
A 10-year fight for vision in a patient with recurrent uveal melanoma: a case report
2023-10-21 03:17HengWangJingTingLuoYangXuTaoYangLiWenBinWei
Heng Wang, Jing-Ting Luo, Yang-Xu Tao, Yang Li, Wen-Bin Wei
Beijing Tongren Eye Center, Beijing Key Laboratory of Intraocular Tumor Diagnosis and Treatment, Beijing
Ophthalmology & Visual Sciences Key Lab, Medical Artificial Intelligence Research and Verification Key Laboratory of the
Ministry of Industry and Information Technology, Beijing Tongren Hospital, Capital Medical University, Beijing 100730,China
Dear Editor,
Uveal melanoma (UM) is the most common primary intraocular malignancy in adults[1].We are writing to present a case of recurrent UM.This case presents an important clinical challenge: vision preservation in patients with recurrent anterior UM, especially in young patients.Informed consent was obtained from the patient.This case study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Beijing Tongren Hospital(approval number: TRECKY2018-056).
CASE PRESENTATION
A 42-year-old woman presented to our department in 2008 with decreased visual acuity (VA) in her left eye for ten days without any other visual symptoms.On examination, the corrected distance VA was 20/40 (left) and 20/25 (right).Intraocular pressure (IOP) was mildly elevated in her left eye (24 mm Hg).Slit lamp examination after pupillary dilation found a supranasal, pigmented, ciliary body neoplasm with local iris bulging in her left eye (Figure 1A), and local angle invasion was found by gonioscopy.Magnetic resonance imaging showed that the neoplasm was hyperintense on T1-weighted and hypointense on T2-weighted images with enhancement(Figure 1B).A pigmented iris nevus was found in her right eye.The fundus of both eyes was normal.Ciliary body melanoma in the left eye was suspected.Since the patient was motivated to conserve the eye and preserve vision, we performed a transscleral local tumor resection with 1-2 mm margins for safety.Lensectomy and vitrectomy were performed simultaneously to ensure tumor removal and reduce complications.A 6×6×5 mm3pigmented neoplasm was removed and classified as T1b according to the American Joint Committee on Cancer Consensus (8thedition) staging.Histopathological examination revealed spindle-cell type melanoma (Figure 1C).Secondary intraocular lens implantation was carried out in March 2009.Regular follow-up was performed.
In September 2014, the corrected distance VA of her left eye was 20/30, and the IOP reached 55 mm Hg.Pigmented lesions were found at the 6 o’clock of the anterior chamber angle in the left eye.After anti-glaucoma medication treatment and cyclophotocoagulation, the IOP decreased for a short time but still increased in the long run.The corrected distance VA of her left eye progressively got worse (20/100).In May 2016, a diffuse brown-black iris-ciliary body tumor was observed from 2 to 6 o’clock in the left eye (Figure 2) with no evidence of systemic metastasis.Almost entire iris and ciliary body showed irregular low signal in ultrasound biomicroscopy (Figure 2A).The patient subsequently accepted I-125 brachytherapy in the left eye.The radiation dose was 100 Gy at the apex of the tumor, and the dose rate was 25.775 mGy/mCi.hr.In October 2016, the corrected distance VA of the left eye was 20/2000,and the IOP was 27 mm Hg.
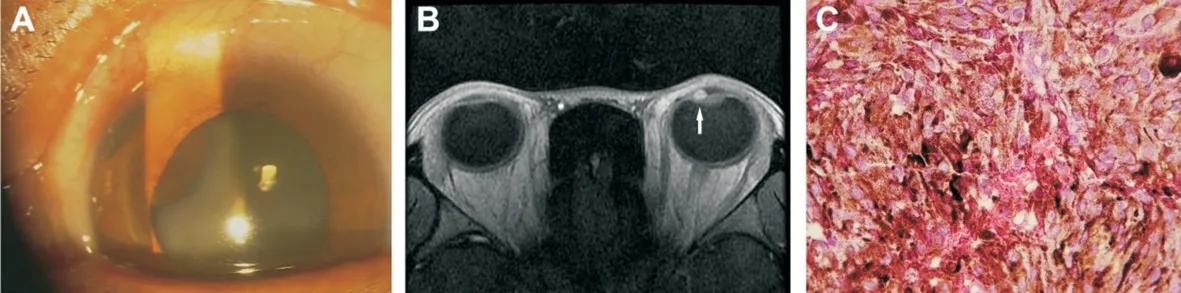
Figure 1 Photography of lefteye at the first visit A: Slit lamp examination found a pigmented ciliary body neoplasm from 9 to 11 o’clock with local iris bulging in her lefteye; B: Magnetic resonance imaging showed that the neoplasm (arrow) was hyperintense on T1-weighted and hypointense on T2-weighted images with enhancement; C: On histopathological examination, the tumor exhibited spindle-cell type ciliary melanoma.

Figure 2 Photography of lefteye in May 2016, before receiving I-125 brachytherapy A: Ultrasound biomicroscopy showed a diffuse iris-ciliary body neoplasm (arrow) with uneven internal echo, mainly with middle and low echo; B: Magnetic resonance imaging revealed a temporal irisciliary body tumor in the lefteye (arrow); C: Slit lamp photography showing a brown-black tumor from 2 to 6 o’clock in the lefteye.

Figure 3 Photography of lefteye in 2017 and 2018 A: Ultrasound biomicroscopy showed the neoplasm (arrow) with irregular acoustic echo in 2017; B: Ultrasound showed an increased tumor size (arrow) in 2018; C: The pathological diagnosis was iris and ciliary body melanoma,epithelial-cell type.
In June 2017, the corrected distance VA of the left eye was light perception, and the IOP was 40 mm Hg.The lesion was relatively stable (Figure 3A).Endoscopic cyclophotocoagulation over 270° of the ciliary body in the left eye was performed and local anti-glaucoma medications were prescribed to control the IOP.However, the IOP was poor controlled.In March 2018, the patient complained of persistent eye pain.The corrected distance VA of the left eye was no light perception and the IOP reached 52 mm Hg.Color Doppler imaging showed the tumor grew (Figure 3B).Therefore,enucleation and artificial eye implantation was performed.The pathological diagnosis were iris and ciliary body melanoma,epithelial-cell type (Figure 3C).Bulk RNA sequencing was performed.We adopted the Gene Expression Profiling (GEP)system proposed by Harbour[2]- to classify this UM sample into Class 1.The patient has been followed up for 14y since 2008 and is currently alive without metastasis.The pigmented iris nevus in the right eye was stable and still under regular follow-up.
DISCUSSION
Vision preservation should be considered an important task,especially for young patients in UM treatment.This study made a great effort to preserve the vision of a patient with recurrent anterior UM.Our patient started initial treatment in 2008, relapsed in 2016, and had her eyeball removed in 2018.Her VA was preserved for 10y, and no systemic metastasis was found during the 14-year follow-up.
We performed surgical resection initially, not only to preserve the vision but also to make the histopathological diagnosis.In some cases, it may be difficult to distinguish UM from other tumors, such as melanocytoma, adenoma of nonpigmented epithelium, adenoma of pigmented epithelium, and medulloepithelioma based on clinical manifestations.Local resection offers several theoretical advantages over enucleation and radiotherapy.It can satisfy cosmetic demand and achieve intraocular tumor control and vision preservation[3].
Local recurrence typically occurs within months to a few years after resection of ciliary body melanomas.Our patient developed a ring melanoma, which has been reported after local tumor resection[4].Recurrent anterior UM is usually managed by brachytherapy and enucleation.Our case indicates that brachytherapy could be considered an option for salvage therapy for local recurrence of nonresectable diffuse iris and ciliary body melanoma.A personalized retreatment strategy with brachytherapy may offer a high probability of tumor control and organ preservation[5].
The timeline of vision loss was consistent with the IOP elevation.The patient suffered from persistently elevated IOP, which may be related to tumor invasion, surgery,and radiotherapy.We reflect on the possibility that a local recurrence led to IOP elevation.Brachytherapy can kill tumor cells and may help control IOP and preserve the patient’s vision for a longer time.Glaucoma is one of the most common complications of UM, which can lead to irreversible visual loss and great pain.We highlight the significance of IOP monitoring and glaucoma treatment in the management of UM.
GEP, genetic mutations, and chromosome abnormalities are also associated with patient outcomes and shed light on the prognosis of UM.Tumor biopsy for genetic testing might be beneficial for clinicians to make clinical decisions in practice.In our patient, the tumor exhibited an alteration in pathological type from spindle to epithelioid type.We assume that the tumor cells may residue after treatments.Therefore, the heterogeneity of tumor cells and selective clone growth may lead to the change of pathological type.
ACKNOWLEDGEMENTS
Foundations:Supported by National Natural Science Foundation of China (No.82141128); the Capital Health Research and Development of Special (No.2020-1-2052);Beijing Natural Science Foundation (No.7204245); Science& Technology Project of Beijing Municipal Science& Technology Commission (No.Z201100005520045;No.Z181100001818003); Scientific Research Common Program of Beijing Municipal Commission of Education (No.KM202010025018); Beijing Municipal Administration of Hospitals’ Youth Programme (No.QML20190202); Beijing Dongcheng District Outstanding Talents Cultivating Plan(No.2018).
Conflicts of Interest: Wang H,None;Luo JT,None;Tao YX,None;Li Y,None;Wei WB,None.
 International Journal of Ophthalmology2023年10期
International Journal of Ophthalmology2023年10期
- International Journal of Ophthalmology的其它文章
- A novel approach for 25-gauge transconjunctival sutureless vitrectomy to evaluate vitreous substitutes in rabbits
- Visual resolution under photopic and mesopic conditions in patients with Sjögren's syndrome
- Effects of obstructive sleep apnea on retinal microvasculature
- Bibliometric analysis of research relating to refractive cataract surgery over a 20-year period: from 2003 to 2022
- Three-dimensional bioprinting in ophthalmic care
- Agreement of intraocular pressure measurement with Corvis ST, non-contact tonometer, and Goldmann applanation tonometer in children with ocular hypertension and related factors