艾司氯胺酮对胸腔镜肺癌根治术后恢复质量及炎症应激反应的影响*
2024-12-04 00:00:00陈丽丽魏磊张卓亮鲁刚潘建华
南通大学学报(医学版) 2024年3期

[摘" "要]" "目的:观察艾司氯胺酮对胸腔镜肺癌根治患者术后恢复质量及炎症应激的影响。方法:选择2022年9月—2023年5月于南京医科大学附属苏州医院行胸腔镜下肺癌根治术患者60例,采用随机数字表法分为艾司氯胺酮组(S组)和对照组(C组),各30例。两组麻醉诱导方案相同,S组麻醉诱导后予艾司氯胺酮0.25 mg/kg以0.15 mg/(kg·h)持续静脉泵注至缝皮。C组麻醉诱导后和术中予同等剂量生理盐水。记录两组患者麻醉时间、手术时间、拔管时间、术后恢复室(postanesthesia care unit, PACU)停留时间,阿片类药物消耗量与术后48 h内镇痛泵按压次数,术前24 h(T0)、术后24 h(T1)、术后48 h(T2)各时间点的40项恢复质量量表(40-item Quality of Recovery Questionnaire, QoR-40)评分,ELISA检测T0、T2时的TNF-α、IL-6的表达水平,记录两组患者24 h内谵妄、恶心呕吐、噩梦、头晕等并发症的发生情况。结果:两组患者手术时间、拔管时间、PACU停留时间比较差异均无统计学意义(均P>0.05)。与C组比较,S组患者术中瑞芬太尼消耗量显著降低(Plt;0.05),术后舒芬太尼消耗量显著下降(Plt;0.05),术后48 h内镇痛泵按压次数明显减少(Plt;0.05)。两组患者术前总QoR-40评分及各项维度评分比较差异均无统计学意义(均Pgt;0.05);与T0时相比,两组患者T1、T2时总QoR-40评分以及各项维度评分均明显下降(均Plt;0.05);与C组比较,T1时S组总QoR-40评分、身体舒适度、心理支持和疼痛感受评分显著升高(Plt;0.05),T2时S组总QoR-40评分、身体舒适度和疼痛感受评分高于C组(Plt;0.05)。T0时,两组患者的血清TNF-α和IL-6水平比较差异无统计学意义(Pgt;0.05)。T2时,两组患者血清IL-6和TNF-α水平均显著升高(均Plt;0.05),S组均低于C组(均Plt;0.05)。两组患者术后不良反应发生率比较差异无统计学意义(Pgt;0.05)。结论:艾司氯胺酮可以提高胸腔镜肺癌根治患者术后早期恢复质量,降低术后炎症应激反应,调节患者免疫平衡,有利于加快患者术后快速康复。
[关键词]" "肺癌;艾司氯胺酮;术后恢复质量;胸腔镜;炎症应激反应
[中图分类号]" "R614" " " " " " " nbsp;[文献标志码]" "A" " " " " " " "[文章编号]" "1674-7887(2024)03-0236-05
Effect of esketamine on the quality of postoperative recovery and inflammatory stress in patients undergoing thoracoscopic radical lung cancer treatment*
CHEN Lili**, WEI Lei, ZHANG Zhuoliang, LU Gang, PAN Jianhua***" " " " (Department of Anesthesiology, Suzhou Hospital of Nanjing Medical University, Jiangsu 215002)
[Abstract]" "Objective: To observe the effect of esketamine on the quality of postoperative recovery and inflammatory stress in patients undergoing radical thoracoscopic lung cancer treatment. Methods: Sixty patients who underwent thoracoscopic radical lung cancer surgery in Suzhou Hospital of Nanjing Medical University from September 2022 to May 2023 were selected, and were divided into the esketamine group(Group S) and the control group(Group C) using the randomized numerical table method, with 30 cases in each group. The anesthesia induction protocol was the same in both groups, and group S was injected with esketamine 0.25 mg/kg intravenously and continuously pumped intravenously to the suture skin at 0.15 mg/(kg·h). Group C was given the same dosage of saline after the induction of anesthesia and during the operation. The anesthesia time, operation time, extubation time, and postanesthesia care unit(PACU) stay time, the 40-item Quality of Recovery Questionnaire(QoR-40) scores at each time point of 24 h preoperatively(T0), 24 h postoperatively(T1), and 48 h postoperatively(T2) were recorded in the two groups, and the expression levels of TNF-α and IL-6 were detected by ELISA at the T0 and T2, and the incidence of complications such as delirium, nausea and vomiting, nightmare and dizziness were recorded for the patients in the two groups within 24 h. Results: There was no statistically significant difference in operation time, extubation time and PACU stay time between the two groups(Pgt;0.05). Intraoperative remifentanil consumption was significantly lower(Plt;0.05) and postoperative sufentanil consumption was significantly lower(Plt;0.05) in patients of group S compared with group C. The number of analgesic pump presses was significantly lower in group S than in group C during the postoperative period of 48 h(Plt;0.05). The preoperative total QoR-40 scores and various dimension scores of patients in the two groups were compared, and the differences were not statistically significant(Pgt;0.05). Compared with T1 period, the total QoR-40 scores as well as the scores of all dimensions of the patients in the two groups decreased significantly at T1 and T2 postoperatively, and the difference was statistically significant(Plt;0.05). Compared with the group C, the total QoR-40 score, physical comfort, psychological support and pain perception scores of the group S were significantly higher at T1, and the difference was statistically significant(Plt;0.05); the total QoR-40 score, physical comfort and pain perception scores of the group S were significantly higher than those of the group C at T2, and the difference was statistically significant(Plt;0.05). At T0, there was no statistically significant difference between the serum TNF-α and IL-6 levels of the two groups(Pgt;0.05). At T2, serum IL-6 and TNF-α levels were significantly higher in both groups(Plt;0.05), but were lower in the group S than in the group C(Plt;0.05). There was no difference in the comparison of the incidence of postoperative adverse reactions between the two groups(Pgt;0.05). Conclusion: Eslicarbazone can improve the quality of postoperative recovery in patients undergoing radical thoracoscopic lung cancer treatment, reduce postoperative inflammatory reactions, regulate the immune balance of patients, and contribute to accelerating the rapid recovery of patients in the postoperative period.
[Key words]" "lung cancer; esketamine; quality of postoperative recovery; thoracoscopy; inflammatory stress response
肺癌是全球范围内最常见的癌症之一,胸腔镜肺癌根治手术是治疗早期肺癌的首选方法[1]。然而,术后创伤、多处切口的刺激以及胸管对胸膜的刺激仍然会产生一系列的术后并发症和生理应激反应[2-3]。艾司氯胺酮是一种新型的N-甲基-D-天冬氨酸受体拮抗剂,具有较强的镇痛和镇静作用[4]。研究[5-6]表明,艾司氯胺酮可有效缓解术后疼痛,并能调节免疫和炎症反应减轻手术创伤后的应激。然而,关于艾司氯胺酮是否能够加快胸腔镜肺癌根治术后患者的术后恢复、抑制术后的炎症应激反应尚需进一步探讨。因此,本研究旨在探讨艾司氯胺酮对胸腔镜肺癌根治患者术后早期恢复质量及炎症反应的潜在影响,以期为改善患者术后的生存质量提供新的认识和方法。
1" "资料与方法
1.1" "一般资料" "选择2022年9月—2023年5月在南京医科大学附属苏州医院行胸腔镜肺癌根治术患者60例,纳入标准:(1)年龄30~70岁;(2)BMI 18~30 kg/m2;(3)ASA分级为Ⅰ~Ⅱ级;(4)临床TNM分期为Ⅰ或Ⅱ期。排除标准:(1)有胸部手术史;(2)存在严重的心肺、肝、肾合并症及手术禁忌证;(3)有吸毒史或酗酒史;(4)长期服用镇痛或抗精神类药物史;(5)合并内分泌系统和免疫系统疾病。排除标准:(1)中转开胸手术;(2)术中或术后发生严重药物不良反应;(3)围术期有输血史及抢救措施;(4)患者或家属因自身原因中途要求退出研究者。采用随机数字表法分为艾司氯胺酮组(S组)和对照组(C组),每组30例。本研究获得南京医科大学附属苏州医院伦理委员会审查批准(伦审号:K-2020-056-K01),所有患者或其家属签署知情同意书。
1.2" "麻醉方法" "患者术前禁食8 h、禁饮4 h,行心电、血压、SpO2和脑电意识深度(narcotrend, NT)监测,建立上肢静脉通路,桡动脉穿刺置管监测动脉血压。麻醉诱导:咪达唑仑0.04 mg/kg、丙泊酚1.5~2 mg/kg、舒芬太尼0.3~0.4 μg/kg、顺式阿曲库铵0.2 mg/kg。双腔支气管导管插管并连接麻醉机以控制呼吸。S组在麻醉诱导后静脉注射艾司氯胺酮0.25 mg/kg,并以0.15 mg/(kg·h)的速度持续静脉泵注至缝皮。C组则通过静脉注射等量的生理盐水。麻醉维持过程中,通过静脉泵注瑞芬太尼(0.1~0.3) μg/(kg·min),吸入浓度1%~2%七氟醚,静脉泵注顺式阿曲库铵5~8 mg/h维持肌松,同时维持NT值20~46。手术结束后,连接静脉自控电子泵。术后镇痛方案为舒芬太尼0.05 μg/kg+格拉司琼0.15 mg/kg加生理盐水至100 mL,输注速率为1.5 mL/h,连续输注48 h,每次自控追加容量为1.5 mL,锁定时间20 min。
1.3" "观察指标" "记录两组患者的性别、年龄、BMI、ASA分级、麻醉时间、手术时间、拔管时间以及术后恢复室(postanesthesia care unit, PACU)停留时间。比较两组患者阿片类药物消耗量与术后48 h内镇痛泵按压次数,术前24 h(T0)、术后24 h(T1)、术后48 h(T2)的40项恢复质量量表(40-item Quality of Recovery Questionnaire, QoR-40)评分,评估手术及麻醉后恢复的5个维度的感受:(1)身体舒适度(60分);(2)情绪状态(45分);(3)自理能力(25分);(4)心理支持(35分);(5)疼痛感受(35分)。每个问题5分,共40个问题,总分200分,得分越高患者恢复状态越好。分别检测患者T0、T2时TNF-α、IL-6的表达水平,记录两组患者术后24 h内谵妄、恶心呕吐、噩梦、头晕等并发症的发生情况。
1.4" "统计学方法" "数据处理采用SPSS 25.0软件,计量资料以X±s表示,组内比较采用重复测量方差分析,组间比较采用两独立样本t检验;计数资料采用频数和率(%)进行描述,组间比较采用χ2检验或Fisher精确检验。Plt;0.05为差异有统计学意义。
2" "结" " " 果
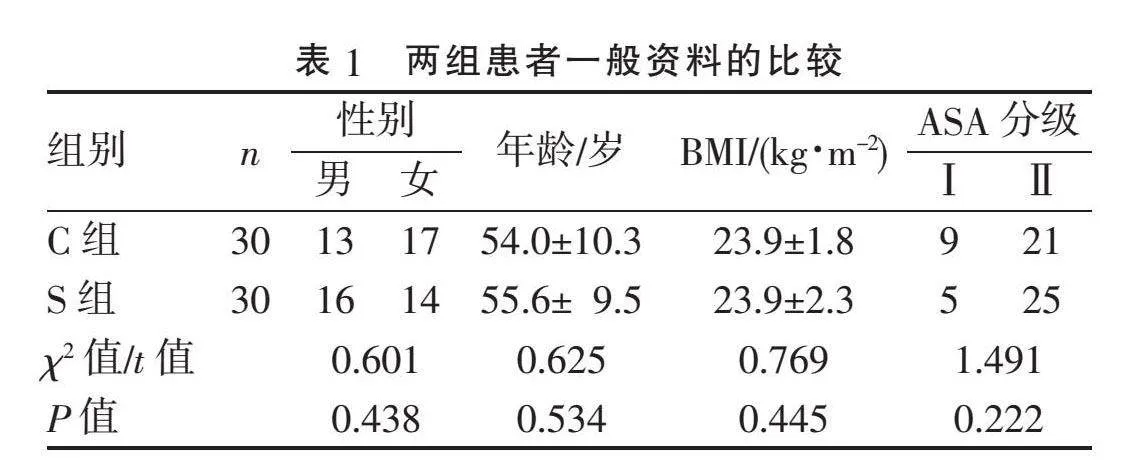
2.1" "两组患者一般资料比较" "两组患者年龄、性别、BMI、ASA分级差异均无统计学意义(均Pgt;0.05),见表1。
2.2" "两组患者围术期临床指标比较" "与C组相比,S组患者手术时间、拔管时间、PACU停留时间差异无统计学意义(Pgt;0.05),术中瑞芬太尼消耗量显著降低(Plt;0.05),术后舒芬太尼消耗量显著下降(Plt;0.05),术后48 h内镇痛泵按压次数显著少于C组(Plt;0.05),见表2。
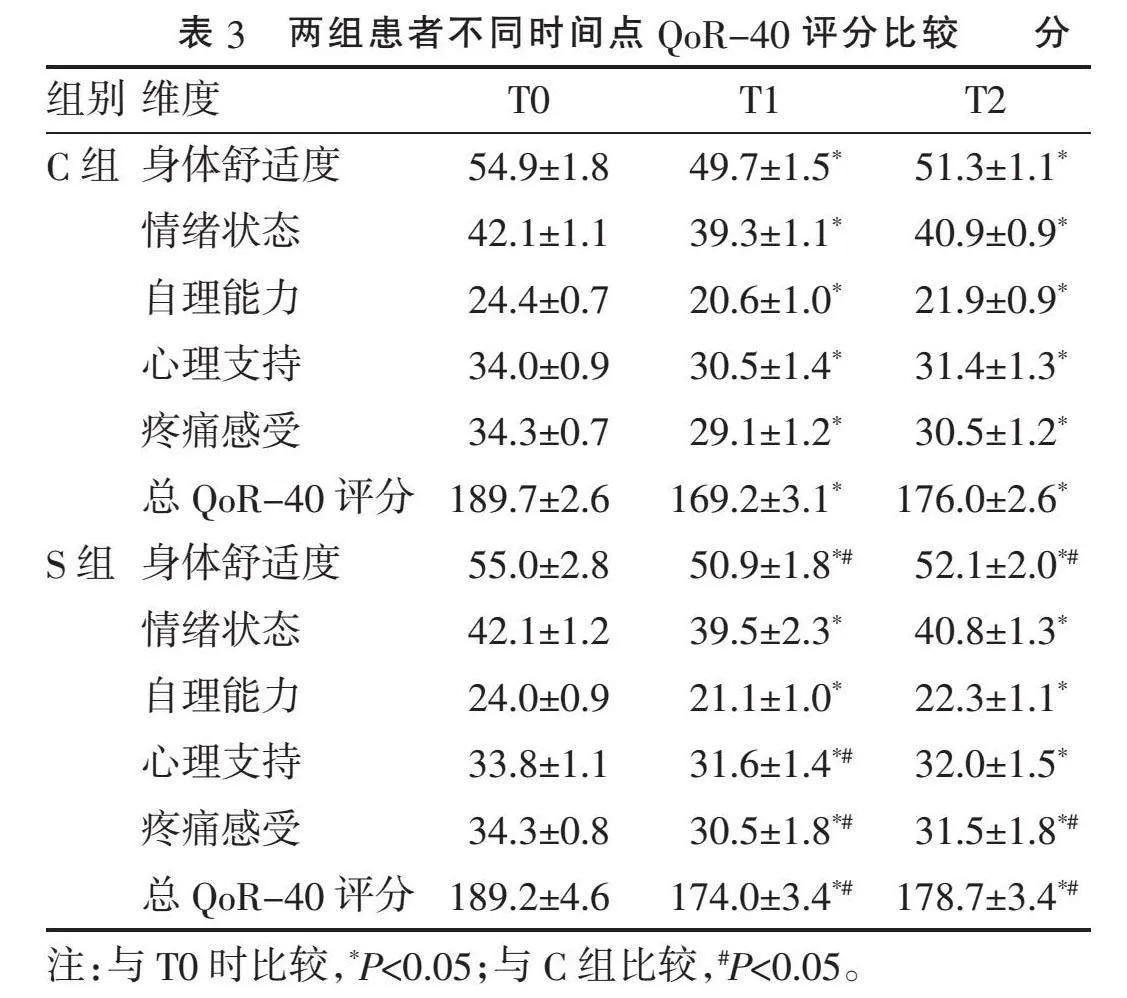
2.3" "两组患者不同时间点QoR-40评分的比较" "两组患者T0时QoR-40评分差异无统计学意义(Pgt;0.05),T1、T2时总QoR-40评分以及各项维度评分均较T0明显下降(Plt;0.05)。S组T1时总QoR-40评分、身体舒适度、心理支持和疼痛感受评分均较C组明显升高(均Plt;0.05);T2时总QoR-40评分、身体舒适度和疼痛感受评分均明显高于C组(均Plt;0.05),见表3。
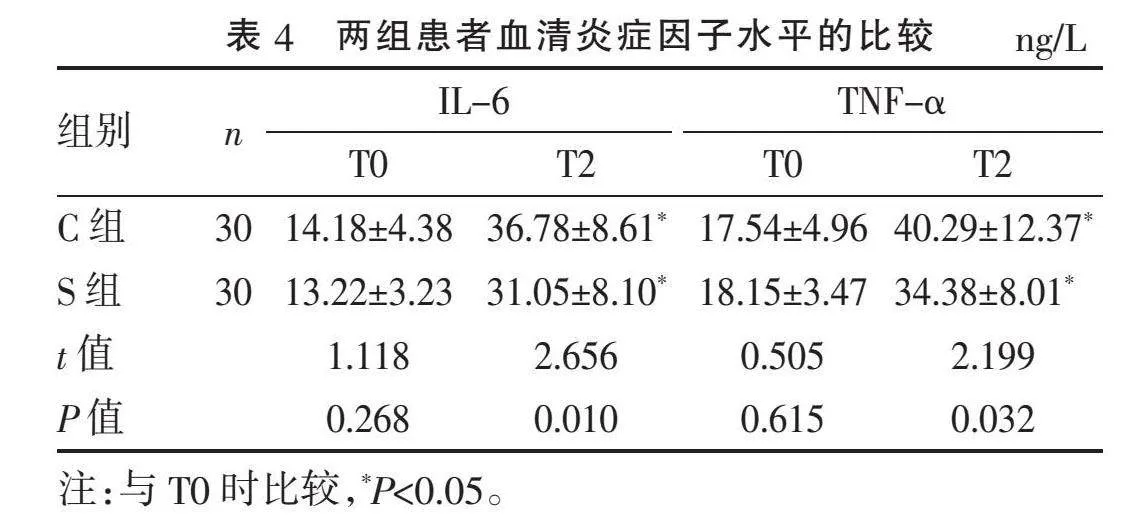
2.4" "两组患者炎症因子水平的比较" "两组患者T0时的血清炎症因子IL-6和TNF-α水平比较差异无统计学意义(Pgt;0.05)。T2时,两组患者血清IL-6和TNF-α水平均显著升高(Plt;0.05),但S组均低于C组(Plt;0.05),见表4。
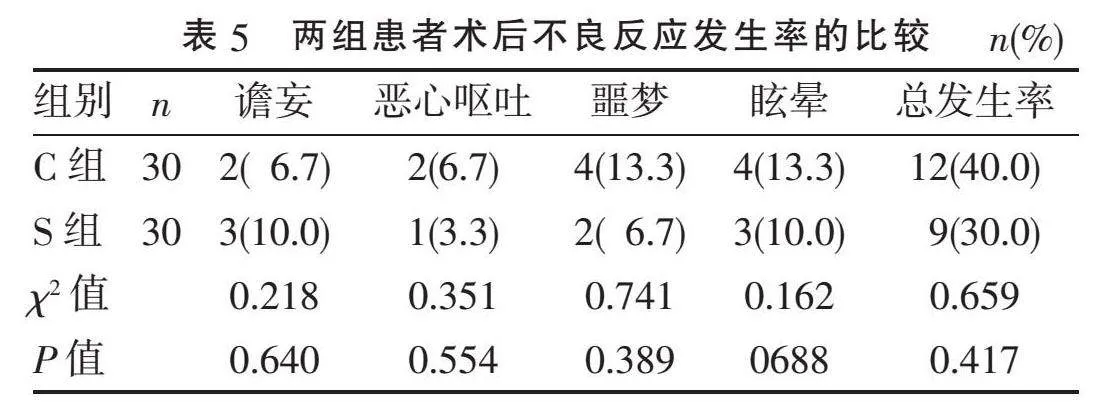
2.5" "两组患者术后不良反应发生率的比较" "两组术后不良反应发生率比较差异无统计学意义(Pgt;0.05),见表5。
3" "讨" " " 论
胸腔镜手术临床用于切除肺部肿瘤越来越广泛,然而患者常面临术后疼痛的困扰,这可能会对肺功能的早期恢复产生负面影响,可导致术后肺部炎症、低氧血症、肺不张等严重并发症[7-8]。研究[9]表明,艾司氯胺酮作为一种有效的辅助镇痛药物,在胸腔镜术后的恢复过程中发挥着重要作用。艾司氯胺酮是氯胺酮的右旋结构,可以显著降低阿片类药物的使用量,从而减缓患者对药物的耐受性,同时也有利于患者更早活动、翻身和进行肺功能锻炼,促进术后康复。因此,参考国内外文献[10-12],本研究选择麻醉诱导后静脉注射艾司氯胺酮0.25 mg/kg,术中以0.15 mg/(kg·h)静脉泵注用于胸腔镜下肺叶切除术患者。
QoR-40评分量表涵盖了康复过程中的多个方面,包括身体舒适度、情绪状态、自理能力、心理支持和疼痛感受等,具有全面性和个体化的优势,能从多维度对术后恢复质量进行评估[13]。本研究表明,S组术后24、48 h总QoR-40评分显著高于C组,可有效提高患者术后恢复质量,减轻患者疼痛。S组的阿片类药物消耗量和镇痛泵主动按压次数均显著低于C组,说明艾司氯胺酮具有良好镇痛作用的同时,可减少术中阿片类药物的使用量。X.CHENG等[14]研究表明,静脉输注艾司氯胺酮0.25 mg/kg,术中以0.15 mg/(kg·h)静脉泵注可以提高接受胸腔镜手术患者的康复质量,同时还具有改善术后镇痛和术后抑郁的作用。Z.HUANG等[15]认为,采用艾司氯胺酮联合右美托咪定能有效提高患者的术后康复质量,并减少心动过缓的发生,但联合应用可能会延长患者清醒时间、拔管时间以及在PACU的停留时间。因此,临床应用时需研究艾司氯胺酮的合适剂量,以平衡其带来的术后康复优势和患者术后不适。
手术创伤是一种破坏性的生理过程,能激发机体的炎症反应。在手术创伤初期,损伤的组织释放信号分子(包括TNF-α和IL-6),TNF-α参与细胞免疫调节和炎症调控,而IL-6在免疫和炎症应答中具有多方面的功能。它们的释放激活了免疫细胞,引导其向损伤部位迁移,清除受损细胞并防御可能的感染。尽管适度的炎症反应对于组织修复至关重要,但过度的炎症反应可能导致全身性炎症反应综合征等[16-18]。研究[19]表明,艾司氯胺酮[0.2 mg/kg负荷,0.2 mg/(kg·h)维持]提高了术后24 h的恢复质量,减轻了炎症反应,同时不增加不良反应的发生率。I.D.WELTERS等[20]亦发现,艾司氯胺酮能显著降低冠脉搭桥术后IL-6和IL-8的水平,减轻体外循环诱导的全身炎症反应。本研究中,两组患者血清TNF-α和IL-6水平在术后48 h均有不同程度的升高,但S组明显低于C组,提示艾司氯胺酮能减轻全身性的炎症反应,减轻疼痛感,这可能是艾司氯胺酮提高患者术后恢复质量的重要机制之一。
本研究的局限:(1)为单中心试验,未来还需要结合多中心研究,提高外部推广性;(2)仅选择单一剂量艾司氯胺酮在围术期应用,并未研究其他剂量,仍需进一步探索更理想的剂量;(3)样本量较小,增加了随机误差的可能,需更大规模的研究来全面探讨艾司氯胺酮对术后恢复与炎症反应的影响。
综上所述,艾司氯胺酮有助于减轻胸腔镜肺癌根治术后的疼痛感,提高患者的恢复质量;同时,艾司氯胺酮通过调节免疫平衡,抑制身体过度的炎症应激反应,有利于患者的快速康复。
[参考文献]
[1]" "SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3):209-249.
[2]" "MOORTHY A, N?魱 EOCHAG?魣IN A, DEMPSEY E, et al. Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: a prospective, randomised controlled trial[J]. Br J Anaesth, 2023, 130(1):e137-e147.
[3]" "SUN K, LIU D Y, CHEN J, et al. Moderate-severe postoperative pain in patients undergoing video-assisted thoracoscopic surgery: a retrospective study[J]. Sci Rep, 2020, 10(1):795.
[4]" "WANG X M, LIN C, LAN L F, et al. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis[J]. J Clin Anesth, 2021, 68:110071.
[5]" "刘永, 钟祥鹏, 张亮, 等. 艾司氯胺酮联合舒芬太尼PCIA对肾移植患者术后镇痛效果和早期肾功能的影响[J]. 川北医学院学报, 2023, 38(10):1322-1325.
[6]" "TU W C, YUAN H B, ZHANG S J, et al. Influence of anesthetic induction of propofol combined with esketamine on perioperative stress and inflammatory responses and postoperative cognition of elderly surgical patients[J]. Am J Transl Res, 2021, 13(3):1701-1709.
[7]" "CARUANA E, STEINER M C. Perioperative rehabilitation in thoracic surgery: get up and go![J]. Thorax, 2023, 78(1):1-2.
[8]" "ZHENG Y, MAO M, LI F, et al. Effects of enhanced recovery after surgery plus pulmonary rehabilitation on complications after video-assisted lung cancer surgery: a multicentre randomised controlled trial[J]. Thorax, 2023, 78(6):574-586.
[9]" "YAN H, CHEN W N, CHEN Y W, et al. Opioid-free versus opioid-based anesthesia on postoperative pain after thoracoscopic surgery: the use of intravenous and epidural esketamine[J]. Anesth Analg, 2023, 137(2):399-408.
[10]" "王金凤, 徐海军, 戚钰, 等. 艾司氯胺酮复合舒芬太尼自控静脉镇痛对胸腔镜肺癌根治患者术后疲劳及免疫功能的影响[J]. 中国临床医学, 2022, 29(6):982-986.
[11]" "谢本发, 何睿, 许伟, 等. 预先静脉注射艾司氯胺酮对腹腔镜胆囊切除术患者术后疼痛效果及并发症的影响[J]. 河北医学, 2022, 28(11):1896-1901.
[12]" "CHENG Y, XUE F S, LI C W. Effects of the different doses of esketamine on postoperative quality of recovery in patients undergoing modified radical mastectomy: a randomized, double-blind, controlled trial [letter][J]. Drug Des Devel Ther, 2023, 17:937-938.
[13]" "VIGNAUD M, MOREL C, HENAULT A, et al. Variability and reliability of the French version of the Quality of Recovery-40 Questionnaire(QoR-40)[J]. Anaesth Crit Care Pain Med, 2021, 40(2):100822.
[14]" "CHENG X, WANG H, DIAO M M, et al. Effect of S-ketamine on postoperative quality of recovery in patients undergoing video-assisted thoracic surgery[J]. J Cardiothorac Vasc Anesth, 2022, 36(8 Pt B):3049-3056.
[15]" "HUANG Z, LIU N, HU S H, et al. Effect of dexmedetomidine and two different doses of esketamine combined infusion on the quality of recovery in patients undergoing modified radical mastectomy for breast cancer-A randomised controlled study[J]. Drug Des Devel Ther, 2023, 17:2613-2621.
[16]" "ZHANG W C, WANG T L, WANG G, et al. Effects of dexmedetomidine on postoperative delirium and expression of IL-1β, IL-6, and TNF-α in elderly patients after hip fracture operation[J]. Front Pharmacol, 2020, 11:678.
[17]" "SARIBAL D, HOCAOGLU-EMRE F S, ERDOGAN S, et al. Inflammatory cytokines IL-6 and TNF-α in patients with hip fracture[J]. Osteoporos Int, 2019, 30(5):1025-1031.
[18]" "BAIN C R, MYLES P S, MARTIN C, et al. Postoperative systemic inflammation after major abdominal surgery: patient-centred outcomes[J]. Anaesthesia, 2023, 78(11):1365-1375.
[19]" "GAO W Y, LI H T, LI T, et al. Effects of S-ketamine on postoperative recovery quality and inflammatory response in patients undergoing modified radical mastectomy[J]. Pain Ther, 2023, 12(5):1165-1178.
[20]" "WELTERS I D, FEURER M K, PREISS V, et al. Continuous S-(+)-ketamine administration during elective coronary artery bypass graft surgery attenuates pro-inflammatory cytokine response during and after cardiopulmonary bypass[J]. Br J Anaesth, 2011, 106(2):172-179.
[收稿日期] 2024-03-11
猜你喜欢
保健医苑(2023年2期)2023-03-15 09:03:04
中国临床医学影像杂志(2022年2期)2022-05-25 13:24:34
国际呼吸杂志(2019年5期)2019-03-30 01:38:08
腹腔镜外科杂志(2016年12期)2016-06-01 12:10:09
腹腔镜外科杂志(2016年9期)2016-06-01 12:10:07
癌变·畸变·突变(2016年3期)2016-02-27 06:15:34
医学研究杂志(2015年12期)2015-06-10 06:57:46
郑州大学学报(医学版)(2015年1期)2015-02-27 14:50:26
福建医科大学学报(2014年6期)2014-03-20 13:42:28
河北医科大学学报(2011年8期)2011-03-25 10:16:56