
Detection of Alzheimer’s disease onset using MRI and PET neuroimaging: longitudinal data analysis and machine learning
2023-03-23 08:13IroshanAberathneDonKulasiriSandhyaSamarasinghe
中国神经再生研究(英文版) 2023年10期
Iroshan Aberathne, Don Kulasiri,*, Sandhya Samarasinghe
AbstractThe scientists are dedicated to studying the detection of Alzheimer’s disease onset to find a cure, or at the very least, medication that can slow the progression of the disease.This article explores the effectiveness of longitudinal data analysis, artificial intelligence, and machine learning approaches based on magnetic resonance imaging and positron emission tomography neuroimaging modalities for progression estimation and the detection of Alzheimer’s disease onset.The significance of feature extraction in highly complex neuroimaging data, identification of vulnerable brain regions, and the determination of the threshold values for plaques, tangles, and neurodegeneration of these regions will extensively be evaluated.Developing automated methods to improve the aforementioned research areas would enable specialists to determine the progression of the disease and find the link between the biomarkers and more accurate detection of Alzheimer’s disease onset.
Key Words:deep learning; image processing; linear mixed effect model; neuroimaging; neuroimaging data sources; onset of Alzheimer’s disease detection; pattern recognition
Introduction
Alzheimer’s disease (AD) is a disorder which destroys the human brain and ultimately leads to dementia (Joubert et al., 2016; Ayodele et al., 2021).Alois Alzheimer, a German psychiatrist, diagnosed the first AD patient (51 years old) in 1906 (Ammar and Ayed, 2020).In the long term, due to the significant decline of her memory, the patient ultimately become totally dependent on caregivers, a fate shared by all AD patients (Feng et al., 2020; Popuri et al.,2020; Dashtipour et al., 2021; Huggins et al., 2021).
Globally, AD is the most common form of dementia, the percentages range from 50% to 75%.This figure is staggering when compared with other types of dementia, including vascular dementia (20–30%), Lewy Body disease(10–25%), and frontotemporal dementia (10–15%) (Joubert et al., 2016;Ayodele et al., 2021; Dashtipour et al., 2021; Gao, 2021).In 2019, there were 50 million individuals diagnosed with dementia.It has been estimated that by 2050 there will be 131.5 million sufferers.By 2030, the total, global financial cost of AD is expected to be US$2 trillion (Ammar and Ayed, 2020;Farina et al., 2020; Feng et al., 2020; Popuri et al., 2020; Shirbandi et al.,2021).By 2050 globally, it is estimated that the number of people suffering from dementia would be 130 million (Gao, 2021).This may have a positive association with the increasing rate of the elderly population worldwide and a negative relationship with the lack of proper medication or more accurate early detection techniques for AD.
Even though scientists have spent considerable amounts of time, money, and effort researching early AD diagnosis using a variety of methods, post-mortem examination is still considered to be the only definitive way to confirm a diagnosis (Houmani et al., 2018; Popuri et al., 2020; Sun et al., 2020; Huggins et al., 2021).Hence, there is a great need for more accurate diagnosis techniques that can be used in the early stages of AD.Identifying those at risk of AD as early as possible would have a significant and positive effect on disease control (Popuri et al., 2020; Ghazi et al., 2021).Nevertheless, early detection of AD is challenging as, aside from AD, most elderly people suffer from age-related pathologies.
It is well-known that structural and molecular level alterations in the brain related to AD begin years before any physically noticeable symptoms such as memory loss, issues with problem solving, and language difficulties appear(Hojjati et al., 2022).Using magnetic resonance image (MRI) and positron emission tomography (PET) neuroimaging technologies, these structural and molecular level changes and their patterns can be observed (Chandra et al.,2019; Sun et al., 2020; Bomasang-Layno and Bronsther, 2021; Ghazi et al., 2021;Shirbandi et al., 2021).Identifying novel and effective biomarkers for earlystage AD using neuroimaging modalities would provide informed treatment plans, reduce the severity of the symptoms and prevent complications, all of which would ultimately enhance the patient’s quality of life (Dashtipour et al.,2021; Jeremic et al., 2021; Qu et al., 2021; Shirbandi et al., 2021).
At present, sufferers are usually diagnosed by doctors in consultation with specialists such as neurologists and/or neuropsychologists.Diagnosis usually involves taking the patient’s medical history, conducting physical examinations,running diagnostic tests, performing neurological and neuroimaging examinations, and mini-mental state assessments.These manual methods are not only time-consuming, but also require expert knowledge.All these manual methods rely on visual inspection or semi-quantitative approaches which totally depend on the examiner/reader expertise; however, that might lead to inter-reader disagreement, but if computer-aided diagnosis systems are used to identify the underlying neurological causes of brain disorders,more accurate and precise diagnosis can be performed at the early stage of the disease continuum (Farina et al., 2020; Feng et al., 2020; Tanveer et al.,2020; Huggins et al., 2021; Hazarika et al., 2022).
This review focuses on the detection of AD onset using neuroimaging data and artificial intelligence (AI), machine learning (ML), and longitudinal data analysis.Our main objective is to review biomarkers, detection techniques,and current research gaps in the early detection of AD.
Search Strategy
In the present review, we searched papers from Google Scholar (https://scholar.google.com/) and ScienceDirect (https://www.sciencedirect.com/)and included full-text papers published between 2013 and 2022.To ensure relevant results were retrieved, we focused on finding certain keywords followed by Alzheimer’s disease in the title, abstract, or keywords, such as“early detection”,“early and late onset”,“biomarkers”,“detection techniques”,“neuroimaging”,“MRI and PET”,“amyloid-beta and Tau”,“artificial intelligence and machine learning”,“statistical modelling”.We included research papers that were aligned with the following inclusion criteria: studies that mainly focused on the application of AI, ML, and statistical modeling in the early detection of AD, with structural and molecular level biomarkers extracted from MRI and PET neuroimaging modalities.As shown in Figure 1, after applying the duplicate removal, screening, and inclusion criteria, the original number of 348 studies was reduced to 84.

Figure 1|Search strategy and study selection process.
Onset of Alzheimer’s Disease and Disease Continuum
The progression of AD with brain changes which are unnoticeable to memory deficits and eventual physical disability occurs as a result of the deposition of amyloid-beta (Aβ) and hyperphosphorylated tau.Aβ and tau are aggregated to form plaques and neurofibrillary tangles which have a great positive effect on structural neurodegenerative changes and even cell deaths in the brain (Iddi et al., 2019; Farina et al., 2020; Huggins et al., 2021; Jeremic et al., 2021; Shirbandi et al., 2021).Two forms of AD onset have been defined based on the age because age is the key risk factor for AD: Early-onset AD(EOAD) defined as AD with clinical onset occurring in the patients younger than 65 years; late-onset AD (LAOD) defined as the patients older than 65 years.EOAD sufferers constitute 5% to 6% of all AD patients (Mendez et al.,2019; Graff-Radford et al., 2021).However, the heritability of EOAD (between 92–100%) is higher than that of LOAD (70–80%) (Ayodele et al., 2021).Generally, EOAD patients present with non-amnestic syndromes, including impaired language, attention, and visuospatial functions.In contrast, patients with LOAD often present with memory deficits (Gumus et al., 2021).Some of the characteristics associated with various brain regions are shown in Table 1.The underlying neuropathology is still unclear for either type of onset, it is thus necessary to conduct an in-depth investigation of these characteristics in relation to AD and identify the associated brain regions as some of these characteristics are common to other brain diseases as well (Koedam et al.,2010; Joubert et al., 2016; Tellechea et al., 2018; Mendez, 2019; Ayodele et al., 2021; Contador et al., 2021).

Table 1 |Characteristics of early- and late-onset AD where different patterns of atrophy and molecular changes can be observed over time
Although some of the characteristics listed in Table 1 are common to other brain diseases, distinct patterns of plaques and tangle depositions, atrophy of the brain, and changes in molecular level metabolism can be observed on the MRI and PET scans of AD patients.In other words, MRI and PET images can be used as more advanced and informative modalities to diagnose AD and identify specific characteristics associated with AD (Mele et al., 2019;Mendez, 2019; Popuri et al., 2020; Graff-Radford et al., 2021).Regardless of whether AD is early or late onset, the disease continuum can be divided into three stages: preclinical, mild cognitive impairment (MCI), and dementia(Zhang et al., 2017; Houmani et al., 2018; Sun et al., 2020; Huggins et al.,2021).However, the length of each stage of the continuum is subject to age,genetics, gender, and various other factors (Zhang et al., 2017; Zhao et al.,2021).
Although in the preclinical stage the patients do not show any obvious symptoms, such as memory loss, there are measurable indicators in the brain, e.g., cerebral amyloidosis (Zhang et al., 2017; Houmani et al., 2018).The next stage of AD, MCI is considered a transitional stage between healthy aging and AD subjects (Sun et al., 2020; El-Sappagh et al., 2021; Huggins et al., 2021).At this stage, the patients experience some memory impairments due to the affected medial temporal lobe.Meanwhile the lateral temporal and parietal lobes are also at a great risk.However, the patients can continue daily activities (Houmani et al., 2018; Sun et al., 2020).These patients have been identified as one of the subtypes of MCI called amnestic MCI who characterized by memory loss; all other cognitive impairments can be observed in those with non-amnestic MCI (Joubert et al., 2016; Farina et al.,2020).In this stage, patients might be able to revert to‘normal’, due to family intervention: family members are often able to identify common symptoms,such as the sufferer having problems remembering names, recent events,conversations with others, and a disjointed flow of communication.In such situations, doctors may recommend adopting precautionary measures to halt disease progress (Jeremic et al., 2021; Zhao et al., 2021; Hazarika et al., 2022).Clinic-based studies have shown that 4–15% of individuals displaying MCI revert to a normal state; the figure is even higher in population-based studies,with 29–55% reverting to a normal state (Feng et al., 2020).However, both types of patients have a greater risk of becoming AD patients in the future:32% of MCI patients are diagnosed with AD within the next 5 years (Houmani et al., 2018; Farina et al., 2020; Zhao et al., 2021).As indicated above, in the final stage of AD, there are notable reductions in hippocampal volume and/or changes in cortical thickness.The frontal and occipital lobes are also damaged.In this stage, patients are totally dependent upon caregivers due to significant declines in cognitive and motor functions (Houmani et al., 2018;Sun et al., 2020; Zhao et al., 2021).The aforementioned findings suggest that different brain regions play key roles in AD diagnosis at different stages of AD but less information is available for the preclinical stage.Feng et al.(2019)have found some potential brain regions which have the greatest impact on AD and MCI.They have focused on MCI with two subgroups: progressive and stable MCI.According to the findings, the top 10 brain regions are right uncus, right superior frontal gyrus, left parahippocampal gyrus, right superior temporal gyrus, right hippocampal formation, right subthalamic nucleus, right thalamus, left middle frontal gyrus, left precuneus, and left inferior temporal gyrus (Figure 2).
Neuroimaging Biomarkers and Alzheimer’s Disease
Neuroimaging techniques such as electroencephalography (EEG),magnetoencephalography (MEG), MRI, and PET enable researchers to gather quantitative data on the central nervous system (Houmani et al., 2018; Kamathe and Joshi, 2018; Huggins et al., 2021).These modalities are capable of capturing functional, structural, and molecular level information in the brain (Mele et al., 2019; Popuri et al., 2020).Neuroimaging techniques have extensively been used in a variety of ways to formulate biomarkers associated with AD.The level of complexity of EEG and magnetoencephalography signals of the brain is used as one of the potential biomarkers for the identification of early detection of AD regardless of their inherent non-linear, non-stationary, and noisy nature.These signals record the brain’s electrical activities in the order of milliseconds with quantitative features such as epoch-based entropy (i.e., sample entropy, Tsallis entropy, approximate entropy, multi-scale entropy, and Lempel-Ziv complexity);a measure of signal complexity and bump modeling; a model of synchrony.To measure the synchrony of EEG, correlation coefficient, coherence, Granger causality, phase synchrony, state-space-based synchrony, stochastic event synchrony, and mutual information can be used.All these methods enable them to determine potential pathways for disease diagnosis (Houmani et al., 2018;Mele et al., 2019; Huggins et al., 2021).
Volumetric biomarkers with MRI

Figure 2|Potential brain regions which have the greatest impact on AD (top row), pMCI (middle row), and sMCI (bottom row).
MRI is both a cost-effective and non-invasive (due to the lack of ionizing radiation) high-quality neuroimaging technique.Information on structural properties using structural MRI (sMRI; e.g., cortical thickness and loss of braintissues) and functional properties via functional MRI (e.g., blood flow to the brain and low-frequency endogenous oscillations in hundreds of cortical areas and major subcortical nuclei in the brain) can be gathered using MRI, which are considered key biomarkers of AD because neuron death causes overall shrinkage of the brain over time.Specifically, cerebral white matter and gray matter tissue indicate possible atrophy of the brain (Papo et al., 2014; Islam and Zhang, 2017; Kamathe and Joshi, 2018; Iddi et al., 2019; Mele et al.,2019; Farina et al., 2020; Ayodele et al., 2021; Piersson et al., 2021; Zhao et al., 2021).In the brain, the hippocampus manages episodic and spatial memory.It functions as a relay structure between an individual’s body and brain.AD causes the hippocampus and cerebral cortex of the brain to shrink and leads to enlarged ventricles (Figure 3).In healthy individuals, the average rate of hippocampus reduction is 0.24–1.73%; in AD patients, the rate of shrinkage is much higher (2.2–5.9% per year; Islam and Zhang, 2017).It has been found that the overall size/area of the hippocampus and gray matter of patients aged 60–69 years is larger than that in any other group (i.e., 70+years old)(Hazarika et al., 2022).Shrinkage of the hippocampus has a negative effect on synapses and neuron ends, suggesting that an individual’s short-term memory,thinking, planning, and judgment are badly affected (Islam and Zhang, 2017).As shown in Figures 4 and 5, hippocampal atrophy, ventricular expansion and precuneus atrophy have different patterns at different stages of AD (Mӧller et al., 2013; Mofrad et al., 2021).Both studies show that hippocampus atrophy,while ventricle enlargement has non-linear positive and precuneus atrophy,negatively correlates with age.
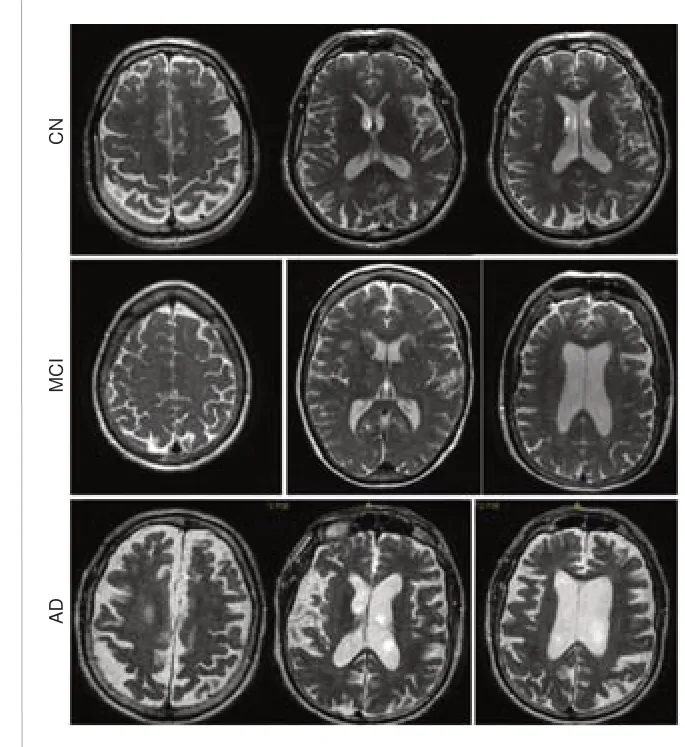
Figure 3|Ventricle enlargement and hippocampus changes can be observed at different stages of AD via MRI images.
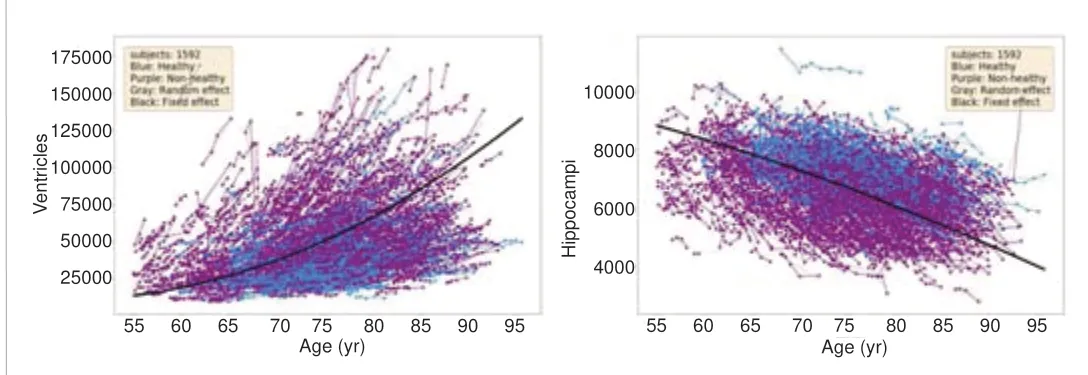
Figure 4|The correlation of volume trajectories of the ventricles and hippocampus of the left hemisphere with age.
Molecular Biomarkers with PET

Figure 5|The atrophy of the hippocampus (left) and precuneus (right) with age.
PET imaging measures the metabolism of glucose in the brain.Hypometabolism, a decline in metabolic activity in the brain, can be easily measured using a PET scan; it can provide complementary information, which can be used alongside MRI images (Zhang et al., 2017; Tanveer et al., 2020;Zhao et al., 2021).PET scans can be used to detect the onset of AD by utilizing different types of radiotracers prior to taking other types of neuroimages.This technique has a higher sensitivity since it reveals the molecular level changes prior to the onset of structural changes in brain regions even in the preclinical stage of AD; therefore, it can be used to map the distribution of tangles and plaques because these molecular level changes have distinctive stage-specific effects on the global coupling between the structural and functional brain networks associated with AD (Zhang et al., 2017, 2021; Duffy et al., 2019; Li et al., 2022).The density of amyloid-beta and tau in the brain can be determined using18F-AV45 and18F-AV1451 PET images respectively (Ferri et al., 2021;Ghazi et al., 2021; Qu et al., 2021).
Some of the volumetric and molecular level biomarkers and their association with AD progression, and the significance of the various neuroimaging modalities in identifying AD are shown in Table 2.However, these associated features can be used to formulate novel composite biomarkers which might be specific to AD (DeTure and Dickson, 2019; Ghazi et al., 2021; Hojjati et al.,2022).
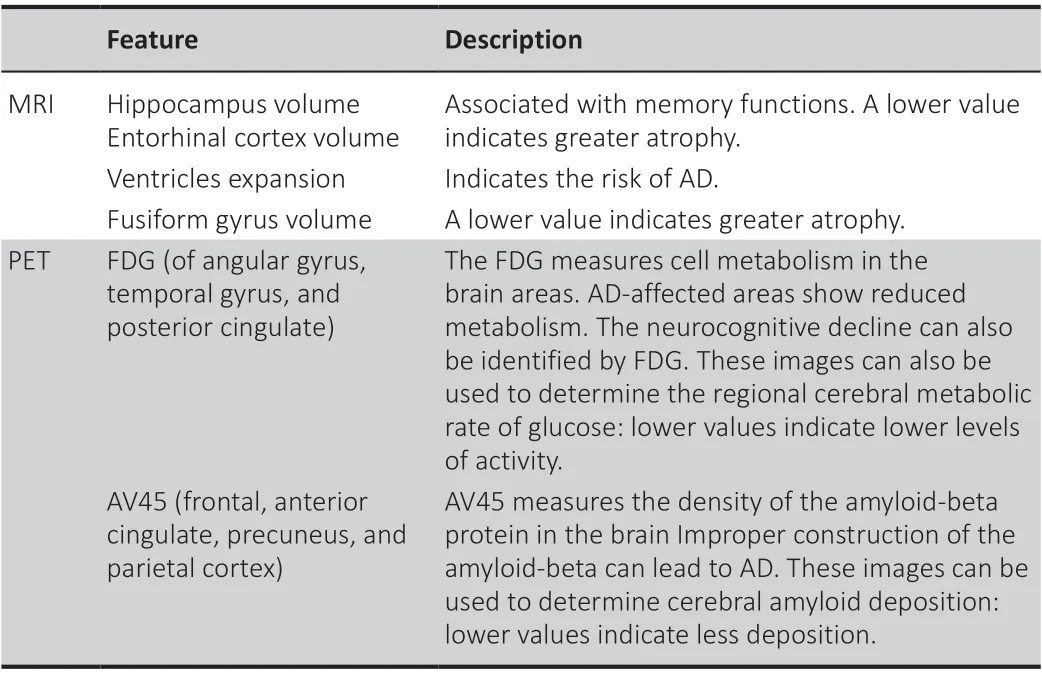
Table 2 |Biomarkers identified on MRI and PET images and their association with AD
Datasets
Reliable data are needed to correctly diagnose AD.The following databases are currently available: Australian Imaging, Biomarkers and Lifestyle (AIBL)database, the National Alzheimer’s Coordinating Center (NACC) database, and the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (Burnham et al., 2021; Feng et al., 2020; Mofrad et al., 2021).The AIBL database is associated with two study centers located in Melbourne and Perth (Burnham et al., 2021).The study is composed of more than 1000 participants, all of whom are 60 years or older, and includes healthy volunteers and MCI and AD patients.The NACC has developed and maintains a large relational database of standardized clinical and neuropathological research data.The database contains measurements from MRI and PET scans,and various cognitive tests.NACC data is available to researchers for free(Burnham et al., 2021; Mofrad et al., 2021).
The ADNI was established in 2003 as a multicenter longitudinal study.The primary goal of ADNI is to develop a list of disease biomarkers and advance understanding related to AD pathophysiology.The ADNI has been used to test whether serial MRI, PET, other biological markers, and clinical and neuropsychological assessments can be combined to measure the progression of MCI and early AD (Feng et al., 2020; Martí-Juan et al., 2020; Mofrad et al.,2021; Sethi et al., 2022).The study has been splitted into three sub-initiatives:ADNI1, ADNI2, and ADNI GO.The initial phase, known as ADNI1, included subjects at 50–90 years of age, from approximately 50 sites across the United States and Canada.ADNI2 and ADNI GO added new participants and received new sources of funding.The database is available to researchers worldwide and enriched with different modalities and long follow-up period (Martí-Juan et al., 2020), and has a broad range of collaborators (Feng et al., 2020;Martí-Juan et al., 2020).The data is well-organized and has been processed.JADNI, a new publicly available database, includes clinical Alzheimer data from longitudinal studies conducted in Japan (Tanveer et al., 2020).Table 3 explains the significance and the highly versatile nature of these data sources in the context of AD detection, progression estimation, and classification.2021).Thus, the longitudinal data analysis approach with neuroimaging has greater potential even though it has received less attention in terms of the early detection of AD (Martí-Juan et al., 2020).One such study, conducted by Martí-Juan et al.(2020), grouped the research which uses longitudinal data into two broad categories based on the follow-up period; 1) short-term longitudinal works, including follow-ups to a maximum of 2 years, 2) longterm longitudinal works, including follow-ups of 3 years or more.The authors concluded that there is a lack of research on computer-aided diagnosis using long-term longitudinal data.
The linear mixed effect model (LME), a well-established approach to longitudinal data analysis, enables relatively simple, robust, noise-free, and subject-specific representations of brain changes over time based on age.LME can be used to provide a combination of fixed and random effects as predictor variables.While the fixed effects represent the cohort-level variation, the random effects are dedicated to that at the subject level.As it represents the subject and cohort-level longitudinal trajectories in terms of parameters (i.e., the intercept and slope), dependency on each data point can be avoided, enabling noise-free measurements (Maruotti, 2011;Mofrad et al., 2021).Mofrad et al.(2021) used longitudinal brain MRI data from subjects scanned at least twice over a 15-year period.The dataset was obtained from ADNI and AIBL sources.LME was used to extract the features from the longitudinal MRI examinations in terms of region of interest (ROI)s.Their mixed effect model represents the volumetric measurements (Volijr)of each ROI (r) in multiple scans (j) for each individual (i) with respect to the linear and non-linear relationship of age (Volijr= β0r+ β1rAgeij+ β2rAgeij2+ b0ir
Detection Techniques
Longitudinal data analysis
Longitudinal data facilitates the measurement of within-sample changes over time: this technique enables scientists to measure the duration of various events and record the timing of them (Martí-Juan et al., 2020; Mofrad et al.,There are a wide range of physical and neurobiological exams designed to detect AD and determine the advance of AD; these tests assess verbal and visual episodic memory, attention, executive functions, visuospatial skills,and language (Joubert et al., 2016; Tanveer et al., 2020).These tests include the Clinical Dementia Rating Sum of Boxes (CDRSB), the Alzheimer’s Disease Assessment Scale Cognitive 13-item cognitive subscale (ADAS13), the Rey Auditory Verbal Learning Test, the Mini-Mental State Examination, the Clinical Dementia Rating (CDR), the Oktem Verbal Memory Processes Test, the Wechsler Memory Scale-Revised, the Digit Span Test, the Verbal Fluency Test(semantic), and the Boston Naming Test (Islam and Zhang, 2017; Farina et al.,2020; Ghazi et al., 2021; Zhao et al., 2021; Hojjati et al., 2022).Clinicians also take a detailed patient history.Along with Mini-Mental State Examination and CDR methods, clinicians use a simple questionnaire approach to assess an individual’s cognitive ability (Zhao et al., 2021).+ b1irAgeij+ b2irAgeij2+ εijr).These features were fed into ensemble machine learning models which performed a multi-class classification task (i.e., CNvs.MCIvs.AD) designed to detect AD prior to the clinical events.This method used measurements of the hippocampal and lateral ventricle volumes in a single subject and examined the differences over time.This technique had prediction accuracies of 73% and 78% for CN to MCI and MCI to AD,respectively.These results are significant because they indicated disease prior to clinical diagnosis.
Hojjati et al.(2022) quantitatively analyzed AD progression utilizing longitudinal sMRI and PET neuroimaging data with a feed forward multilayer perceptron.They experimented with unimodal (i.e., sMRI or PET data)and bimodal neuroimaging data to predict CDRSB and ADAS13 scores.CDRSB refers to the global clinical measure for six cognitive areas (i.e., memory,orientation, judgment, community affairs, home and hobbies, and personal cares).ADAS13 is a measurement tool which clinicians use to examine multiple cognitive domains including memory, language, praxis, orientation,executive functioning, and functional abilities.The results showed that sMRI features such as the entorhinal cortex and the hippocampus with PET features, including FDG-PET of the angular gyrus, temporal gyrus, and posterior cingulate, outperform other neuroimaging features in predicting ADAS13 and CDRSB scores.This study revealed an association between neuropsychological scores and sMRI and FDG-PET biomarkers, ranging fromnormal aging to severe AD.Even though these findings demonstrate the significance of the longitudinal data modeling in AD detection and the field of onset AD detection, there are few studies examining longitudinal modeling with neuroimaging data.Moreover, this technique can be incorporated with the aforementioned vulnerable brain regions identification rather than depending on conventional ROI to perform the detection of AD onset with the help of AI and ML approaches.
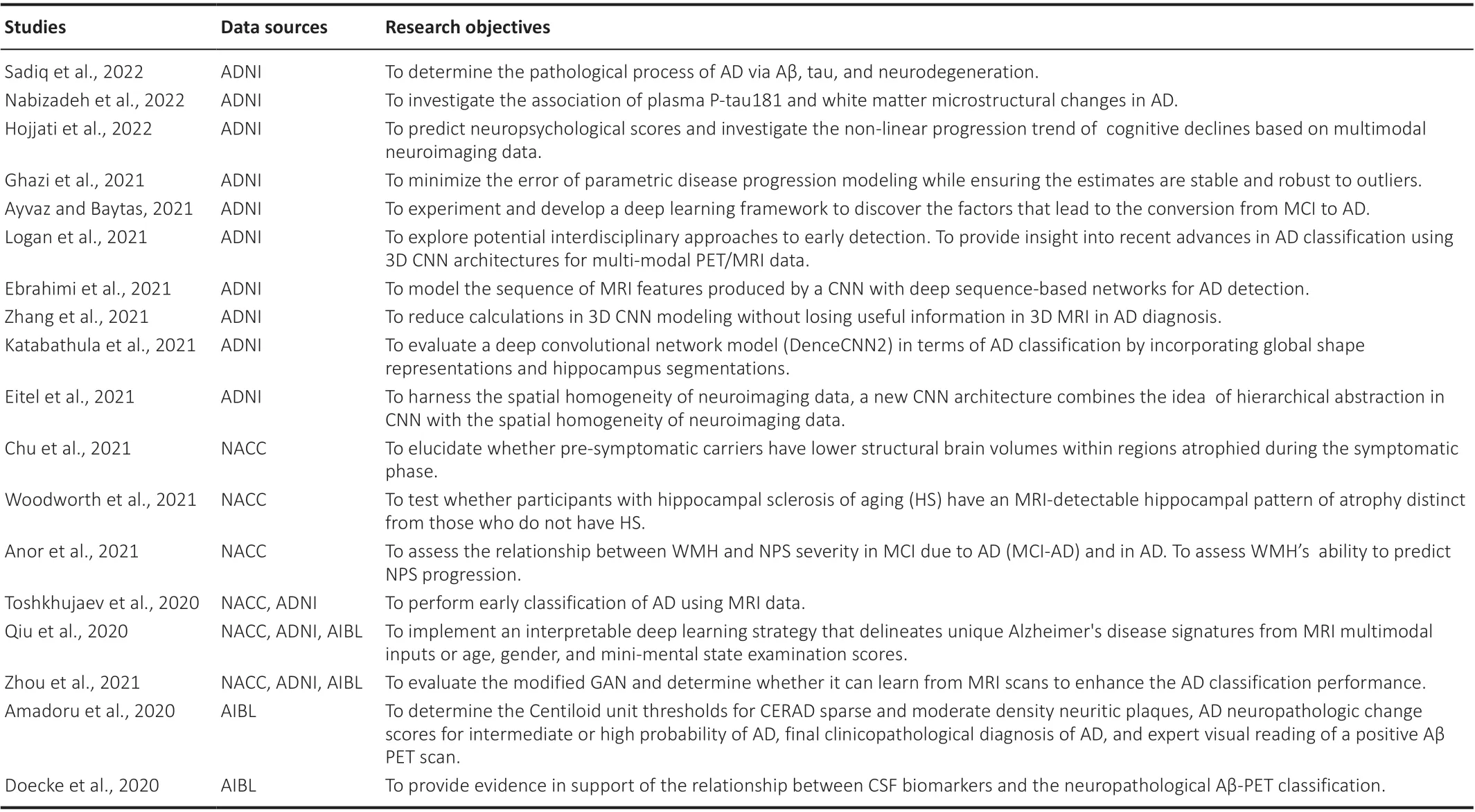
Table 3| Recent research studies which use ADNI, AIBL, and NACC data
Artificial intelligence and machine learning
Neuroimaging modalities with AI and ML techniques demonstrate a greater ability to identify AD and its stages more accurately rather than traditional neuropsychological tests (Ghazi et al., 2021; Hojjati et al., 2022).Hence, over the last few years, scholars have developed a number of techniques and tools to detect AD, often using AI and ML approaches (Tanveer et al., 2020;Arabi et al., 2021; Mofrad et al., 2021).Especially in AI-driven medical image analysis, between 1975 and 2015, there was an average of approximately 300 published papers in this field but in just 5 years (2015 to 2020), the figure had doubled, to approximately 600 (Mӧhle et al., 2021).Support vector machine (SVM), convolutional neural network (CNN), and deep learning(DL) models are the most widely used AI classification techniques for AD detection and diagnosis (Tanveer et al., 2020).In terms of data analysis,prediction, forecasting, and classification tasks, DL has gained popularity over conventional statistical analysis methods.The popularity of DL is due to the advancement of complex algorithms, automatic feature identification, and its high processing abilities (Cheng et al., 2016; Tanveer et al., 2020; Huggins et al., 2021; Zhao et al., 2021).
The use of AI and DL in biomedical engineering applications has demonstrated potential in the classification, segmentation, and detection of several diseases and pathologies, particularly those found in the brain, lungs,and retina (Islam and Zhang, 2017; Mӧhle et al., 2021).Scientists have investigated the applicability of AI, ML, and DL approaches using different kinds of model implementation, feature engineering/selection techniques,and hyperparameter optimization.MRI and PET data have been used, both individually and collectively, to solve binary class, ternary class, and even multi-class classification problems (Islam and Zhang, 2017; Kamathe and Joshi, 2018; Dashtipour et al., 2021; Raju et al., 2021; Hazarika et al., 2022).
Kamanthe et al.(2018) used an SVM with MRI brain images collected from CN and MCI patients to segment brain tissue into three different classes called CSF, WM, and gray matter with the intention of early detection of AD based on brain atrophy.They observed that the best-performing model is polynomial kernel SVM for tissue segmentation with the band expansion process and independent component analysis (ICA).Dashtipour et al.(2021) also used MRI images but with a range of ML and DL algorithms such as logistic regression, decision trees, random forest, SVM, multi-layer perceptron,k-nearest neighbors, Naive Bayes, CNN, and bidirectional long short-term memory to detect five types of categories (i.e., normal, very mild dementia,mild dementia, moderate dementia, and severe dementia).Upon the study results, the best-performing model was bidirectional long short-term memory with the accuracy rate of 91.28%.A similar study has been conducted by Islam and Zhang (2017) for detecting four categories: non-demented, very mild, mild, and moderated, and they reached the accuracy rate of 73.7%.The significance of this approach is that it demonstrated the application of data augmentation with CNN is one of the inherent limitations of this research field.Transfer learning is one of such approaches to working with very little data and data augmentation (Tanveer et al., 2020).The combination of CNN and TL has given better results to Puente-Castro et al.(2020) in their study with sagittal MRI images.They used SVM for feature extraction and enhanced the data set with TL.Finally, they were able to achieve accuracy, precision,recall, specificity, and f1 scores of 78.64%, 68.87%, 58.27%, 80.06%, and 60.30%, respectively.Another interesting result can be found in the study by Feng et al.(2020) where researchers have employed multi-dimensional CNNs(2D-CNN and 3D-CNN) and 3D-CNN-SVM, along with MRI data, to conduct binary and ternary AD disease classification.The experiment demonstrated the potential to capture 3D MRI images of the amygdala, temporal lobe, and parahippocampal regions, all of which are known to be affected by AD.
A key limitation of the research on the detection of AD onset (i.e., CNvs.MCI)relates to the performance of the current AI and ML models.Most of the previous binary class classification models pay little attention to the specificity even though this matrix is a key performance measure in the detection of AD onset; specificity provides a numerical figure which can be used to evaluate the model’s ability to correctly identify subjects who do not have the disease.Some of the recent research studies to support this fact are shown in Table 4.While the accuracy and sensitivity scores of the models are above 95%, the highest specificity rate is considerably lower (87.0%).
It has been shown that measurable changes in PET and MRI biomarkers occur some years before the onset of clinical symptoms.However, most of the studies have focused on individual biomarkers rather than considering combining contributions to the disease diagnosis (Sadiq et al., 2022).Therefore, a combination of MRI and PET modalities would not only help clinicians to qualitatively diagnose AD but would also enable them to determine the threshold between the normal phase and the onset of AD(Ferré-González et al., 2021).The performance measures in Table 4 for MRI and PET image modalities have shown more consistent performance than that of individual image modality, which indicates that the composite modalities have better potential in the detection of AD onset.

Table 4 |Performance of the different ML approaches in CN vs.MCI classification
Future Directions on Onset of Alzheimer’s Disease Detection
Although over the past decade, scientists have made numerous discoveries relating to the onset of AD, there are still unique and specific areas that need to be explored.Only a few studies focus directly on the onset of AD (Joubert et al., 2016; Ayodele et al., 2021; Carpanini et al., 2021; Kim et al., 2021).Joubert et al.(2016) used statistical analysis, along with neuropsychological assessments, and MRI and PET data to investigate memory breakdown patterns in patients with EOAD and LOAD.The study results showed that EOAD and LOAD patients display distinct patterns in the memory domain,the cognitive domain, executive functions, and visuoconstructional abilities.Kim et al.(2021) evaluated risk factors such as the apolipoprotein E ε4, low education, and vascular risk on cognitive trajectories, with respect to EOAD and LOAD, to determine whether there are any notable differences between the two.The results indicated that the risk factors have a positive relationship with LOAD, but a negative relationship with EOAD.Although both EOAD and LOAD share the same pathological characteristics, the cognitive decline is faster in EOAD.Though the most common cause of dementia is LOAD, its molecular basis is not yet fully understood.
Carpanini et al.(2021) studied the impact of complementary genes and the risk of LOAD.While the study results confirmed the link between the CLU and CR1 genes with LOAD, there was no significant association for the complementary gene set when CLU and CR1 were excluded.Moreover,they found no association with other complementary genes, C1S included.Ayodele et al.(2021) conducted a systematic review and demonstrated the importance of understanding the etiology of EOAD.The authors proved that only a fraction of the biomarker and neuropathological variations of AD onset have been identified.Using MRI data, a longitudinal study by Contador et al.(2021) investigated EOAD.They observed progressive atrophy in several brain regions, including the posterior cortices, the hippocampus, and the amygdala.Although it is quite normal for the brain to show some signs of atrophy as individual ages, in dementia, in some regions of the brain, the rate of atrophy is faster.Thus, another aspect of AD research should focus on identifying the particular parts of the brain that are affected at the early stage: determining these biomarkers would aid the early detection of AD.Distinctions between neurodegenerative changes as a result of normal aging and those associated with AD need to be explored further, as it is very difficult to differentiate between cognitive decline related to MCI symptoms and those associated with CN (Mofrad et al., 2021).It is vital to identify novel biomarkers so that clinicians can confidently distinguish between MCI and CN (Li et al.,2021).Distinguishing between CN and MCI is even more critical when using traditional image classifiers because neuroimaging features are very similar to both categories in older age groups.Therefore, advanced and effective feature engineering, the hyperparameter tuning approaches of AI and ML models, and novel classifiers are needed to enhance the classification task of the onset of AD (Feng et al., 2020; Zhang et al., 2021).
It is obvious that all these AI, ML, and statistical models are data-driven.Hence data preprocessing and feature extraction play a vital role irrespective of the classification model types.However, we found that most of the studies based on neuroimaging data use the features extracted from thirdparty software for model training and testing processes.We suspect this could be one of the reasons for model performance.The level of accuracy of these software is debatable because the different versions of these software produce different features for the same modalities (Chepkoech et al., 2016;Mofrad et al., 2021).In addition, it has been identified that some of these software are able to neither capture the variability in atomic features nor define boundaries of some key brain regions accurately.The reliability of absolute volume measurement in ROIs, such as total intracranial, white matter, ventricular, gray matter, and cortical thickness are lower (Wisse et al., 2014, 2021; Chepkoech et al., 2016; Bigler et al., 2020; Hedges et al.,2022).Therefore, research focuses on novel/advanced data preprocessing and feature extraction aspects of neuroimaging data are vital to reduce the uncertainty of the AI and ML models so that quantitative and indicative biomarkers such as vulnerable brain region identification, calculation of brain atrophy, tau and tangle deposition can be improved.
Summary and Concluding Remarks
This review has outlined the context and explained various applications of longitudinal data analysis, in terms of the use of AI and ML in the detection of AD onset.The review has identified significant research gaps and suggested future research directions.Future research should concentrate on identifying advanced neuroimaging biomarkers using novel neuroimaging data preprocessing techniques, and AI and ML model implementation to identify vulnerable brain regions and estimate threshold values for key biomarkers.Advanced/novel AI and ML techniques, along with mathematical and statistical approaches, could be used to facilitate greater use of computationally inexpensive, robust, and reliable models which could detect either form of AD onset.To be effective, such techniques require greater specificity.
Author contributions:Conceptualization, methodology, and writing: IA;review and editing: DK, SS; supervision: DK, SS.All authors have read and agreed to the published version of the manuscript.
Conflicts of interest:The authors declare no conflicts of interest.
Data availability statement:No additional data are available.
Open access statement:This is an open access journal, andarticles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
- 中国神经再生研究(英文版)的其它文章
- From static to dynamic: live observation of the support system after ischemic stroke by two photon-excited fluorescence laser-scanning microscopy
- MicroRNAs in mouse and rat models of experimental epilepsy and potential therapeutic targets
- The generation and properties of human cortical organoids as a disease model for malformations of cortical development
- Nanotechnology-based gene therapy as a credible tool in the treatment of Alzheimer’s disease
- A pancreatic player in dementia: pathological role for islet amyloid polypeptide accumulation in the brain
- The role of fibronectin in multiple sclerosis and the effect of drug delivery across the blood-brain barrier