
Renin-angiotensin system in the central nervous system: focus on Huntington’s disease
2023-03-23 08:13AlineSilvadeMirandaAntonioLucioTeixeira
中国神经再生研究(英文版) 2023年10期
Aline Silva de Miranda, Antonio Lucio Teixeira
The renin-angiotensin system (RAS) was originally conceived as a circulating hormonal system involved in the regulation of cardiovascular and renal homeostasis.With the discovery of local RAS components in diverse organs, including the brain, and related biologically active peptides,enzymes, and receptors, the understanding of the physiological and pathophysiological roles of RAS has changed significantly.Accordingly, RAS has been conceptualized as a system composed of two major axes: a“classical”one formed by the angiotensin-converting enzyme (ACE),angiotensin II (Ang II), and angiotensin type 1(AT1) receptor (ACE/Ang II/AT1), and a‘counterregulatory’one composed by the ACE2, Ang-(1-7),Mas receptor (ACE2/Ang-(1-7)/Mas).The classical arm promotes vasoconstriction, pro-inflammatory,pro-thrombotic, and pro-fibrotic effects mainly through the activation of AT1 receptors.Ang II can also bind to AT type 2 receptor but with much less affinity and with distinct effects of AT1.The counter-regulatory axis ACE2/Ang-(1-7)/Mas often opposes the actions of the classical arm,promoting anti-inflammatory, anti-oxidant, antiapoptotic, and anti-fibrotic effects (Miranda et al.,2022).
Therapeutic approaches aiming to inhibit the ACE/Ang II/AT1 axis activation and/or to promote ACE2/Ang-(1-7)/Mas axis functioning have been developed for different medical conditions (Miranda et al., 2022).ACE inhibitors(e.g., lisinopril) and AT1 receptor antagonists(e.g., candesartan) are currently used in the treatment of hypertension and heart failure.Intravenous administration of Ang-(1-7), as well as oral treatment with an Ang-(1-7) cyclodextrin formulation, has shown promising results in experimental models of post-myocardial infarction heart failure (Machado-Silva et al., 2016).Preclinical (or experimental) and clinical studies have also demonstrated the protective effects of the treatment with ACE inhibitors and AT1 receptor antagonists (ARAs) in neurodegenerative diseases,supporting the involvement of RAS peptides in central nervous system dysfunction (Miranda et al., 2022).Epidemiological studies have shown a reduced risk of Alzheimer’s disease (AD) and aging-related cognitive decline in individuals under ACE inhibitors and/or ARAs therapies (Zhuang et al., 2016).Similarly, the use of ARAs significantly decreased the risk of Parkinson’s disease (PD) in patients with an ischemic heart condition (Jo et al., 2022).
Although accumulating evidence has reinforced the contribution of RAS components in both AD and PD (Miranda et al., 2022), the involvement of this system in other less common neurodegenerative disorders, like Huntington’s disease (HD), remains unclear.Herein, we will discuss the evidence of RAS involvement in the pathophysiology of HD, the related knowledge gaps, as well as the potential therapeutic role of RAS modulation for this highly disabling condition.HD is an autosomal-dominant inherited neurodegenerative disease caused by abnormal expansion of CAG trinucleotide repeats in theHuntingtingene (HTT) located on chromosome 4.This mutation promotes huntingtin misfolding and the formation of toxic soluble oligomers in the nucleus and cytoplasm of neurons.Progressive accumulation of mutant huntingtin (mHTT)within neurons followed by degeneration of brain areas such as the striatum, cerebral cortex,hippocampus, and brainstem, contribute to the constellation of motor, cognitive and behavioral symptoms observed in HD.Given the genetic nature of the disease that allows the recognition of pre-symptomatic cases, and the fact that the progression of HD symptoms occurs in parallel with neuropathological changes, HD is a unique model to investigate neurobiological mechanisms of neurodegeneration (McColgan and Tabrizi,2018).
Although the toxic gain of function ofmHTTalongside a loss of function of the normalHTTprotein is regarded as the main contributors to neurodegeneration in HD, additional mechanisms are involved, including inflammation, oxidative stress, and mitochondrial dysfunction (McColgan and Tabrizi, 2018; Furlam et al., 2022).The recognition that RAS components are present in the brain opens new venues for the study of the potential contribution of RAS in the pathophysiology of neurodegenerative diseases,including HD.Although there is evidence that RAS components can induce tau phosphorylation and amyloid β peptide production in AD models,whether RAS contributes to huntingtin misfolding and aggregation remains unknown (Miranda et al., 2022).The first evidence that RAS components may play a role in HD came from a post-mortem study in the late 1970s showing a significant decrease in ACE activity in the striatum (globus pallidus, caudate, and putamen) of HD patients compared with healthy controls.Increased concentration of ACE was also found in the cerebrospinal fluid of HD patients compared with controls.Differences in methodological approaches as well as in the biological sample analyzed,i.e.brain tissue or cerebrospinal fluid, explain,at least in part, these contradicting findings.Later, radiolabelled ATl receptor recognition site levels were decreased by approximately 35% in the putamen from post-mortem patients with HD relative to control individuals who had died without a neurological or a psychiatric disorder.No significant differences were found in the AT1 receptor levels in the caudate nucleus and substantia nigra of HD patients (Ge et al., 1996).Studies are necessary to investigate the levels of RAS counter-regulatory components in brain areas implicated in HD.Recently, clinical studies provided preliminary evidence that the activation of the RAS counterregulatory axis formed by ACE2/Ang-(1-7)/Mas receptors might contribute to mitigating HD symptoms (Rocha et al., 2020; Kangussu et al., 2022).Manifest HD gene carriers presented higher plasma levels of Ang-(1-7) in comparison with healthy controls (Kangussu et al., 2022).The increased levels of Ang-(1-7) in the plasma of HD patients might be an attempt of the system to counteract pathophysiological events, such as inflammation and oxidative stress, in the course of HD.No significant differences were found in the plasma levels of the RAS components Ang II, ACE, and ACE2 when comparing controls,premanifest, and manifest HD gene carriers(Rocha et al., 2020).However, positive correlations were found between ACE2 and Verbal Fluency Test scores, therefore, higher circulating levels of ACE2 were associated with better cognitive functioning in HD.A negative correlation between Ang II concentrations and general cognition, as assessed by the Mini-Mental State Examination,was also observed, indicating that activation of the RAS classical axis was associated with worse cognitive performance in HD (Rocha et al., 2020).These findings are in line with previous studies in other neurodegenerative conditions showing that the RAS counter-regulatory axis activation can promote neuroprotective or positive effects while the activation of the classical arm contributes to neurodegeneration and worse cognitive and behavioral symptoms (Miranda et al., 2022).
Emerging evidence from pre-clinical studies reinforces the hypothesis that both RAS classical and counter-regulatory axes are involved in HD pathophysiology.For instance, oral administration of trandolapril, an ACE inhibitor, daily for 12 days attenuated weight loss, locomotor and cognitive impairments in a rat model of HD induced by the infusion of 3-nitropropionic acid in the striatum.Trandolapril improvements in HD-related motor and behavioral symptoms were related to a reduction in oxidative stress and mitochondrial enzyme activities in the brain (Hariharan et al., 2014).The BACHD mice, a well-established transgenic model of HD, display significant motor deficits alongside increased mRNA expression of AT1 receptors in key brain areas like the striatum.Motor performance decline was also associated with decreased expression and activity of RAS counter-regulatory components ACE2/Ang-(1-7)/Mas receptors in BACH mice brains compared with their littermate controls (Kangussu et al., 2022).Altogether, these data support an imbalance between the RAS classical ACE/Ang II/AT1 and counter-regulatory ACE2/Ang-(1-7)/Mas receptor axes in HD, as previously reported in other neurodegenerative diseases such as AD and PD (Miranda et al., 2022).Importantly, the discrepancies in the expression of AT1 receptors found in the brain of HD patients (Ge et al., 1996)and in the brain of BACH mice (Kangussu et al.,2022) might be, at least in part, explained by differences on methodological approaches.In the human study, ATI levels were determined by radioligand binding techniques while in the BACHD murine model real-time PCR measured ATI mRNA expression.Furthermore, the human study analyzed specific areas of the dorsal striatum like the putamen and the caudate nuclei, whereas the experimental study assessed the whole striatum(Ge et al., 1996; Kangussu et al., 2022).
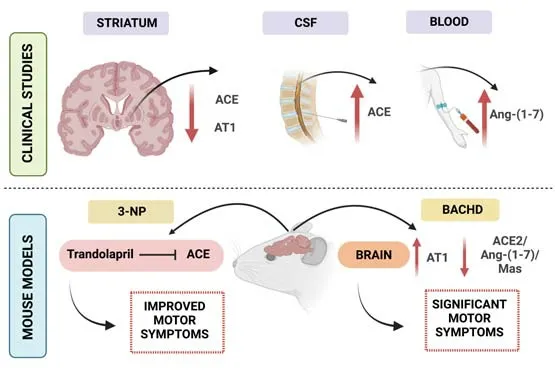
Figure 1|Evidence from clinical and pre-clinical (experimental) studies of renin-angiotensin system (RAS)components in Huntington’s disease (HD) pathophysiology.
As shown above, the available experimental and clinical data (Figure 1) on the involvement of RAS in HD are largely descriptive and correlational,lacking mechanistic insights directly linking the RAS components to the pathophysiology of HD.Another major drawback is the absence of clinical trials aiming to evaluate specific effects of RAS modulators like ACE inhibitors and ARAs in HD patients.A single observational study showed that hypertensive HD patients treated with antihypertensive drugs, including ACE inhibitors and ARAs, had less motor, cognitive and total functional capacity impairments as well as attenuated anxiety and depressive symptoms compared with normotensive and untreated hypertensive HD patients (Steventon et al., 2020).While the beneficial effects of anti-hypertensive medications in HD patients with hypertension seem evident,it remains to be determined whether RAS modulators would provide additional benefits compared to other antihypertensive strategies(e.g., beta blockers, diuretics).Furthermore, it would be interesting to evaluate the potential neuroprotective effects of ACE inhibitors and ARAs in normotensive HD patients.Of note, a proofof-concept, double-blind, placebo-controlled,crossover study conducted with moderately affected normotensive PD patients revealed that the ACE inhibitor perindopril was able to improve motor symptoms (Reardon et al., 2000).
Furthermore, studies addressing whether ACE2 activators and/or Mas receptor agonists might benefit HD are still lacking.For that, the development of drugs capable of crossing the blood-brain barrier as well as strategies to avoid proteolytic degradation of short peptides like Ang-(1-7) are warranted.The encapsulation of Ang-(1-7) in cyclodextrin or microencapsulated in biodegradable polymers or liposomes has been proposed and may enable the oral administration of Ang-(1-7) (Machado-Silva et al., 2016).Finally,the involvement of other RAS components remains to be investigated in HD.Among promising targets,it is worth mentioning the angiotensin II type 2 receptor whose signaling also tends to oppose the AT1 effects (Miranda et al., 2022).
In sum, the available experimental and clinical evidence supports a role for RAS in the pathophysiology of HD.Whether inhibition/antagonism of the ACE/Ang II/AT1 receptor axis or the activation of the ACE2/Ang-(1-7)/Mas receptor axis may improve HD outcomes remains to be determined.These questions are very relevant while no disease-modifying strategies are available for HD.
ASM and ALT have received financial support from the Brazilian government funding agencies:FAPEMIG (Fundação de Amparo à Pesquisa do Estado de Minas Gerais, Brazil), CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil) and CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior).ALT received financial support from UTHealth Department of Psychiatry and Behavioral Sciences,NIH/NIA, TARCC.ASM and ALT are CNPq fellowship recipients.
Aline Silva de Miranda*,Antonio Lucio Teixeira*
Laboratório de Neurobiologia, Departamento de Morfologia, Instituto de Ciências Biológicas,Universidade Federal de Minas Gerais (UFMG),Belo Horizonte, MG, Brasil (de Miranda AS)Laboratório Interdisciplinar de Investigação Médica(LIIM), Faculdade de Medicina, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte,MG, Brasil (de Miranda AS)Neuropsychiatry Program, Department of Psychiatry and Behavioral Sciences, McGovern Medical School, University of Texas Health Science Center at Houston, TX, USA (Teixeira AL)Faculdade Santa Casa BH, Belo Horizonte, MG,Brasil (Teixeira AL)
*Correspondence to:Aline Silva de Miranda, PhD,mirandas.aline@gmail.com; Antonio Lucio Teixeira,MD, PhD, antonio.L.Teixeira@uth.tmc.edu.https://orcid.org/0000-0003-2811-7924(Aline Silva de Miranda)https://orcid.org/0000-0002-9621-5422(Antonio Lucio Teixeira)
Date of submission:October 27, 2022
Date of decision:December 20, 2022
Date of acceptance:January 6, 2023
Date of web publication:January 30, 2023
https://doi.org/10.4103/1673-5374.368301
How to cite this article:de Miranda AS,Teixeira AL (2023) Renin-angiotensin system in the central nervous system: focus on Huntington’s disease.Neural Regen Res 18(10):2206-2207.
Open access statement:This is an open access journal, and articles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License,which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Open peer reviewer:Rocio Gomez-Pastor,University of Minnesota Neuroscience, USA.
Additional file:Open peer review report 1.
- 中国神经再生研究(英文版)的其它文章
- From static to dynamic: live observation of the support system after ischemic stroke by two photon-excited fluorescence laser-scanning microscopy
- MicroRNAs in mouse and rat models of experimental epilepsy and potential therapeutic targets
- The generation and properties of human cortical organoids as a disease model for malformations of cortical development
- Nanotechnology-based gene therapy as a credible tool in the treatment of Alzheimer’s disease
- Detection of Alzheimer’s disease onset using MRI and PET neuroimaging: longitudinal data analysis and machine learning
- A pancreatic player in dementia: pathological role for islet amyloid polypeptide accumulation in the brain