16.MethodsA total of 430 children who were definitely diagnosed with HFMD in the Department of Pediatrics in Tangshan Women and Children Health-care Hospital from May to September in 2015 were enrolled.According to clinical symptoms,physical signs and species of virus,the children were divided into EV71 mild group(162 cases),EV71 severe group(87 cases),CoxA16 mild group(158 cases)and CoxA16 severe group(23 cases).Throat swabs of the children were collected and the RNA of EV71 and CoxA16 was detected by real-time fluorescent quantitative RT-qPCR method,and viral load was calculated.Length of disease,temperature,length of fever,dental ulcer,salivation,cough,hand rash,foot rash,somnolence,convulsion,vomit,change of consciousness,limb jitter,and myospasm of the children were recorded.ResultsCycle threshold(Ct value) shown by standard curve had highly negative correlation with the viral load(r=-1.000,P<0.01).The relation between the Ct value(X) and the logarithm of viral load(Y) was Y=-0.29X+13.03.CoxA16 mild group and CoxA16 severe group were lower than EV71 mild group and EV71 severe group in Ct value (P<0.05).There was no significant difference in the Ct value of HFMD children between EV71 mild group and EV71 severe group and between CoxA16 mild group and CoxA16 severe group(P>0.05).EV71 severe group and CoxA16 severe group had longer length of disease than EV71 mild group and CoxA16 mild group (P<0.05).EV71 severe group had longer length of disease than CoxA16 severe group (P<0.05).The four groups were not significantly different in the incidence rates of temperature ≥38.5 ℃,dental ulcer,salivation,hand rash and foot rash(P>0.05).EV71 severe group and CoxA16 severe group had higher incidence rate of the length of fever ≥3 d than EV71 mild group and CoxA16 mild group (P<0.007).EV71 severe group and CoxA16 severe group had higher incidence rate of temperature ≥38.5 ℃ plus length of fever ≥3 d than EV71 mild group and CoxA16 mild group,EV71 mild group was higher than CoxA16 mild group in the incidence rate of temperature ≥38.5 ℃ plus length of fever ≥3 d,and EV71 severe group was higher than CoxA16 severe group in the incidence rate of temperature ≥38.5 ℃ plus length of fever ≥3 d(P<0.007).CoxA16 mild group and CoxA16 severe group had higher incidence rates of cough,the number of hand rashes ≥15(both hands) and the number of foot rashes ≥15(both feet) than EV71 mild group and EV71 severe group(P<0.007).EV71 severe group and CoxA16 severe group had higher incidence rates of somnolence and vomit than EV71 mild group, and EV71 severe group was higher than CoxA16 severe group in the incidence rates of somnolence(P<0.01).ConclusionThe viral load of HFMD children varies with different types of enterovirus but is not different among different disease severity levels.HFMD children with different types of enterovirus and disease severity levels are different in the incidence rates of length of fever ≥3 d,temperature ≥38.5 ℃ plus length of fever ≥3 d,cough,the number of hand rashes ≥15(both hands) and the number of foot rashes ≥15(both feet),somnolence,convulsion,vomit,change of consciousness,limb jitter and myospasm.
【Key words】Hand,foot and mouth disease;Enterovirus;Coxsackievirus infections;Viral load;Signs and symptoms
通信作者:杜潘艳,063000河北省唐山市妇幼保健院检验科;E-mail:dpy405@sohu.com
【中图分类号】R 725.1
【文献标识码】B
doi:10.3969/j.issn.1007-9572.2016.18.020
(收稿日期:2015-11-12;修回日期:2016-02-22)
·临床诊疗提示·
猜你喜欢
现代养生·下半月(2016年5期)2017-01-09
中国实用医药(2016年28期)2016-12-07
中外医疗(2016年29期)2016-11-30
中国实用医药(2016年24期)2016-10-17
中国实用医药(2016年13期)2016-07-05
中国实用医药(2016年13期)2016-07-05
中国实用医药(2016年13期)2016-07-05
上海医药(2016年8期)2016-05-30
科技视界(2016年2期)2016-03-30
中国实用医药(2016年3期)2016-01-05