
RET原癌基因突变致多发性内分泌腺瘤病2b型临床诊治
2016-02-23 05:15黄培颖宋海曲王彩虹张惠杰李小英李学军林明珠
中国全科医学 2016年2期
黄培颖,陈 宁,宋海曲,王彩虹,张惠杰,李小英,李学军,林明珠
作者单位:361003福建省厦门市,厦门大学附属第一医院内分泌糖尿病科(黄培颖,陈宁,宋海曲,王彩虹,张惠杰,李学军,林明珠);上海市内分泌代谢病研究所(李小英)
RET原癌基因突变致多发性内分泌腺瘤病2b型临床诊治
黄培颖,陈 宁,宋海曲,王彩虹,张惠杰,李小英,李学军,林明珠
作者单位:361003福建省厦门市,厦门大学附属第一医院内分泌糖尿病科(黄培颖,陈宁,宋海曲,王彩虹,张惠杰,李学军,林明珠);上海市内分泌代谢病研究所(李小英)
【摘要】多发性内分泌腺瘤病(MEN)2b型是RET基因突变引起的常染色体显性遗传病,常见临床表型为甲状腺髓样癌(MTC)、嗜铬细胞瘤、多发性黏膜神经瘤和类马凡体型,各表型可同时或先后发生,易漏诊。本文分析了1例MEN2b型患者病史、诊断、治疗及随访资料。本例患者1995年无诱因出现颈部增粗,诊断为“右甲状腺腺瘤”;1999年发现“左侧甲状腺占位”;2000年发现舌、唇黏膜增厚并突起小肿物,肿物渐增大;2009年及2010年分别行左、右肾上腺肿物切除,术后病理示:嗜铬细胞瘤。本次入院行下唇内侧局部小突起切除和双侧甲状腺次全切除术,术后病理示:舌黏膜神经瘤、MTC。患者基因测序发现RET基因第16号外显子918密码子突变(M918T),患者父母、兄均未出现MEN2b表型特征,基因检测无异常发现。患者MTC术后1年降钙素水平仍高于参考值,结合肺部CT检查结果,考虑MTC肺部转移可能性较大。
1961年,Sipple报道了同时患有甲状腺髓样癌(MTC)、嗜铬细胞瘤和甲状旁腺瘤的病例,后被命名为多发性内分泌腺瘤病2型(MEN2),即Sipple综合征[1]。此后,Williams和Pollock报道了同时患有MTC、嗜铬细胞瘤以及多发性黏膜神经瘤的病例,并于1975年命名为MEN2b型[2]。目前,全世界共报道了约1 000例MEN2家系,其中MEN2b型发病率为2.5/10万[3],但其发病年龄较早,较MEN2a型有更高的侵袭性和病死率。
MEN2b型常见临床表型有MTC、嗜铬细胞瘤、多发性黏膜神经瘤和类马凡体型[4]。此外,部分症状隐匿,若不能及时诊治,预后较差。MEN2b型患者几乎均有MTC,且较一般MTC发病年龄早、侵袭性高。本研究报道了1例经RET基因检测确诊的MEN2b型患者,并总结其临床特点,为临床医生提高该病诊治水平提供参考。
1病例简介
患者,女,30岁,因“颈粗17年,口唇增厚12年,肾上腺术后2年余”于2012-05-10入住本院。患者1995年无诱因出现颈部增粗,无怕热、心悸、多汗,外院诊断为“右甲状腺腺瘤”,行“右侧甲状腺肿物切除”(具体不详),术后未行病理检查,未查甲状腺功能,未随访。1999年彩色多普勒超声检查发现“左侧甲状腺占位4.0 cm×2.9 cm”,未诊治。2001年复查提示“右侧甲状腺多发低回声结节”,结节大小不详,未处理。2000年发现舌、唇黏膜增厚并突起小肿物,肿物渐增大。2007年于外院行“唇黏膜肿物切除”,未行病理检查。2009年前无明显诱因出现发作性心悸、头痛、胸闷、冷汗、面色苍白,每次发作持续10 min,发作时血压最高达160/110 mm Hg(1 mm Hg=0.133 kPa),无不适时血压于90~100/50~60 mm Hg波动。本院CT检查提示“双侧肾上腺占位,左侧9.0 cm×8.0 cm,右侧2.0 cm×2.0 cm,考虑嗜铬细胞瘤”(见图1),行左侧肾上腺肿物切除术,术后病理示:嗜铬细胞瘤,浸润肾上腺皮质。术后血压在130/75 mm Hg上下波动。2010年7月再次行右侧肾上腺肿物切除术,术后病理示:嗜铬细胞瘤。术后糖皮质激素替代治疗,监测血压均正常。多次查甲状腺功能及甲状腺相关抗体均正常。近2年唇黏膜仍出现局部小突起,未重视。1年前于本院查肺部CT提示双肺多发结节,未诊治。1个月前复查肺部CT提示双肺多发结节,较前无明显变化。患者未婚未育。既往月经周期规则。
本次入院查体:血压118/75 mm Hg,体质指数16.4 kg/m2。无明显类马凡体型,四肢细长,消瘦。自主体位,语言清晰。眼睑无水肿,口唇肥厚,舌缘突起多个刺状赘生物(见图2,本文图2~4等彩图见本刊官网www.chinagp.net电子期刊相应文章附件)。颈软,双侧甲状腺表面凹凸不平,左侧甲状腺可触及3.0 cm×3.0 cm包块,质韧,无触痛,无血管杂音。胸廓对称,心肺腹查体无特殊发现,双手细颤阴性,双下肢无水肿,脊柱及四肢关节无畸形。病理反射未引出。取下唇内侧局部小突起活检,并进行RET基因检测。行下唇内侧局部小突起切除,术后病理示:舌黏膜神经瘤(见图3)。因甲状腺肿物,在全身麻醉下行双侧甲状腺次全切除术+中央组淋巴结清扫术+喉返神经探查术,术后病理示:MTC,呈多灶性,累及甲状腺周围淋巴结(见图4);免疫组化:甲状腺转录因子1(+),降钙素(+),突触素(+),Ki-67增殖指数(1%),神经特异性烯醇化酶(+),CD56(+)。术后给予左甲状腺素和氢化可的松替代治疗,未进一步放化疗。患者各时期降钙素、癌胚抗原水平见表1。术后1年复查肺部CT较术前无明显变化。
患者染色体RET原癌基因外显子经PCR测序并亚克隆验证,发现RET基因第16号外显子存在918密码子突变(M918T)。患者父母、兄均未出现MEN2b表型特征,基因检测无异常发现,其家系图见图5。

图1 肾上腺CT检查示双侧肾上腺占位(箭头所示)
Figure 1Bilateral adrenal space occupying shown by adrenal CT examination

图2 患者舌缘突起多个刺状赘生物
2讨论
2.1遗传学MEN2b型是罕见的常染色体显性遗传病,由RET原癌基因突变引起。RET基因位于染色体10q11.2,有21个外显子,编码酪氨酸激酶受体超家族的跨膜蛋白,一旦RET原癌基因密码子发生突变,则活化为显性的具有诱导肿瘤发生的基因,在多种神经内分泌细胞上表达而表现出相应的疾病,如甲状腺C细胞、泌尿生殖系统细胞、肾上腺细胞、副交感神经和交感神经节细胞[5-6]。

注:图A、B见较多增生的神经束呈结节状排列(HE染色,×40);图C、D见肿瘤细胞呈短梭形细波浪状(HE染色,×200)
图3患者下唇内侧局部小突起切除术后病理结果
Figure 3Pathological analysis following the excision of the small protrusions on the inner side of the underlip

图4 甲状腺次全切除术后病理示MTC(HE染色,×40)
Figure 4MTC shown in pathological analysis following the subtotal thyroidectomy

图5 本例MEN2b型患者家系图
Table 1Changes in hormone and tumor marker levels at different time points
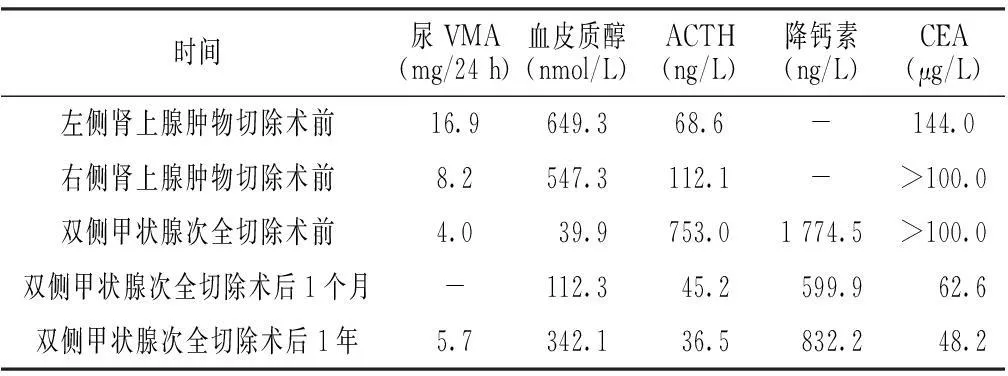
时间尿VMA(mg/24h)血皮质醇(nmol/L)ACTH(ng/L)降钙素(ng/L)CEA(μg/L)左侧肾上腺肿物切除术前16.9649.368.6-144.0右侧肾上腺肿物切除术前8.2547.3112.1->100.0双侧甲状腺次全切除术前4.039.9753.01774.5>100.0双侧甲状腺次全切除术后1个月-112.345.2599.962.6双侧甲状腺次全切除术后1年5.7342.136.5832.248.2
注:VMA=香草扁桃酸,ACTH=促肾上腺皮质激素,CEA=癌胚抗原;-表示无此数据;各指标参考值:VMA 1.4~8.0 mg/24 h,血皮质醇85.3~618.0 nmol/L,ACTH<46.0 ng/L,降钙素0.1~10.0 ng/L,CEA<5.0 μg/L
本例患者出现MTC、双侧肾上腺嗜铬细胞瘤、舌黏膜神经瘤,遗传学分析发现RET原癌基因918密码子突变,根据上述表型和遗传特征,MEN2b型诊断明确。国外对MEN2b型已确定了50种不同的错义突变[7],其中95%的MEN2b型患者和家系为16号外显子918密码子突变[4],本例患者即是该热点突变。MEN2b型在所有MEN2类型中最具侵袭性[8],疾病进展相对较快。由于RET基因是新生突变引发,多数患者无家族史[5],本例患者的家系基因筛查同样未发现存在RET基因突变。
2.2诊断MEN2b型十分罕见,诊断较为困难。只有50%的MEN2b型患者同时出现MTC、黏膜神经瘤、嗜铬细胞瘤的典型表现,在上述表现均出现时再进行诊断为时已晚。本例患者首先发现左叶甲状腺占位,随后逐渐出现舌、唇黏膜肿物,此时即应考虑MEN的可能;后出现血压升高,双侧肾上腺嗜铬细胞瘤,先后行双侧肾上腺肿物切除术,仍未引起临床医生的重视。本院结合其甲状腺肿瘤、双侧肾上腺嗜铬细胞瘤及舌唇黏膜小肿瘤病史,即考虑MEN2b型;进一步进行唇黏膜肿物活检提示黏膜神经瘤,降钙素、癌胚抗原(CEA)水平升高提示甲状腺占位,MTC可能性大,进一步支持MEN2b型。患者RET原癌基因外显子进行PCR直接测序,发现RET基因第16号外显子存在918密码子突变(M918T),最终确诊为MEN2b型。甲状腺肿瘤切除术后病理确诊MTC,术后降钙素及CEA水平即有明显下降。
本例患者双侧甲状腺次全切除术后降钙素及CEA水平虽有下降,但术后1年其水平仍高于参考值。患者存在MTC颈部淋巴结浸润,而淋巴结浸润程度与术后降钙素水平相关。另外,肺是MTC细胞最常见的转移部位[9],降钙素水平>150 ng/L,提示MTC可能已有远处转移,如降钙素水平>1 000 ng/L,则远处转移的风险增大[10]。本例患者双侧甲状腺次全切除术前降钙素水平为1 774.5 ng/L,远处转移可能性极大,故CT提示肺部结节考虑为MTC肺部转移,但患者未再进一步行肺部结节穿刺证实并对肺部病变进一步处理。因此,MTC肺转移可能是降钙素及CEA未能降至参考值的主要原因。
2.3预后在导致MEN2b型的RET基因各种突变类型中,外显子15位密码子883和外显子16位密码子918突变患者易在疾病早期发展为MTC[11],一般预后较差,10年生存率为61%~76%[12]。MTC是MEN2b型患者预后的主要影响因素,MTC病变局限于甲状腺内或仅有少数淋巴结转移,MTC早期是可治愈的[13],超过1年后手术则不能治愈,因此,早期诊断是改善患者预后的关键。笔者建议,出现黏膜神经瘤、嗜铬细胞瘤、甲状腺占位其中2种相关的临床表现均应接受MEN2b型筛查,并将RET原癌基因测序作为常规筛查手段之一,以及早诊断,改善预后。
本例患者甲状腺肿瘤病史达17年,并已确诊MTC,仍无肿瘤晚期衰竭表现。分析患者生存时间较长的原因为:(1)MTC病死率低于其他肿瘤;(2)影响MTC预后的因素有TNM分期、降钙素水平、淋巴结受侵、血管受侵、神经受侵、甲状腺被膜外侵及年龄等[14-15],国内文献报道原发灶直径>4.0 cm、甲状腺被膜外受侵者预后较差[16],本例患者无血管受侵、神经受侵、甲状腺被膜外侵,年龄较小;(3)Ki-67增殖指数与不良预后密切相关[17],Ki-67增殖指数越高,提示处于增殖周期的肿瘤细胞比例越高,肿瘤生长越快,本例患者Ki-67增殖指数仅1%,G0期细胞占多数,可能为其生存时间较长的重要原因。
2.4总结MEN2b型可同时或先后发生多个腺体受累,易漏诊。基因测序是MEN2b型诊断的金标准,早期行RET基因诊断,在出现临床症状时早期行甲状腺切除术可改善预后;同时,RET密码子突变类型决定了不同的表型和MTC侵袭性,因此,RET基因分析可指导甲状腺手术时机。
作者贡献:黄培颖进行资料收集整理、文献检索、撰写论文、成文并对文章负责;陈宁、宋海曲、王彩虹、张惠杰、李小英、李学军进行资料收集;林明珠进行质量控制及审校。
本文无利益冲突。
参考文献
[1]Steiner AL,Goodman AD,Powers SR.Study of a kindred with pheochromocytoma,medunary thyroid carcinoma,hyperparathyroidism,and Cushing′s disease:mutiple endocrine neopIasia,type 2[J].Medicine(Baltimore),1968,47(5):371-409.
[2]Carney JA,Go VL,Sizemore GW,et al.Alimentary-tract ganglioneuromatosis.A major component of the syndrome of multiple endocrine neoplasia,type 2b[J].N Engl J Med,1976,295(23):1287-1291.
[3]Raue F,Frank-Raue K.Multiple endocrine neoplasia type 2:2007 update[J].Horm Res,2007,68(Suppl 5):101-104.
[4]Eng C,Clayton D,Schuffenecker I,et al.The relationship between specific RET proto-oncogene mutations and disease phenotype in multiple endocrine neoplasia type 2.International RET mutation consortium analysis[J].JAMA,1996,276(19):1575-1579.
[5]Kouvaraki MA,Shapiro SE,Perrier ND,et al.RET proto-oncogene:a review and update of genotype-phenotype correlations in hereditary medullary thyroid cancer and associated endocrine tumors[J].Thyroid,2005,15(6):531-544.
[6]Toledo SP,dos Santos MA,Toledo Rde A,et al.Impact of RET proto-oncogene analysis on the clinical management of multiple endocrine neoplasia type 2[J].Clinics(Sao Paulo),2006,61(1):59-70.
[7]Frank-Raue K,Rondot S,Schulze E,et al.Change in the spectrum of RET mutations diagnosed between 1994 and 2006[J].Clin Lab,2007,53(5/6):273-282.
[8]Neumann HP,Eng C,Mulligan LM,et al.Consequences of direct genetic testing for germline mutations in the clinical management of families with multipleendocrine neoplasia,typeⅡ[J].JAMA,1995,274(14):1149-1151.
[9]Dora JM,Canalli MH,Capp C,et al.Normal perioperative serum calcitonin levels in patients with advanced medullary thyroid carcinoma:case report and review of the literature[J].Thyroid,2008,18(8):895-899.
[10]Chen H,Sippel RS,O′Dorisio MS,et al.The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors:pheochromocytoma,paraganglioma,and medullary thyroid cancer[J].Pancreas,2010,39(6):775-783.
[11]Brandi ML,Gagel RF,Angeli A,et al.Guidelines for diagnosis and therapy of MEN type 1 and type 2[J].J Clin Endocrinol Metab,2001,86(12):5658-5671.
[12]Roman S,Lin R,Sosa JA.Prognosis of medullary thyroid carcinoma:demographic,clinical,and pathological predictors of survival in 1252 cases[J].Cancer,2006,107(9):2134-2142.
[13]Machens A,Gimm O,Ukkat J,et al.Improved prediction of calcitonin normalization in medullary thyroid carcinoma patients by quantitative lymph node analysis[J].Cancer,2000,88(8):1909-1915.
[14]Ito Y,Miyauchi A,Yabuta T,et al.Alternative surgical strategies and favorable outcomes in patients with medullary thyroid carcinoma in Japan:experience of a single institution[J].World J Surg,2009,33(1):58-66.
[15]Milan SA,Sosa JA,Roman SA.Current management of medullary thyroid cancer[J].Minerva Chir,2010,65(1):27-37.
[16]Zhang Q,Yang CS,Guo ZM,et al.Prognostic factors of medullary thyroid carcinoma [J].Chinese Journal of Otorhinolaryngology Head and Neck Surgery,2008,43(12):939-942.(in Chinese)
张诠,杨传胜,郭朱明,等.甲状腺髓样癌预后影响因素分析[J].中华耳鼻咽喉头颈外科杂志,2008,43(12):939-942.
[17]Frank-Raue K,Machens A,Leidig-Bruckner G,et al.Prevalence and clinical spectrum of nonsecretory medullary thyroid carcinoma in a series of 839 patients with sporadic medullary thyroid carcinoma[J].Thyroid,2013,23(3):294-300.
(本文编辑:吴立波)
·临床诊疗提示·
【关键词】多发性内分泌腺瘤病2b型;甲状腺肿瘤;嗜铬细胞瘤;RET基因;突变
黄培颖,陈宁,宋海曲,等.RET原癌基因突变致多发性内分泌腺瘤病2b型临床诊治[J].中国全科医学,2016,19(2):229-232.[www.chinagp.net]
Huang PY,Chen N,Song HQ,et al.Diagnosis and therapy of multiple endocrine neoplasia type 2b induced by RET proto-oncogene mutation[J].Chinese General Practice,2016,19(2):229-232.
Diagnosis and Therapy of Multiple Endocrine Neoplasia Type 2b Induced by RET Proto-oncogene MutationHUANGPei-ying,CHENNing,SONGHai-qu,etal.DepartmentofEndocrinologyandDiabetes,theFirstAffiliatedHospitalofXiamenUniversity,Xiamen361003,China
【Abstract】Multiple Endocrine Neoplasia Type 2b (MEN2b)is a autosomal dominant inherited disease induced by RET proto-oncogene mutation.Its common clinical phenotypes include medullary thyroid carcinoma(MTC),pheochromocytoma,multiple mucosal neuromas and body type like marfan syndrome.These phenotypes occur concurrently or successively,which may cause miss diagnosis.In this study,we analyzed the medical history,diagnosis,treatment and follow-up data of a patient with MEN2b.In 1995,neck enlargement occurred in the patient without inducement,and it was diagnosed as "adenoma in the right thyroid".In 1999,"space occupying lesion in the left thyroid" was found in the patient.In 2000,labium mucosa became thick and small mass was found on it with the mass enlarging gradually.The excision of left adrenal masses and the excision of right adrenal masses were conducted in 2009 and 2010 respectively,and the lesion was diagnosed as pheochromocytoma by postoperative pathological analysis.During the hospital visit of the patient when the research was conducted,local small protrusions on the inner side of the underlip were excised,and bilateral subtotal thyroidectomy was also conducted.After these surgeries,the lesions were diagnosed as tongue mucosa neuroma and MTC.By gene sequencing of the patient,we noted the mutation of codon 918 in exon 16 of RET gene.The parents and brothers of the patient showed no phenotypic characteristic of MEN2b and no abnormalities in gene sequencing.One year after MTC surgery,the level of calcitonin was still higher than the reference value,which,combined with the examination results of lung CT scanning,indicated great possibility of lung metastasis from MTC.
【Key words】Multiple endocrine neoplasia type 2b;Thyroid neoplasms;Pheochromocytoma; RET gene;Mutation
收稿日期:(2015-05-18;修回日期:2015-11-25)
【中图分类号】R 736
【文献标识码】B
doi:10.3969/j.issn.1007-9572.2016.02.022
通信作者:林明珠,361003福建省厦门市,厦门大学附属第一医院内分泌糖尿病科;E-mail:linmz65@126.com
猜你喜欢
电子科技大学学报(2022年5期)2022-10-29
中国生殖健康(2020年4期)2021-01-18
生物学通报(2020年11期)2020-10-22
临床肝胆病杂志(2020年9期)2020-09-28
中国微创外科杂志(2019年12期)2019-12-20
中国临床医学影像杂志(2019年5期)2019-08-27
发明与创新·中学生(2019年6期)2019-06-26
中国生殖健康(2018年4期)2018-11-06
中成药(2018年7期)2018-08-04
健康管理(2016年6期)2016-05-14
