
早期液体复苏对重症急性胰腺炎患者疗效的影响
2011-11-22 01:28:12钟鸣陈尔真
中华胰腺病杂志 2011年6期
钟鸣 陈尔真
·论著·
早期液体复苏对重症急性胰腺炎患者疗效的影响
钟鸣 陈尔真
目的探讨早期液体复苏对重症急性胰腺炎(SAP)患者治疗效果的影响。方法将发病72 h内就诊的70例SAP患者纳入研究。液体复苏达标参数:心率<120次/min;尿量≥1 ml·h-1·kg-1;血细胞比容≤35%;平均动脉压65~85 mmHg(1 mmHg=0.133 kPa)。回顾分析液体复苏达标时间(<48 h、48~72 h、>72 h)和达标项目数(0~1、2、3、4项)对患者疗效的影响。结果70例患者中41例(58.6%)发生并发症,20例(28.6%)中转手术,10例(14.3%)病死。中位住院天数为23.5 d,中位治疗费用为7.19(0.57~56.74)万元。<48 h、48~72 h、>72 h液体复苏达标患者的中转手术率(20.0%、33.3%、75.0%)、急性肾损伤发生率(20.0%、25.0%、75.0%)和并发症发生率(50.0%、83.3%、100%)在3组间均有统计学意义(P<0.05)。发病48 h内液体复苏后0~1、2、3、4项达标者的中转手术率(50.0%、26.3%、13.0%、25.0%)、急性肾损伤发生率(45.0%、31.6%、17.4%、0)、ARDS发生率(35.0%、31.6%、13.0%、0)均呈显著下降趋势。结论SAP发病48 h内,合理的液体复苏策略有利于提高疗效,改善患者预后。
胰腺炎,急性坏死性; 回顾性研究; 液体复苏
急性胰腺炎(AP)是临床常见急腹症,其中重症急性胰腺炎(SAP)患者约占28%[1],其病死率为10%~25%[2]。早期规范化治疗对进一步提高SAP总体疗效具有重要的意义。但对其具体实施方案,包括具体输液量、输液目标和输液种类等至今尚缺乏一致的结论。本研究回顾分析我院近两年来收治的SAP患者临床资料,旨在探讨SAP早期液体复苏治疗策略对预后的影响。
资料与方法
一、研究对象
选择2008年1月至2009年12月发病72 h内入院且临床资料齐全的SAP患者为研究分析对象,年龄在18~70岁之间。SAP诊断符合中华医学会外科学分会制定的标准[3]。排除标准:有慢性基础心脏病、安装心脏起搏器、慢性肾功能衰竭的患者。
二、资料收集
1.患者一般资料:患者性别、年龄、发病时间、病因、入院时APACHEⅡ评分、CT严重指数(CTSI)和Ranson评分值。记录入院后72 h内患者晨6∶00的心率、血压、24 h尿量、血细胞比容及每24 h接受的液体输入量。在液体复苏治疗中,患者满足以下4项指标中的任意两项或两项以上即认为液体复苏达标[4]:(1)平均动脉压维持在 65~85 mmHg(1 mmHg=0.133 kPa);(2)尿量≥ 1 ml·h-1·kg-1;(3)血细胞比容≤35%;(4)心率<120 次/min。
2.并发症:急性呼吸窘迫综合征(ARDS)、急性肾损伤、腹腔感染、腹腔高压综合征(abdominal compartment syndrome, ACS)、假性囊肿、弥漫性血管内凝血(DIC)等。ARDS诊断标准采用1994年欧美ARDS会议的共识标准[5],急性肾损伤定义为RIFLE评分达到或超过R级[6]。
3.患者存活率、中转手术率、住院天数及治疗费用。
三、统计学处理

结 果
一、一般情况
70例SAP患者符合要求而纳入,其中男50例,女20例,平均年龄(54±18)岁。入院时患者APACHEⅡ评分中位数为8(1~18)分,Ranson评分中位数为2(0~5)分,CTSI中位数为4(1~6)分。
病因:胆源性40例(57.1%),高脂血症性12例(17.1%),特发性15例(21.4%),酒精性3例(4.3%)。
并发症总发生率为58.6%(41/70)。发生各种并发症66例次,其中腹腔感染16例次(24.2%),ARDS 16例次(24.2%),急性肾损伤19例次(28.8%),ACS 1例次(1.5%),腹腔出血2例次(3.0%),肺部感染2例次(3.0%),假性囊肿5例次(7.6%),血液感染2例次(3.0%),DIC 3例次(4.6%)。发生1种并发症患者23例(32.9%)、2种12例(17.1%)、3种5例(7.1%)、4种1例(1.4%)。病死10例(14.3%),中转手术20例(28.6%),总体中位住院天数为23.5(3.6~157)d,总体中位治疗费用为7.19(0.57~56.74)万元。
二、液体复苏达标时间对患者的影响
根据复苏达标时间,将患者分为<48 h、48~72 h、>72 h达标组。三组间的病死率及ARDS发生率无显著差异。但随着液体复苏达标时间的延后,中转手术率、急性肾损伤发生率和并发症发生率呈增高趋势(表1)。
三、48 h内液体复苏达标程度对预后的影响
48 h内液体复苏达标的项数与患者的APACHEⅡ评分、CTSI、Ranson评分、平均输液量、总体并发症发生率、患者病死率均无相关性,但随着48 h内液体复苏达标项数的增加,中转手术率、ARDS和急性肾损伤发生率显著下降(表2)。

表1 液体复苏不同达标时段患者各指标比较[(例,率(%)]
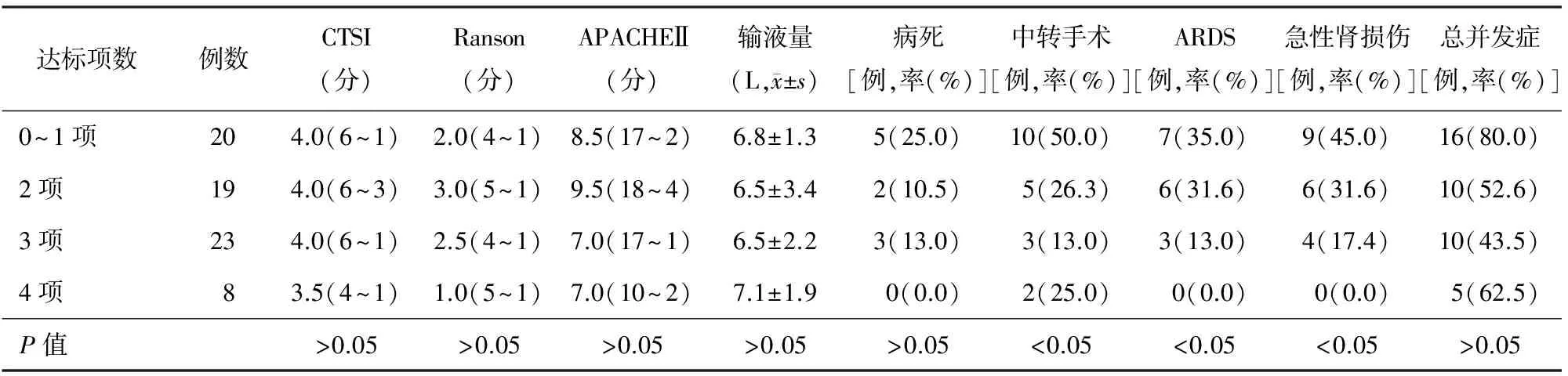
表2 48 h内不同液体复苏达标程度患者各项指标的发生例数
讨 论
关于SAP时液体复苏的目标至今仍处于争论之中。Muddana等[7]认为,须维持尿量在0.5~1 ml·h-1·kg-1,并在第一个24 h内使血细胞比容下降。毛恩强等[4]提出的SAP早期液体复苏达标的参数主要包括心率<120次/min、血细胞比容≤35%、尿量>1 ml·h-1·kg-1和平均动脉压维持在65~85 mmHg,满足以上两项或两项以上即表示液体复苏达标。其中,心率<120次/min及平均动脉压恢复表明血容量开始回复;尿量>1 ml·h-1·kg-1表示肾脏灌注基本正常;血细胞比容≤35%表示输液量克服毛细血管渗漏引起的血液浓缩。但临床上仍有不少患者出现各种并发症、需要手术治疗并带来较高的治疗成本,故有必要对这些标准及SAP患者的液体复苏情况进一步分析,以期有所启发。
本结果显示,48 h内达到液体复苏标准的患者预后较好。随着达标时间的推移,患者中转手术率、总体并发症发生率和急性肾损伤发生率呈显著增高的趋势,ARDS的发生率、中转手术率及病死率亦有增高趋势,提示及时的液体复苏有助于改善患者预后。Rivers等[8]亦提出液体复苏的时机宜在6 h以内。但毛恩强等[4]报道, 24 h内达标的SAP患者治愈率显著低于48 h和72 h达标者,而48 h内达标患者的治愈率较72 h内达标者为高,认为适当延迟的液体复苏可能更有助于改善患者预后。
本结果还提示,在发病48 h内液体复苏达标项目数越多,急性肾损伤及ARDS发生率越低,病死率也较低。但液体复苏4项指标均达标或均未达标患者较部分达标患者的48 h总输液量及总体并发症发生率较高,提示对SAP患者单纯的以输液量来指导液体复苏可能并不合适。Eckerwall等[9]曾报道,24 h输液量>4 L的SAP患者其呼吸系统并发症发生率较<4 L者高。Bagshaw等[10]亦指出,液体正平衡的患者预后较液体负平衡者预后差,故提倡对SAP患者早期限制性液体复苏。Wu[11]提出了对SAP进行针对性的液体复苏策略,但最近的多中心研究尚未给出确切的答案。
由于本研究为回顾性研究,临床资料受许多因素影响,且样本量相对较少。另一方面,达标参数本身亦受到诸多因素的影响。如胰腺炎引起的全身炎症反应综合征(SIRS)最常见的表现为心率增快,故心率作为液体复苏达标参数的特异性较差;病理情况下正常的血压值并不能排除微循环中的灌注不足;尿量则可能受到使用利尿剂的影响而并不能反映肾脏的实际灌注情况;血细胞比容在SAP中对预后的意义也颇有争议[12-13]。此外,本研究未区分胶体液及晶体液对复苏效果的影响。因此,对于以上液体复苏参数很有必要进行前瞻性的研究加以证明,同时临床上还需要进一步寻找更合适和准确的参数指导液体复苏治疗。
[1] 急性胰腺炎协作组. 中国6223例急性胰腺炎病因及病死率分析.胰腺病学, 2006, 6: 321-325.
[2] Tonsi AF, Bacchion M, Crippa S, et al. Acute pancreatitis at the beginning of the 21st century: The state of the art. World J Gastroenterol, 2009, 15: 2945-2959.
[3] 中华医学会外科学分会胰腺外科学组. 重症急性胰腺炎诊治指南. 中华外科学杂志, 2007, 45: 727-729.
[4] 毛恩强,汤耀卿,李磊,等.重症胰腺炎急性反应期控制性液体复苏策略.中华外科杂志,2007, 45: 1331-1334.
[5] Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome.The Acute Respiratory Distress Syndrome Network. N Engl J Med,2000,342:1301-1308
[6] Hoste EA, Clermont G, Kersten A, et al. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis.Crit Care, 2006, 10: R73-R83.
[7] Muddana V, Whitcomb DC, Papachristou GI. Current management and novel insights in acute pancreatitis.Expert Rev Gastroenterol Hepatol, 2009, 3:435-444.
[8] Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med, 2001, 345:1368-1377.
[9] Eckerwall G, Olin H, Andersson B, et al. Fluid resuscitation and nutritional support during severe acute pancreatitis in the past: what have we learned and how can we do better?Clin Nutr, 2006, 25:497-504.
[10] Bagshaw SM, Brophy PD, Cruz D, et al. Fluid balance as a biomarker: impact of fluid overload on outcome in critically ill patients with acute kidney injury.Crit Care,2008,12:169.
[11] Wu BU, Hwang JQ, Gardner TH, et al. Lactated Ringer′s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol,2001,9:710-717.
[12] Brown A, Orav J, Banks PA. Hemoconcentration is an early marker for organ failure and necrotizing pancreatitis.Pancreas, 2000, 20: 367-372.
[13] Lankisch PG, Mahlke R, Blum T, et al. Hemoconcentration: an early marker of severe and/or necrotizing pancreatitis? A critical appraisal. Am J Gastroenterol, 2001, 96: 2081-2085.
2011-03-02)
(本文编辑:屠振兴)
Effectofearlyfluidresuscitationontheprognosisofsevereacutepancreatitis
ZHONGMing,CHENEr-zhen.
DepartmentofEmergencyIntensiveCareUnit,RuijinHospital,SchoolofMedicine,ShanghaiJiaotongUniversity,Shanghai200025,China
CHENEr-zhen,Email:chenerzhen@hotmail.com
ObjectiveTo investigate the effect of early fluid resuscitation on the prognosis of SAP patients.MethodsPatients who were admitted to our hospital within 72 h after the onset of the SAP were enrolled. The parameters for the fluid resuscitation were as follow: heart rate <120 beat/h, urine output ≥ 1 ml·h-1·kg-1, hematocrit ≤35% and mean arterial pressure 65~85 mmHg (1 mmHg=0.133 kPa). The effects of different time of reaching fluid resuscitation (<48 h, 48-72 h, >72 h) and parameters achieved (0~1 parameter, 2 parameters, 3 parameters, 4 parameters) on the prognosis were analyzed.ResultsThere were 70 patient enrolled in this study and 41(58.6%) developed complications, 20(28.6%) were referred to surgical operation and 10(14.3%) died. The median hospital stay was 23.5 d, and the median medical cost was 71.9(5.7~567.4 thousands RMB). The rates of surgical intervention in <48 h, 48~72 h, >72 h groups were 20.0%, 33.3%, 75.0%, and the rates of acute kidney injury were 20.0%, 25.0%, 75.0%, while the rates of complications were 50.0%, 83.3%, 100%, and the difference among the 3 groups was statistically significant (P<0.05). The rates of surgical intervention in patients achieving 0~1, 2, 3, 4 parameters within 48h of SAP onset were 50.0%, 26.3%, 13.0%, 25.0%, and the rates of acute kidney injury were 45.0%, 31.6%, 17.4%, 0, while the rates of ARDS were 35.0%, 31.6%, 13.0%, 0, which showing a significant decreasing trend.ConclusionsAn appropriate fluid resuscitation in the first 48 h after the onset of SAP was benefit for improving the treatment effects and patients′ outcome.
Pancreatitis, acute necrotizing; Retrospective studies; Fluid resuscitation
10.3760/cma.j.issn.1674-1935.2011.06.002
山东省医药卫生科技发展计划(2009HW001)
200025 上海,上海交通大学医学院附属瑞金医院急诊ICU
陈尔真,Email:chenerzhen@hotmail.com
猜你喜欢
河南科学(2020年3期)2020-06-02 08:30:16
保健与生活(2019年14期)2019-08-21 01:12:17
云南医药(2019年3期)2019-07-25 07:25:16
长春中医药大学学报(2019年3期)2019-02-15 19:45:35
铜仁学院学报(2018年6期)2018-07-05 09:47:36
心血管病学进展(2018年1期)2018-02-12 12:31:41
中国继续医学教育(2015年3期)2016-01-06 01:36:46
中国保健营养·上旬刊(2014年5期)2014-05-30 21:59:38
火工品(2013年3期)2013-10-11 07:46:04
肾脏病与透析肾移植杂志(2013年1期)2013-04-07 12:59:14
