经皮冠状动脉介入相关止血技术的文献学分析
2022-06-22 23:25:28胡伟珍陈婵婵薛琴丹单培仁
中国现代医生 2022年12期
胡伟珍 陈婵婵 薛琴丹 单培仁
[摘要] 目的 通过对经皮冠脉介入止血技术的系统性研究来指导国内相关技术的发展。 方法 使用检索式(percutaneous coronary intervention)AND (hemostasis)对Web of science、Scopus和Pubmed数据库1993年1月至2020年12月期间的经皮冠脉介入围术期止血技术相关文献进行检索和分析。 结果 美国在该领域优势较大,研究机构中心性较低。研究热点包括血管造影术、经皮冠脉介入、人工压迫和止血器等。近年来研究主要关注比较穿刺位点(股动脉 vs. 桡动脉)和止血方式(压迫 vs. 封闭器)的预后。 结论 止血器能够减少出血并发症,改善患者预后。我国研究参与度较低,应开展以护理为主导的多学科研究。
[关键词] 经皮冠状动脉介入;桡动脉;文献学分析;止血装置;并发症
[中图分类号] R195.4 [文献标识码] B [文章编号] 1673-9701(2022)12-0104-03
[Abstract] Objective To guide the development of related technologies in China through systematic research on hemostasis technique during percutaneous coronary intervention. Methods The literature on perioperative hemostasis during percutaneous coronary intervention from January 1993 to December 2020 in the databases of Web of science, Scopus and Pubmed was searched and analyzed by using the search form (percutaneous coronary intervention) and (hemostasis). Results The United States exhibited great advantages in this field,while the research institutions were less centralized.Research hotspots included angiography, percutaneous coronary intervention, artificial compression and hemostat. In recent years, research focused on comparing the prognosis of puncture site (femoral artery vs. radial artery) and hemostasis mode (compression vs. obturator). Conclusion Hemostat can reduce bleeding complications and improve the prognosis of patients. There is relatively little research in this area in China and nursing-based multidisciplinary research should be undertaken.
[Key words] Percutaneous coronary intervention; Radial artery; Bibliometric analysis; Hemostatic device; Complication
近年来冠状动脉粥样硬化性心脏病(atherosclerotic coronary artery disease,CAD)患者群体年轻化[1],经皮冠脉介入治疗(percutaneous coronary intervention,PCI)显著增长[2]。PCI具有侵入性小和住院时间短的优势[3],而出血是围术期的常见并发症[4]。传统止血方法是人工压迫,耗时且占用护理资源[5]。此外,服用抗栓药物患者的人工压迫不足以有效止血,导致住院延长和费用增加[6]。止血器具有定位准确、压力可控等优势[7]。本研究通过对止血技术文献学分析,了解相关热点,指导国内研究的开展。
1 资料与方法
1.1 文献检索
构建检索式(percutaneous coronary intervention)AND(hemostasis),对Web of science、Scopus和Pubmed数据库1993年1月至2020年12月的经皮冠状动脉介入围术期止血技术相关文献进行检索,获得论著、综述、会议记录等464篇。
1.2 文献类别筛选
阅读文献摘要,排除会议记要和信件等34篇,使用EndNote X7删除33篇重复收录文献,最终纳入论著和综述共397篇。
1.3 研究对象处理及分析方法
将文献导入Citespace 5.5.R1,提取研究机构、国家、主题词等信息构建关联网络,使用Log-likelihood rate(LLR)算法進行聚类分析,并提取突显词做词频分析。
2 结果
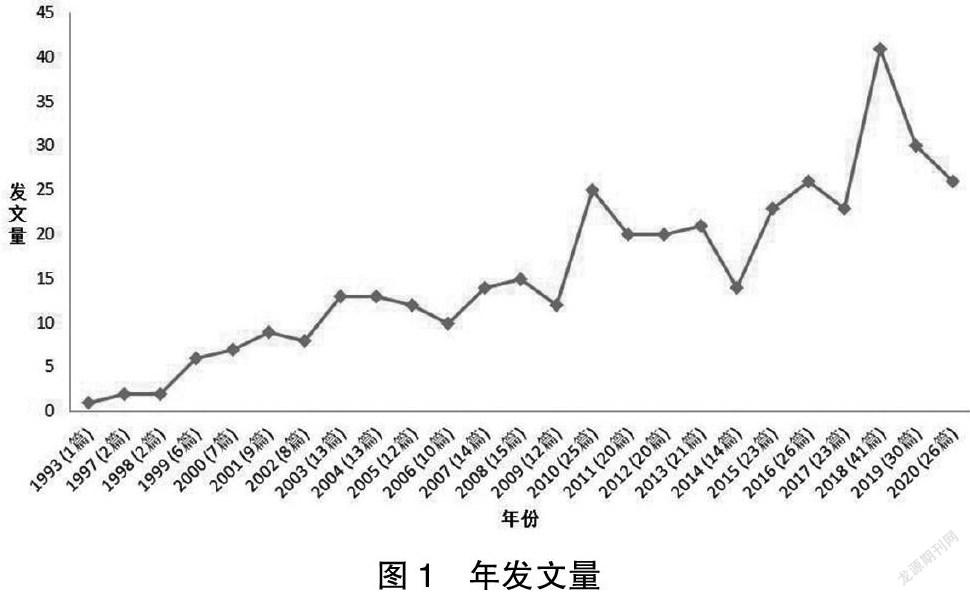
相关研究始于二十世纪末,发文量呈逐渐增多。见图1。
2.1 作者
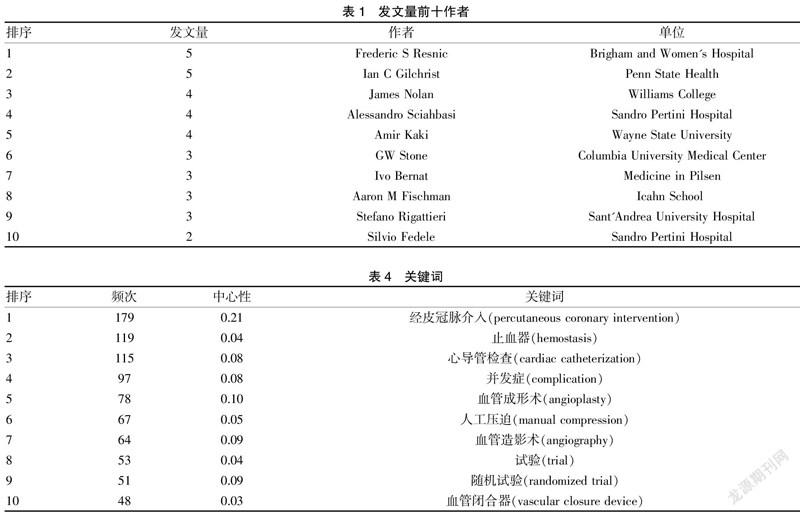
发文量前十位研究员共发表36篇文献(9.1%)。见表1。
2.2 研究机构
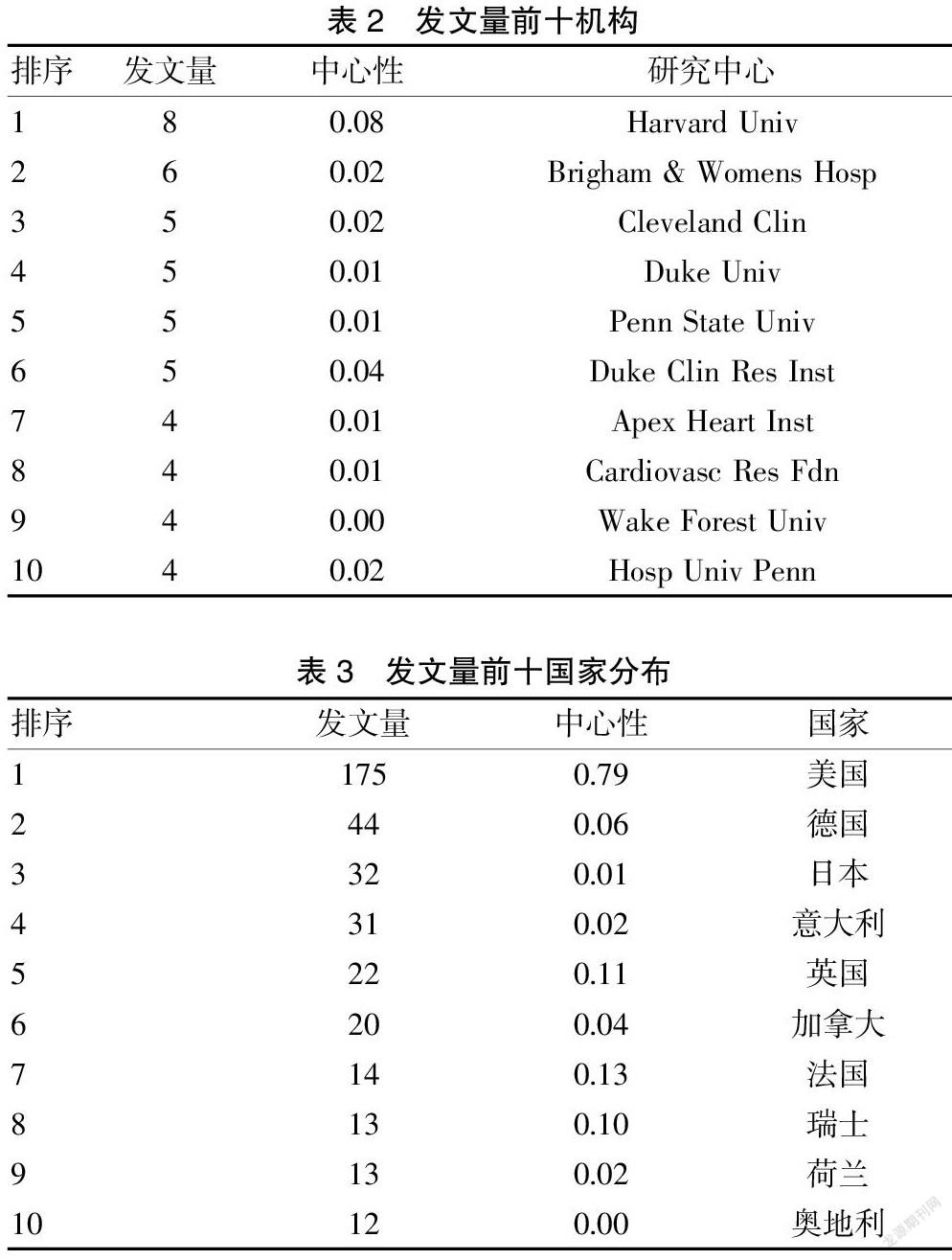
发文量前十位研究机构共发表50篇文献(12.6%),中心性较低。见表2。
2.3 国家
美国在该领域优势较大,发表文献175篇(44.1%)。见表3。
2.4 关键词
热点关键词包括经皮冠脉介入(percutaneous coronary intervention)、止血器(hemostasis)、心导管检查(cardiac catheterization)、并发症(complication)、血管成形术(angioplasty)、人工压迫(manual compression)、血管造影术(angiography)、试验(trial)、随机试验(randomized trial)、血管闭合器(vascular closure device)。见表4、封三图3。
2.5 聚类分析
LLR聚类[8]生成8个群组包括口服抗凝剂(direct oral anticoagulants)、经桡动脉(transradial)、穿刺部位(puncture site)、冠脉成形术(coronary angioplasty)、血小板功能分析仪(pfa-100)、大内皮素(big endothelin)、抗血小板药(antiplatelet drug)和血小板微泡(platelet microvesicles)。见封三图4、封三图5。
2.6 研究趋势
突显词分析[9]显示研究呈周期性发展,由手术术式向止血器械转变。二十世纪末和2000年后分别围绕冠脉成形术(coronary angioplasty)、冠脉介入(coro-nary intervention)向封闭器(closure device)和閉合器(suture mediated closure)转变。见封三图6。
3 讨论
3.1 研究历程
止血技术研究始于二十世纪末,美国发文数量和质量均处于领先地位[10]。科研机构中心性低提示核心团队未形成。我国研究参与度低,应重视和加强该领域的研究。
3.2 研究重点
3.2.1 出血并发症 出血是PCI常见并发症[11],不同穿刺位点出血风险存在差异。与股动脉相比,经桡动脉PCI的出血风险较低[12]。CENTURY Ⅱ随访研究显示,急诊经桡动脉PCI的患者住院和随访期间出血并发症较少(住院:1.7% vs. 6.2%,P<0.001;随访:2.7% vs. 9.6%,P<0.001)[13]。另一项针对10 590例冠脉慢性闭塞患者荟萃分析显示,经桡动脉PCI的大出血风险也较低(0.18% vs. 0.9%,P<0.001)[14],根据不同穿刺路径应采取个体化止血策略。
3.2.2 药物影响 血小板活化是止血基础[15]。抗血小板药物阿司匹林对PCI术后止血影响呈多样性。除抗栓作用外,停药后会出现促血栓形成效应,这种血栓倾向与环氧合酶-2受抑制有关[16]。了解患者抗栓药物的使用情况有利于优化止血决策。
3.2.3 内环境改变 急性冠脉综合征患者内环境微泡增加,促进血小板聚集[17]。PFA-100采用闭合时间评估患者血小板聚集性[18]。血小板高聚集表现为充分抗栓后血小板活性仍正常。对于血小板高聚集的患者应适当缩短压迫时间以降低血栓风险。
3.2.4 止血方法 止血方法主要包括人工压迫和止血器。荟萃分析显示止血器可以减少围术期并发症如动静脉瘘、假性动脉瘤等[20],缩短卧床时间,改善患者体验。使用止血器的劣势主要为学习曲线效应,应组织学习,加强使用止血器有效止血的培训。
3.3 小结
经皮冠脉介入围术期止血技术的研究尚处于发展阶段,我国研究数量和质量均有待提高,应针对止血器开展以护理为主导的多学科研究。
[参考文献]
[1] Krittanawong C,Kumar A,Wang Z,et al.Coronary artery disease in the young in the US population-based cohort[J].Am J Cardiovasc Dis,2020,10(3):189-194.
[2] Karacsonyi J,Brilakis ES.Percutaneous coronary interven- tion:The "oculosufficient" effect and how to overcome it[J].Catheter Cardiovasc Interv, 2020,95(7):1267-1268.
[3] Doenst T,Haverich A,Serruys P,et al. PCI and CABG for treating stable coronary artery disease:JACC review topic of the week[J].J Am Coll Cardiol,2019,73(8):964-976.
[4] Watanabe H,Domei T,Morimoto T,et al. Effect of 1-month dual antiplatelet therapy followed by clopidogrel vs 12-month dual antiplatelet therapy on cardiovascular and bleeding events in patients receiving PCI:The STOPDAPT-2 randomized clinical trial[J].JAMA,2019,321(24):2414-2417.
[5] Kumar V,Wish M,Venkataraman G,et al. A randomized comparison of manual pressure versus figure-of-eight suture for hemostasis after cryoballoon ablation for atrial fibrillation[J].J Cardiovasc Electrophysiol,2019,30(12):2806-2810.
[6] Clementy N,Fernandes J,Carion PL,et al. Pacemaker complications and costs: A nationwide economic study[J].J Med Econ,2019,22(11):1171-1178.
[7] Cilingiroglu M,Kilic I.What about a larger closure device?[J].Catheter Cardiovasc Interv,2020,96(2):479-480.
[8] Lavoie N,Parker J,Legree PJ,et al. Using latent semantic analysis to score short answer constructed responses:Automated scoring of the consequences test[J].Educ Psychol Meas,2020,80(2):399-414.
[9] Kim SY,Lim W.Cluster burst synchronization in a scale-free network of inhibitory bursting neurons[J].Cogn Neur- odyn,2020,14(1):69-94.
[10] Jones PJ,Ma R,Mcnally RJ.Bridge centrality:A network approach to understanding comorbidity[J].Multivariate Behavioral Research,2019,56(2):1-15.
[11] Marquis-Gravel G,Dalgaard F,Jones AD,et al. Post-discharge bleeding and mortality following acute coronary syndromes with or without PCI[J].J Am Coll Cardiol,2020, 76(2):162-171.
[12] Le May M,Wells G,So D,et al. Safety and efficacy of femoral access vs radial access in ST-segment elevation myocardial infarction:The SAFARI-STEMI randomized clinical trial[J].JAMA Cardiology,2020,5(2):126-134.
[13] Campelo-Parada F,Carrie D,Bartorelli AL,et al. Radial versus femoral approach for percutaneous coronary intervention:MACE outcomes at long-term follow-up[J].J Invasive Cardiol,2018,30(7):262-268.
[14] Megaly M,Karatasakis A,Abraham B,et al. Radial versus femoral access in chronic total occlusion percutaneous coronary intervention[J].Circ Cardiovasc Interv,2019,12(6):e007 778.
[15] Brouns SLN,Van Geffen JP,Heemskerk JWM. High-thr-oughput measurement of human platelet aggregation under flow:Application in hemostasis and beyond[J].Platelets,2018,29(7):662-669.
[16] Eizayaga FX,Belon P,Desplat V,et al. Effects of ultra-low-dose aspirin in thrombosis and haemorrhage[J].Homeopathy:The Journal of the Faculty of Homeopathy,2019,108(3):158-168.
[17] Kafian S,Wallen H,Samad BA,et al. Microvesicles from patients with acute coronary syndrome enhance platelet aggregation[J].Scand J Clin Lab Invest, 2019,79(7):507-512.
[18] Favaloro EJ,Bonar R. An update on quality control for the PFA-100/PFA-200[J].Platelets,2018,29(6):622-627.
[19] Kweon OJ,Lim YK,Kim B,et al. Effectiveness of platelet function analyzer-100 for laboratory detection of anti-platelet drug-induced platelet dysfunction[J].Ann Lab Med,2019,39(1):23-30.
[20] Noori VJ,Eldrup-Jorgensen J. A systematic review of vascular closure devices for femoral artery puncture sites[J].J Vasc Surg,2018,68(3):887-899.
(收稿日期:2021-06-15)
猜你喜欢
中国当代医药(2016年32期)2017-02-23 15:00:11
中国当代医药(2016年31期)2017-02-23 14:59:20
中国实用医药(2016年29期)2016-12-26 10:10:10
科技视界(2016年18期)2016-11-03 21:58:33
中国实用医药(2016年24期)2016-10-17 05:58:58
中国实用医药(2016年24期)2016-10-17 04:11:14
上海医药(2016年17期)2016-10-12 01:55:41
中国实用医药(2016年12期)2016-05-04 09:37:35
中外医疗(2015年16期)2016-01-04 06:51:46
西南军医(2015年5期)2015-01-23 01:25:05