
颈椎前路椎间盘切除并自体骨移植钛板固定术对多节段颈椎间盘退行性疾病的疗效分析*
2015-06-05 15:31赵伯明杨述华刘克斌何小斌
华中科技大学学报(医学版) 2015年3期
赵伯明, 杨 操, 杨述华, 刘克斌, 何小斌
颈椎前路椎间盘切除并自体骨移植钛板固定术对多节段颈椎间盘退行性疾病的疗效分析*
赵伯明1,2, 杨 操2△, 杨述华2, 刘克斌1, 何小斌1
1长江大学附属第一医院,荆州第一人民医院骨科,荆州 434000
2华中科技大学同济医学院附属协和医院骨科,武汉 430022
目的 评价颈椎前路椎间盘切除自体髂骨移植钛板固定治疗多节段颈椎间盘退变病的临床和影像学效果。方法 28例患者接受了颈椎前路椎间盘切除自体骨移植钛板固定手术。临床结果评估采用日本矫形外科协会(JOA)评分和Odom标准,并对融合率、颈椎曲度和手术并发症进行了评估。结果 28例均获随访,平均24个月(9~36个月)JOA评分,术前(7.54±0.78),术后3d(10.82±0.93),术后6个月(14.14±0.74),终访时(13.86±1.22),术后各时点与术前相比差异均有统计学意义(均P<0.05)。颈椎影像资料显示牢固融合25例(89.3%),平均融合时间5.9个月。颈椎曲率为术前(14.96±1.90)°,术后3d(26.89±3.78)°,术后6个月(25.86±3.67)°,终访时(24.89±3.69)°,术后各时点与术前相比差异均有统计学意义(均P<0.05)。结论 在多节段颈椎退变病中应用颈椎间盘切除自体骨融合钛板固定术取得了有效减压和稳定脊柱等良好的临床和影像学效果。
颈椎间盘退行性疾病; 多节段颈椎间盘切除融合; 自体骨; 动态钛板
颈椎间盘退行性变是颈椎病最常见的原因,它通过腹侧压迫脊髓或神经根,可能会导致神经功能障碍,颈部疼痛或复合症状。通常需要通过手术进行神经减压,恢复和稳定脊柱前凸。当骨赘或椎间盘突出在腹侧、脊柱后凸,前路减压术不仅可以直接减压,而且有助于利用术中撑开技术恢复颈椎力线。
目前,颈椎前路椎间盘切除术和自体或异体骨植骨融合已成为手术治疗颈椎病的金标准。在多节段手术过程中,一些术者认为需要采用内固定器械如颈椎钢板系统[1],已有报道称器械内固定的自体或同种异体骨移植融合率较非器械内固定高[2]。而同种异体移植骨又较自体骨移植融合率低且成本更高[3]。因此,本文将讨论颈椎前路减压自体髂骨植骨融合和动力钛板固定在多节段颈椎退变病中的应用。
1 资料与方法
1.1 一般情况
病例资料来自2010年7月至2012年6月武汉协和医院骨科收治的2个或3节段颈椎退变病并实施了颈椎前路椎间盘切除并自体骨移植钛板固定术的28例患者。所有患者均签署手术知情同意书,研究经华中科技大学医学伦理委员会批准。入选标准:①有脊髓或神经根症状,保守治疗无效;②磁共振显示明显的颈脊髓压迫;③行颈椎前路椎间盘切除自体骨移植钛板固定术。排除标准:①连续或复合的后纵韧带骨化症;②上颈椎手术;③急性椎间盘突出;④重大创伤,感染或肿瘤。28例患者中有19例男性,9例女性;年龄42~64岁(平均55.0岁)。13例神经根型,6例脊髓型,9例脊髓神经根型。手术节段从C4-5至C6-7。脊髓压迫节段由磁共振成像(MRI)确定。18例患者行2节段颈椎前路椎间盘切除并自体骨移植钛板固定术,10例行3节段手术。
1.2 外科手术
所有的手术在患者仰卧位全身麻醉下进行,由同一名脊柱外科医生(杨操)操作,采用相应颈椎节段右侧颈前方入路。椎间盘切除、后纵韧带切开、椎管和椎间孔骨赘切除过程均采用头戴式显微镜辅助完成。切除完成后,扩大牵开并测量椎间隙高度至少5mm。刮除椎骨终板,适当大小皮髓质髂骨移植。最后依据颈椎前凸曲线置入ABC(Aesculap,Tuttlingen,德国)动态骨板自锁螺钉系统。术中透视确保移植骨和钛板位置正确。
1.3 疗效评价
1.3.1 临床评价 于术前、术后3d、术后3个月及最终随访时间,采用日本骨科协会(JOA)评分和Odom标准[4]进行临床评估。根据JOA评分计算恢复率(RR):(术后评分-术前评分)/(17-术前评分)×100%,分别以≥75%、~50%、~25%、<25%为优、良、中、差。评估由没有参与任何治疗过程的3名骨科医生完成。
1.3.2 影像学评价 于术前、术后3d、3个月、6个月拍摄颈椎X线片,6个月后为每6个月拍1次。影像学融合标准[5]:①终板消失无透亮线;②在移植和终板交界处存在连续骨梁;③屈伸侧位片棘突间位移不超过2mm。颈椎曲度评估是在侧位X线片采用Harrison’s测量[6]:正值切线角表示前凸,负值表示后凸。评估由没有参与任何治疗过程的3名骨科医生完成。
1.3.3 并发症 并发症包括:患者出现暂时的或永久性的疼痛,神经系统症状或体征的持续恶化,软组织损伤,手术部位的感染,二次手术等。
1.4 统计学分析
JOA评分和颈椎曲度结果以均数±标准差表示,数据分析采用SPSS 15.0统计分析软件行Student’s t检验,以P<0.05为差异有统计学意义。
2 结果
2.1 一般情况
平均手术时间为144min(110~190min)与平均出血量为155mL(90~230mL)。所有移植物均植入成功。无患者穿戴颈椎外固定器。随访时间9~36个月,平均24个月。
2.2 临床评估结果
由表1可见,28例患者术后各检测时点的JOA评分均高于术前,差异均有统计学意义(均P<0.05)。28例患者恢复率情况:优10例,良15例,中3例,差0例。根据Odom标准,9例患者疗效优,16例良,3例中,差0例。近90%的患者对结果满意。
2.3 影像学评估结果
颈椎影像资料显示牢固融合25例(89.3%),平均融合时间5.9个月。1例3节段手术患者延迟融合,手术13个月后达到融合。有2例3节段手术患者1个间隙不融合,1例2节段手术患者1个间隙不融合,但患者没有临床症状。
由表1可见,28例患者术后各检测时点的颈椎曲率均较术前明显增大,差异有统计学意义(均P<0.05)。术前和术后颈椎曲度变化如图1、2所示。

表1 不同时间点JOA评分和Harrison’s角(¯x±s)Table1 JOA scores and Harrison’s angles at different time points(¯x±s)

图1 1例2节段颈椎退变病患者术前及术后影像学检查Fig.1 Preoperative and postoperative images in a case of two-level CDDD
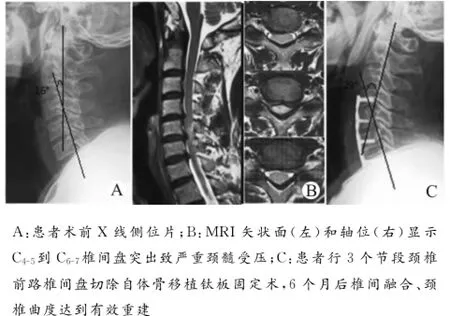
图2 1例3节段颈椎退变病患者术前及术后影像学检查Fig.2 Preoperative and postoperative images in a case of threelevel CDDD
2.4 并发症
本组无死亡病例,没有严重的全身麻醉相关并发症。2例患者有短暂的其他节段的神经根症状。1例患者因引流管堵塞致皮下血肿并于术后3d消除。3例感觉轻度吞咽不适但术后2周消失。3例咬骨钳致硬膜穿孔但没有导致脑脊液瘘或相关神经功能缺损。长期随访未发现其他术后并发症如神经症状加重、移植物松动、伤口感染和呼吸功能不全等。
3 讨论
颈椎退变病包括骨关节病理性椎间盘退变、椎间盘突出后残余纤维环移出及骨赘形成。椎间盘间隙连续塌陷后,黄韧带继而冗余、内凸压迫脊髓表面[7]。由于保守治疗通常无效,常需要手术进行神经减压,恢复和稳定脊柱前凸[8]。
颈椎前路椎间盘切除自体髂骨融合技术对颈椎间盘退变病患者是不错的选择。近十年来,多种类型椎间融合器如PEEK、碳纤维和钛笼逐步问世使得该技术有了较大的发展[9-11]。虽然填充同种异体松质骨的融合器在单节段颈椎手术中获得了较高的融合率和良好的临床效果[4],但在多节段手术中其融合率要低得多,并影响到临床结果如形成假关节和增加再手术率[12-13]。Shapiro等[14]报道在多节段颈椎手术中融合器沉降率、椎间隙塌陷、后凸畸形发生率高达36%。Kaise等[5]的研究显示多阶段颈椎术后需佩戴颈椎外固定器6~12周,该刚性颈领可能会影响患者的生活质量和日常活动。应用自体或异体骨填充椎间融合器的患者中,其症状改善率为65%~92%[15-17]。Dumont等[1819]报道临床症状恶化如复发、假关节的概率为8.1%,假关节、假体下沉、进展性后凸均可降低椎间孔的大小和颈椎稳定性,最终导致神经脊髓受压和内置物失败,约三分之一的复发或出现新症状的患者需再次手术。然而,最近报道的颈椎前路椎间盘切除自体骨移植钛板固定术,患者因这类并发症致再手术的发生率非常低,且不必使用刚性颈椎矫形器,减少了术后恢复时
间[20]。
我们对28例颈椎退变病患者进行了颈椎前路减压自体髂骨融合动态钛板固定术。选择该术式的主要原因:①自体骨具有良好的生物相容性,结构支撑,成骨性能好,无传播疾病的风险,无免疫原性,成本更低,尽管收获自体供骨可能引起患者的不适[2122]。②自体三面皮质髂骨可依据颈椎解剖曲线在冠状面和矢状面上塑形。③动态钛板固定系统与骨承重界面相容性好,该界面传递包括头部重量的轴向载荷和颈部肌肉的力量负荷[23]。随着时间的推移,即使是移植骨在骨重建过程中部分吸收了,该骨板系统也能维持这些负荷,从而促进移植骨重建,因此达到较高的融合率[24-25]。我们应用ABC(Aesculap,Tuttlingen,德国)动态钛板自锁螺钉系统不仅达到即时生物力学稳定,还防止了植骨骨折脱位。
我们依据JOA和Odom’s标准对手术结果进行评估,优良率达到90%,椎间高度和脊柱的生理曲度得到一定的恢复与维持,在所有66个手术节段中融合失败率占4.5%,无严重并发症。通过对本组病例的总结分析,我们的经验是:前路能直接达到病变部位,尤其是颈椎前凸不足或反弓的颈椎退变病的患者,多节段颈椎间盘切除自体髂骨融合骨板固定可以恢复脊柱前凸和充分解除后路手术通常不能去除的脊髓致压物;与椎体次全切的长段腓骨移植相比,多节段椎间植骨能更有效恢复椎间高度。当然,也有学者持有不同的观点。Hussain等[26]认为,前路多节段去除椎体后骨赘技术要求高,脊髓损伤风险大。Robinson等[27]认为,当骨重建融合后原有骨刺会被吸收,因此没必要冒险去除骨赘。我们认为,需要权衡椎体后方骨赘切除的困难与耗时给患者带来的利弊。本组病例去除骨赘没有损伤硬脊膜,并通过ABC动态钛板固定系统实现颈椎病变部位的即刻稳定,术后恢复顺利。
综上所述,多节段颈椎间盘切除自体髂骨融合钛板固定是一种合理安全的手术方法,应用恰当并细致操作能达到减压目的,同时椎间自体植骨技术可恢复维持脊柱前凸,提高融合率,术后通常不需要矫形器外固定。尽管我们的初步结果令人鼓舞,但也存在某些不足,如未能对颈椎多节段融合后邻近节段退变问题进行评估。所以,我们仍需进行大样本长期随访研究,进一步评估颈椎前路椎间盘切除自体骨移植钛板固定术在多节段颈椎间盘退变病中的治疗效果。
[1] Fernández-Fairen M,Murcia A,Torres A,et al.Is anterior cervical fusion with a porous tantalum implant a cost-effective method to treat cervical disc disease with radiculopathy?[J].Spine,2012,37(20):1734-1741.
[2] Kaiser M G,Haid R W J,Subach B R,et al.Anterior cervical plating enhances arthrodesis after discectomy and fusion with cortical allograft[J].Neurosurg,2002,50(2):229-238.
[3] Epstein N E.Iliac crest autograft versus alternative constructs for anterior cervical spine surgery:Pros,cons,and costs[J].Surg Neurol Int,2012,3(3):S143-S156.
[4] Odom G L,Finney W,Woodhall B.Cervical disk lesions[J].JAMA,1958,166(1):23-28.
[5] Kaiser M G,Mummaneni P V,Matz P G,et al.Radiographic assessment of cervical subaxial fusion[J].J Neurosurg Spine,2009,11(2):221-227.
[6] Harrison D E,Harrison D D,Cailliet R,et al.Cobb’s method orHarrison posterior tangent method:wihich is better for lateral cervical analysis[J].Spine,2000,25(16):2072-2078.
[7] Uchida K,Nakajima H,Sato R,et al.Cervical spondylotic myelopathy associated with kyphosis or sagittal sigmoid alignment:outcome after anterior or posterior decompression[J].J Neurosurg Spine,2009,11(5):521-528.
[8] Yang S,Hu Y,Zhao J,et al.Follow-up study on the motion range after treatment of degenerative disc disease with the Bryan cervical disc prosthesis[J].J Huazhong Univ Sci Technolog[Med Sci],2007,27(2):176-178.
[9] Kulkarni A G,Hwan T,Hee K,et al.Solis cage(PEEK)for anterior cervical fusion:preliminary radiological results with emphasis on fusion and subsidence[J].Spine J,2007,7(2): 205-209.
[10] Hermansen A,Hedlund R,Vavruch L,et al.A comparison between the carbon fiber cage and the cloward procedure in cervical spine surgery:a ten-to thirteen-year follow-up of a prospective randomized study[J].Spine,2011,36(12):919-925.
[11] Waschke A,Kaczor S,Walter J,et al.Expandable titanium cages for anterior column cervical reconstruction and their effect on sagittal profile:a review of 48cases[J].Acta Neurochir,2013,155(5):801-807.
[12] Saarinen T,NiemeläM,Kivisaari R,et al.Early and late reoperations after anterior cervical decompression and fusion during an 11-year follow-up[J].Acta Neurochir,2013,155(2):285-291
[13] Frenkel M B,Cahill K S,Javahary R J,et al.Fusion rates in multilevel,instrumented anterior cervical fusion for degenerative disease with and without the use of bone morphogenetic protein[J].J Neurosurg Spine,2013,18(3):269-273.
[14] Shapiro S,Connolly P,Donnaldson J,et al.Cadaveric fibula,locking plate,and allogeneic bone matrix for anterior cervical fusions after cervical discectomy for radiculopathy or myelopathy[J].J Neurosurg,2001,95(Suppl 1):43-50.
[15] Shamji M F,Massicotte E M,Traynelis V C,et al.Comparison of anterior surgical options for the treatment of multilevel cervical spondylotic myelopathy:a systematic review[J].Spine,2013,38(22):195-209.
[16] Fehlings M G,Smith J S,Kopjar B,et al.Perioperative and delayed complications associated with the surgical treatment of cervical spondylotic myelopathy based on 302patients from the AOSpine North America Cervical Spondylotic Myelopathy Study[J].J Neurosurg Spine,2012,16(5):425-432.
[17] Ghogawala Z.Commentary:Patient heterogeneity complicates efforts to compare effectiveness for anterior versus posterior surgery for cervical spondylotic myelopathy[J].Spine J,2013,13(7):732-733.
[18] Dumont T M,Lin C T,Tranmer B I,et al.Pseudarthrosis failures of anterior subaxial cervical spine fusion using aplate with a single screw per vertebral body:a case series[J].World Neurosurg,2014,82(1):225-230.
[19] Park J I,Cho D C,Kim K T,et al.Anterior cervical discectomy and fusion using a stand-alone polyetheretherketone cage packed with local autobone:assessment of bone fusion and subsidence[J].J Korean Neurosurg Soc,2013,54(3):189-193.
[20] Kotil K,Tari R.Two level cervical corpectomy with iliac crest fusion and rigid plate fixation:a retrospective study with a three-year follow-up[J].Turk Neurosurg,2011,21(4):606-612.
[21] Silber J S,Anderson D G,Daffner S D,et al.Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion[J].Spine,2003,28(2):134-139.
[22] Heary R F,Schlenk R P,Sacchieri T A,et al.Persistent iliac crest donor site pain:independent outcome assessment[J].Neurosurg,2002,50(3):510-517.
[23] Brodke D S,Gollogly S,Alexander Mohr R,et al.Dynamic cervical plates:biomechanical evaluation of load sharing and stiffness[J].Spine,2001,26(12):1324-1329.
[24] Balabhadra R S,Kim D H,Zhang H Y.Anterior cervical fusion using dense cancellous allografts and dynamic plating[J].Neurosurgery,2004,54(6):1405-1411.
[25] Connor D E Jr,Shamieh K S,Ogden A L,et al.Biomechanical performance of rigid compared to dynamic anterior cervical plating:analysis of adjacent upper and lower level compressive forces[J].J Clin Neurosci,2012,19(12):1706-1710.
[26] Hussain M,Nassr A,Natarajan R N,et al.Biomechanical effects of anterior,posterior,and combined anterior-posterior instrumentation techniques on the stability of a multilevel cervical corpectomy construct:a finite element model analysis[J].Spine J,2011,11(4):324-330.
[27] Robinson R A.Anterior and posterior cervical spine fusions[J].Clin Orthop Relat Res,1999,2(359):4-17.
(2015-01-12 收稿)
Anterior Cervical Discectomy and Fusion with Autograft and Titanium Plate for the Treatment of Multi-Level Cervical Disc Degenerative Disease
Zhao Boming1,2,Yang Cao2△,Yang Shuhua2et al
1Department of Orthopaedics,Jingzhou First People’s Hospital,Jingzhou 434000,China
2Department of Orthopaedics,Union Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan 430022,China
Objective To evaluate the clinical and radiological outcomes of anterior cervical discectomy and fusion with autograft and titanium plate(ACDFP)for the treatment of multi-level cervical disc degenerative disease(CDDD).Methods Twenty-eight consecutive patients with multi-level CDDD underwent ACDFP.Clinical outcomes were evaluated by using Japanese Orthopaedic Association(JOA)scores and Odom’s criteria.The fusion rate and spinal curvature at the operated levels and surgical complications were assessed.Results All the 28patients were followed up for an average of 24months(range:9-36 months).The JOA score was(7.54±0.78),(10.82±0.93),(14.14±0.74)and(13.86±1.22),respectively,before surgery,3days and 6months after surgery,and at thefinal follow-up.Radiographs of the cervical spine revealed that the solid fusion was obtained in 25cases(89.3%)at a mean time of 5.9months.The cervical spinal curvature was(14.96±1.90)°before operation,(26.89±3.78)°at 3days after operation,(25.86±3.67)°at 6months after operation,and(24.89±3.69)°at the final follow-up.There were significant differences in the JOA score and cervical spinal curvature between before and at various time points after operation.Conclusion Treatment of multi-level CDDD by ACDFP can effectively decompress and stabilize the spine,yielding satisfactory clinical and radiological outcomes.
cervical degenerative disc disease; multi-level cervical discectomy and fusion; autograft; dynamic titanium plate
R681.531
10.3870/j.issn.1672-0741.2015.03.019
*国家自然科学基金资助项目(No.81072187)
赵伯明,男,1980年生,主治医师,E-mail:zbm1999521@163.com
△通讯作者,Corresponding author,E-mail:yangcaomd@163.com
猜你喜欢
中学生博览·文艺憩(2020年3期)2020-08-14
灾害医学与救援(电子版)(2017年3期)2017-02-06
罕少疾病杂志(2016年1期)2017-01-11
中华骨与关节外科杂志(2016年6期)2016-05-17
中华手工(2016年2期)2016-03-08
西南军医(2016年3期)2016-01-23
中国继续医学教育(2015年3期)2016-01-06
中国医疗美容(2015年1期)2015-07-12
中国美容整形外科杂志(2014年3期)2014-01-21
中国中西医结合外科杂志(2013年3期)2013-03-11
