Converting the Functional Independence Measures(FIM)-motor Scores to Modified Barthel Index(MBI)Scores—A Data Mining Approach
2021-12-20 03:01WONGLikhangGaryWONGKammanSimonNGHinPoBobby
康复学报 2021年5期
WONG Lik-hang Gary ,WONG Kam-man Simon ,NG Hin-Po Bobby
1 Tung Wah College,Hong Kong,China;2 Occupational Therapy Department,Tai Po Hospital,Hong Kong,China;3 Occupational Therapy Department,Kowloon Hospital,Hong Kong,China
ABSTRACT Objective:To meet both clinical and research needs,this study developed and evaluated a conversion method between the Modified Barthel Index (MBI) and the Functional Independence Measures (FIM).Methods:This was a retrospective analysis of both MBI &FIM assessment data,which were collected concurrently in a local hospital for stroke patients attending rehabilitation programs in the period from 2005 to 2016.The scorings were rated at the beginning of the rehabilitation.Data mining procedures,which involved the following steps:a)selection of appropriate samples,b)pre-processing of the dataset,c)transformation of the dataset,d)analyzing the data patterns,e)deriving the conversion based on"rank-invariant statistical method",and,f)verifying the conversion method — were adopted for data analysis.Results:Six thousand five hundred and seventyfour cases,which were verified as "error-free",were randomly allocated into two compatible subsets.Using the data from subset (A),we substantiated that all the total scores and every corresponding paired item scores between the MBI and the FIM-motor were highly correlated(i.e.Kendall's tau-b Value ranged from 0.796 to 0.987,P<0.01).Based on"rank-invariant statistical method"an item-to-item conversion table was also developed.Using the data from subset (B) we found the Cohen's Kappa coefficients (k) for either "single-pair" items or "multiplepair" items ranged from 0.770 to 0.913 — which indicated "substantial" to "almost perfect" agreement between the rated MBI scores and the derived MBI scores.Conclusion:A"user-friendly" and yet methodologically sound conversion method is recommended for application in stroke rehabilitation program.
KEY WORDS Functional Independence Measures;Modified Barthel Index;functional assessment;stroke rehabilitation
1 Introduction
The Modified Barthel Index (MBI) and the Functional Independence Measures (FIM) are two functional assessments that are commonly used to document rehabilitation outcome worldwide and in local rehabilitation settings.The 10-item Barthel Index (BI)was developed in 1955[1],and,it remains a cornerstone of a disability measurement in the field of rehabilitation.Many modifications to the original BI had been recommended since then.The original version of BI was modified with upgrading the 3-point scale to 5-point scale to some items with the intention of improving its responsiveness[2].A Chinese version MBI was also developed to accommodate a few culture-specific components related to task content descriptions[3].On the other hand,the FIM was developed as part of the Uniform Data System for Medical Rehabilitation(UDSMR)[4].The FIM was developed in response to the limitations of the BI—being considered too restricted and poorly responsive.The 18-item FIM instrument consists of a minimum number of 13 motor and 5 cognition items being rated on a 7-level scale to describe stages of complete dependence to complete independence in the performance of basic daily living activities.Many studies supported the validity of the FIM that it could provide an estimate of the burden of care[5-6].The development of FIM &UDSMR also marked the cornerstone of application of functional assessment in more areas:(1) evaluating individual and program outcomes;(2) planning rehabilitation interventions;(3) determining effectiveness;(4) maintaining continuity;(5) improving resources,and,(6)determining manpower needs[7].
With the intention to advise on which functional assessment tool was better than the other,head-to-head comparisons between the two measures in terms of their reliability,validity,and responsiveness had been conducted[8-9].Another review of publications on randomized controlled trials (RCTs) of stroke rehabilitation published between 1968 and 2002 were conducted.The frequency with which the BI and FIM measures were used relative to other measures of disability was reviewed[9].The results indicated that BI was used more often than FIM especially in those studies originating in Europe[9].However,studies from North America were more likely to use the FIM.This might be due to the reason that FIM-change score was adopted as one of the indicators in the Prospective Payment System,which is a reimbursement of medical insurance in the United States[10].Besides the regional preference,there were of course other factors that individual settings would consider in the choice of their functional assessment tool.These factors included:(1) the acceptance from frontline practitioners;(2) the time required for completing the instrument;(3) related subscription charges;(4) other back-up functions to the application of the concerned functional assessment,and,(5) benchmark references value on functionally related groups concerning prognosis.In the local settings of Hong Kong,FIM were applied in studying rehabilitation outcomes of patients suffering from hip fractures[11]and predicting length of hospital stay of stroke patients undergoing rehabilitation[12].However,using FIM requires subscription charges,which hinders some settings from using it.Thus,it's foreseeable in the near future that there would not be a single functional assessment tool being used in the field of rehabilitation— both MBI and FIM would coexist.
In views of the needs for pooling data for metaanalysis and comparing outcomes of different rehabilitation programs,conversion of scores across these two instruments can be a solution.It is a necessity to derive empirically valid conversion methods for these two instruments.Thus,the purpose of our research work was to employ a data mining approach in order:(1) to derive a simple but valid method for converting the FIM-motor scores into the MBI scores,and,(2) to verify the conversion method by testing of the degree of agreement between the therapist-rated scores and the derived scores.
2 Methods
This was a retrospective analysis of functional assessment data which were collected concurrently in a local rehabilitation hospital for seven thousand,five hundred and sixteen (7,516) stroke patients in a 10-year period,i.e.from 2005 to 2016.The study data set comprised all their MBI &FIM scores,which were rated at the beginning of their rehabilitation process by their case occupational therapists who were trained in rating with both instruments.This study adopted the "Data Mining" approach in examining this huge data set and followed through the following six steps,as illustrated by experts of the field[13-15].
2.1 Data selection
The data were selected from the clinical database of an occupational therapy department in a rehabilitation hospital,which was specifically designed for capturing data of the patients who were suffering from stroke and receiving the in-patient stroke rehabilitation in that hospital.The dataset included therapists'ratings on patients' level of independence in ADL using both measures — the MBI and the FIM concurrently at the beginning of the stroke rehabilitation process.Data for those stroke patients who were admitted to the hospital for rehabilitation in the period from 01 Jan 2005 to 31 Dec 2016 were retrieved.
2.2 Data pre-processing
After data retrieval,the whole data set was scanned for possible data entry errors.After the preliminary scanning,the first author prepared a list of possible error types.The list was then reviewed among all the authors until a consensus was concluded.The enlisted types of error included (1) missing significant variables (e.g.,age,gender,diagnosis,case therapists,etc.),(2) extreme figures (e.g.,age under 18,2-calendar-day or more discrepancy between the date of rating in two instruments,2-year or more length of stay in hospitalization),and,(3) possible rating error (e.g.,missing rating in any items,ratings in extreme opposite in the two ADL instruments,incorrect numeric figures in a particular items,etc.).The whole data set were reviewed again by the first author based on the finalised list.Records with any enlisted error were excluded from further analysis.
2.3 Data transformation
Those data after being verified as "error-free" were randomly allocated into two independent subsets of roughly equal in numbers.These two subsets were firstly tested for homogeneity in terms of their demographics,types of strokes,case therapists,length of stay and functional independence at intake before any further operations.This random allocation exercise would be repeated until two homogeneous subsets of data were generated.Then these two homogeneous subsets of data would be used for different purposes.The first subset (A),would be used for Step 4 — Pattern analysis,and,Step 5 — Deriving the conversion method.The second subset (B) would be used for Step 6—Verification of the conversion method.
2.4 Pattern analysis
This step intended to validate if MBI &FIM measured the same dimension as well as in the same direction.The correlations between the total scores of the two measures as well as the corresponding individual item scores of the two measures were tested.Bivariate correlation coefficient was applied between the MBI total scores and the FIM-motor total scores while ordinal-by-ordinal bivariate correlation analysis,usingKendall's tau-bmeasures,would be used for related paired items from the two instruments (Figure 1).For tasks such as dressing,toileting,and bathing,there were two related items in the FIM-motor instrument,e.g.dressing upper body and dressing lower body of the FIM-motor instrument.The MBI items were firstly paired with both related FIM-motor items individually,e.g."Dressing" of MBI was paired with both"Dressing Upper Body" and "Dressing Lower Body"individually.
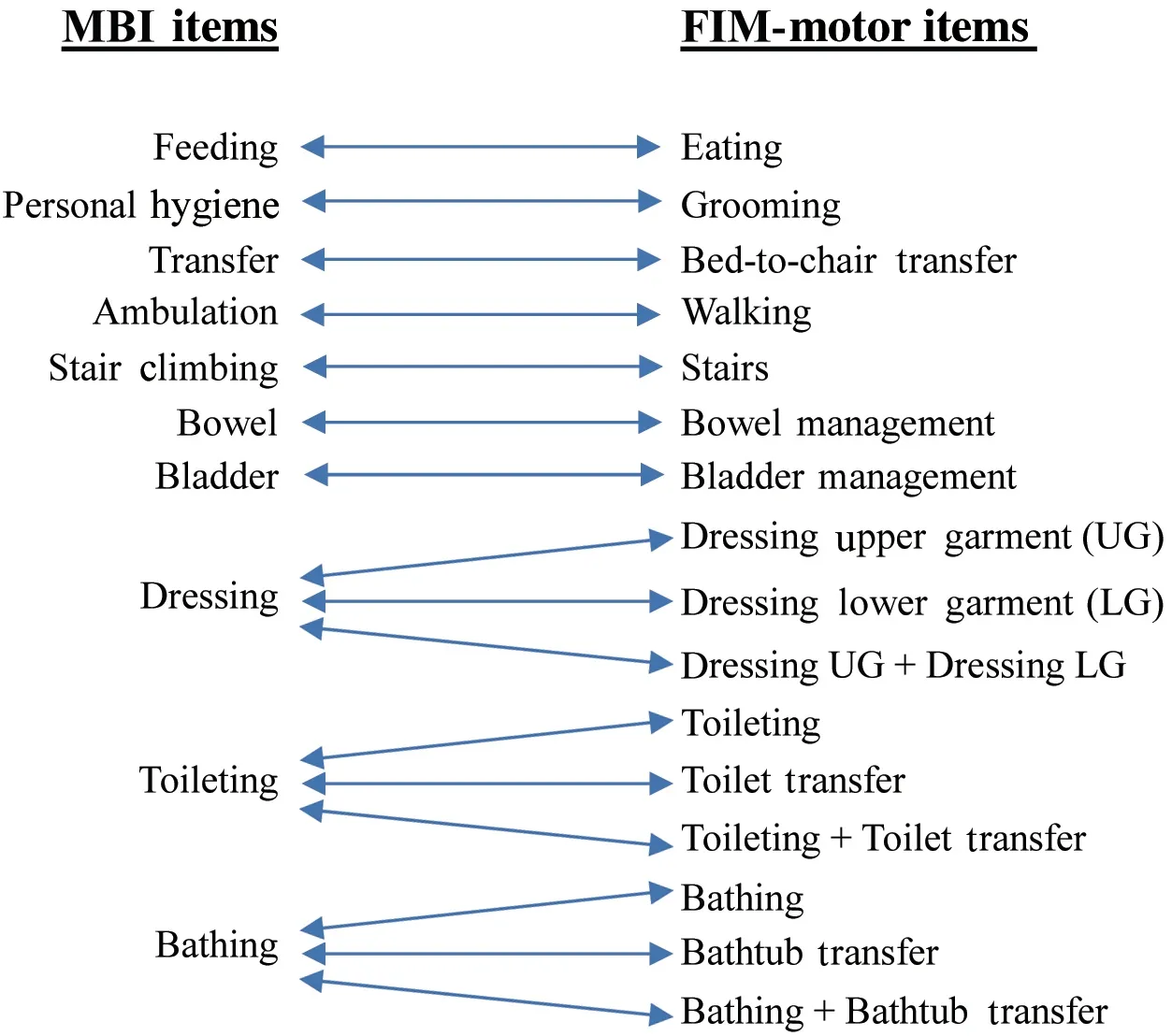
Figure 1 Pairing of Items between MBI&FIM derived from Step 4—Pattern analysis
2.5 Deriving the conversion method
The development of conversion methods was based on the statistical method called"rank-invariant statistical method" suggested by GOSMAN-HEDSTRÖM &SVENSSON[16].Firstly,for each pair of items,a contingency table was formed.The number in each cell represented the ratings in two instruments rated by the same therapist.Hypothetically,for two perfectly coherent instruments,the ratings would be arrayed in the cells located around the diagonal of the table(Figure 2).In order to form a 5×5 contingency table,the 7-level scale in FIM-motor had to be condensed into a 5-level scale.There were many possible patterns of condensation and different pattern would lead to change in the distribution of disarrayed ratings.Eventually,pattern with least disarrayed ratings would be regarded as the most "preferable" conversion method,as it would lead to best parallel reliability between the two instruments[15].
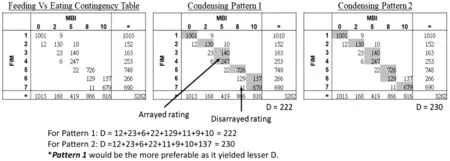
Figure 2 Example of contingency table for MBI-feeding and FIM-eating
2.6 Verification of the conversion method
Based on the derived conversion method,FIM-motor items scores would be converted into MBI scores in the subset (B).Kappastatistic was used to verify the agreement between the derived MBI score and the original score rated by the therapists.
3 Results
There were totally 7,516 number of cases retrieved as the starting data set.All these data were rated by 36 occupational therapists in the same inpatient rehabilitation facility.Nine hundred and forty-two cases(12.5%) were reviewed as "error free".Table 1 summarized the counting of different errors.Eventually,only 6,574 cases(87.5%)were verified as"error-free",and they were randomly allocated into two subsets.The first subset (A) included 3,282 cases (49.9%) and the second subset (B) included 3,292 cases (50.1%).In the testing for homogeneity between the two subsets,there were no significant differences found in major clinical variables between these two subsets of data (Table 2).The first subset (A) was used for Step 4—Pattern Analysis and Step 5—Deriving the Conversion Method.The correlation coefficient between the MBI total score and the FIM-motor for this subset(A) was 0.987 (P<0.01).Moreover,the ordinal correlation coefficients of every item pairs ranged from 0.796 to 0.961(P<0.01)(Table 3).
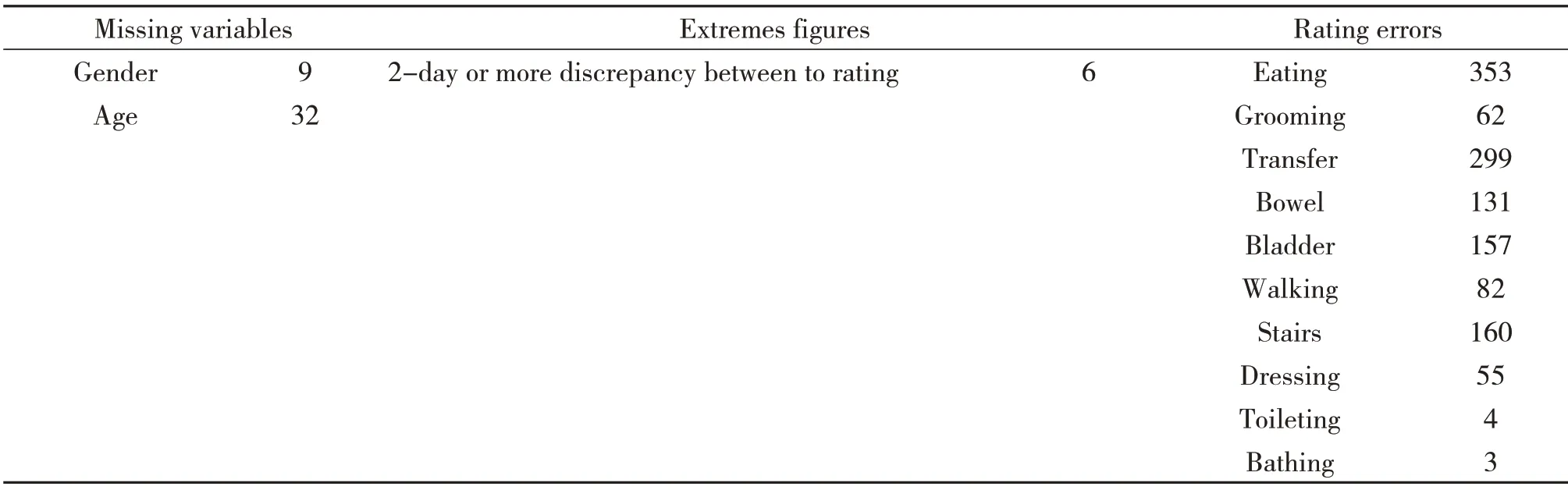
Table 1 Counting of different errors among the 7,516 cases in the original dataset
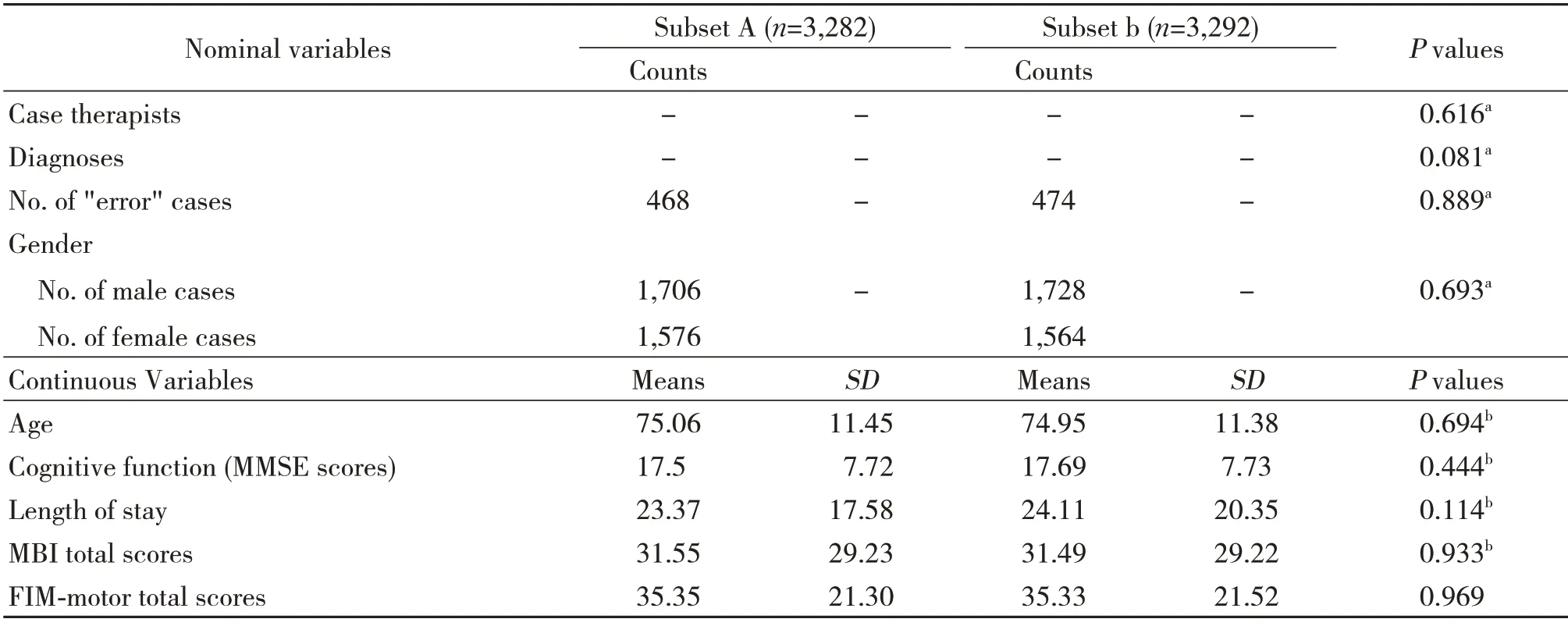
Table 2 Comparison between the two subsets
Table 4 showed the item-by-item conversion patterns,together with the results ofKappastatistical analysis of agreement between the derived scores and the actual scores in the subset (B).For single-pair items,such as eating,grooming,transfer,walking,stair climbing,bowel and bladder control,the Cohen'sKappacoefficients (k) ranged from 0.808 to 0.913,which indicated"substantial"to"almost perfect"agreement[17].For MBI dressing,the best agreement was yielded with the score derived from FIM dressing low-er garment item alone (k=0.770,indicates "moderate"agreement).For MBI toileting,the best agreement was yielded with the score derived from the FIM toileting item alone (k=0.852,indicates "almost perfect"agreement).For MBI bathing,the best agreement was yielded with the FIM bathing item alone (k=0.802,indicates "substantial" agreement).Table 4 also showed another interesting finding:majority of items rated as 6 (modified independence) in FIM fell into Level 4 in MBI,except for items eating,grooming and bathtub transfer.
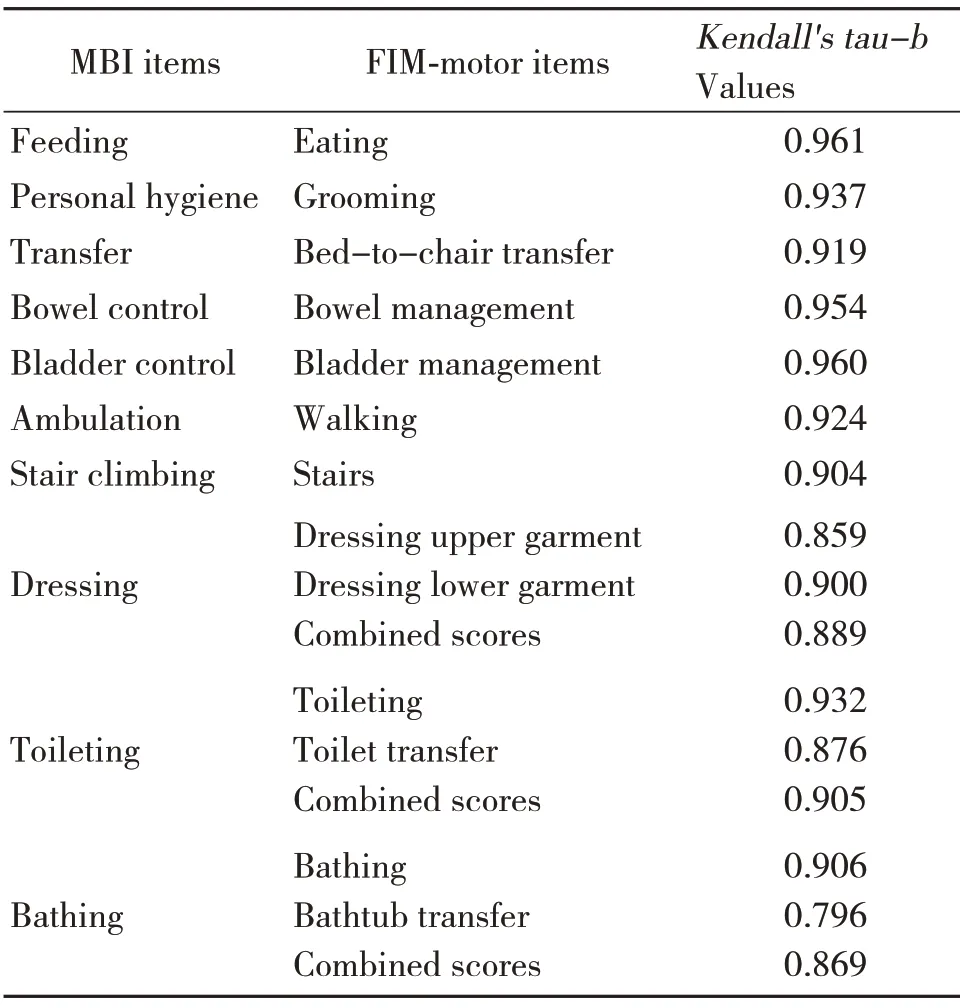
Table 3 Ordinal by ordinal correlations among paired items in data subset A(n=3,282)
4 Discussion
Our team recommended a simple method for converting the FIM-motor scores into the MBI scores,i.e.checking against the conversion table as listed in Table 4.This finalized conversion table appeared to be user-friendly to both clinicians who worked in busy clinical settings,and,researchers who could use simple conversion formula during the data-input process.This conversion method also appeared valid as it was verified by robust statistical procedures.There were prior attempts to offer the conversion of FIM into MBI scores by other research teams.Nyein,McMichael and Turner-Stokes primarily suggested that conversion of FIM-motor scores to BI scores through a theoretical approach[18].After "careful examination"of the scoring manual of the two instruments,they de-rived the conversion criteria and verified them withKappastatistics.In the item-by-item analysis,theKappacoefficients ranged from 0.53 (in feeding) to 1(in bathing).On the other hand,GOSMAN-HEDSTRÖM &SVENSSON[16]suggested a statistical method called,the "rank-invariant method" that could condense 7-level FIM-motors score to 3-level BI score.They ascertained that FIM and BI were concordant to each other on the item-to-item level;the percentage of agreement between real scores and derived scores ranged from 78% to 97% among all the items.HONG et al.[19]also attempted to create a crosswalk between FIM motor items and the Korean version of the 5-level Modified Barthel Index (K-MBI)using the Rasch equating method.Three measurement constructs were identified:self-care,mobility,involuntary movement.The equated test items in the three constructs demonstrated good person separation reliability (r=0.94-0.96) and good internal consistency (Cronbach's alpha=0.93-0.97).The three crosswalks between the FIM raw scores and converted K-MBI scores demonstrated good correlations (r=0.91-0.93,allP<0.0001).However,in all these studies,the conversion methods were verified by calculating the level of agreement between the derived scores and the original scores from the same data source.This method might inherit a certain degree of agreement before the formulation of the conversion method.To address this,our team insisted on using another independent but homogeneous set of data to examine the utility and validity of the conversion method,i.e.we used two datasets,one for deriving the conversions and the other one for testing the results of the conversion in order to minimize the effect of any potential intrinsic errors.Besides this,our work had some more methodologically advantages:a)we used a huge dataset,i.e.6,574 patients,b)we were able to derive an"item to item"conversion rather than conversions to total or sub-total scores only,&,c) we adopted the data mining approach,an emerging field that had received more attention and recognition in related field of studying psychometric properties of assessment tools.
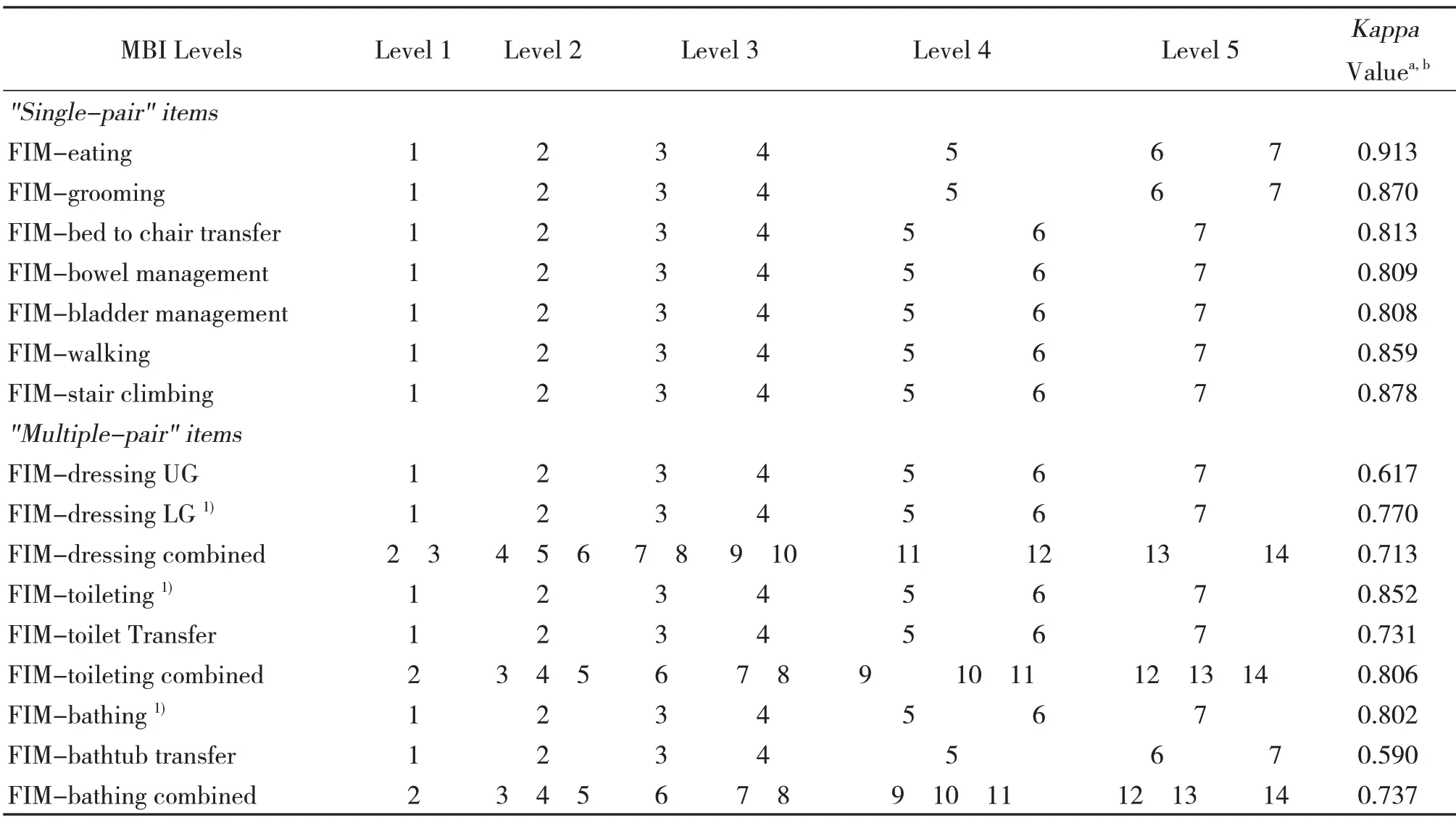
Table 4 Item-by-item conversion patterns derived from data subset A
However,we were aware of the potential limitations of our study and some interesting findings in our analysis,which worth notification and serious considerations by other clinicians and researchers in the future.Firstly,readers were reminded that the rating criteria of the MBI and the FIM were slightly different.For the FIM rating criteria,other performance quality indicators were also included other than "level of assistance" for some items (e.g.travel distance in walking and stair climbing,the frequency of accidents in bowel/bladder management).Our methodology for developing the conversion table was solely depended on existing clinical data.Thus,the resulted conversion table might deviate from the theoretical understanding of the rating criteria between two measuring instruments.This might be accountable for some variation in ratings between two instruments.Secondly,regarding the three special item pairs,i.e."Dressing","Toileting" and "Bathing",single FIM-motor item yielded the bestKappavalue,instead of the combined pairs.For example,scores derived from a single "dressing lower garment" item yielded the bestKappavalue with the MBI "dressing" item.We thought this might be related to two phenomenon:i) frontline practitioners would consider safety during dressing lower body as essential,i.e.fall accident,and,incline to be more conservative in rating dressing lower bodytherefore the rating on lower garment dressing would have higher weight on the overall dressing rating,and ii) when activities were made up of highly inter-dependent task components (dressing lower body was made up of more inter-dependent tasks while dressing upper body was made up of more independent tasks),a behaviourally anchored gross rating protocol might be more effective;that might be the reason why the reliability of dressing lower body was higher than the composite value[20].Score 6 in FIM means modified independence,including the need of supervision or use of assistive device,while Level 4 in MBI indicates the need of supervision.The findings in the conversion table showed that most of the items in FIM score 6 fell into Level 4 in MBI.Only in eating,grooming and bathtub transfer,FIM score 6 fell into Level 5 in MBI.This indicated that therapists were prone to neglect the supervision or assistive device required by patients in rating these three items in MBI.Finally,the conversion table was only applicable to only one diagnostic group,i.e.people with stroke.For clientele of another diagnostic group,the development of another conversion method based on corresponding clinical data would be required.
To conclude,this study derived a conversion of FIM motor items into corresponding MBI item score using a data mining approach.We have confidence in its validity based on its huge dataset and using two homogenous data sets for independent purposes;one for deriving the conversion and the other for verifying the conversion.The finalized conversion table facilitate the conversion of the FIM into the MBI scores for both clinical handover between settings that used different functional measures as well as pooling data for meta-analysis.However,as only stroke patients were involved,we have hesitation in recommending its application in other patient groups.Moreover,there was only one hospital involved in the study.