
Early serum albumin changes in patients with ulcerative colitis treated with tacrolimus will predict clinical outcome
2021-06-24 01:31NatsukiIshidaTakahiroMiyazuSatoshiTamuraShinyaTaniMihokoYamadeMoriyaIwaizumiYasushiHamayaSatoshiOsawaTakahisaFurutaKenSugimoto
World Journal of Gastroenterology 2021年22期
Natsuki Ishida, Takahiro Miyazu, Satoshi Tamura, Shinya Tani, Mihoko Yamade, Moriya Iwaizumi, Yasushi Hamaya, Satoshi Osawa, Takahisa Furuta, Ken Sugimoto
Abstract
Key Words: Ulcerative colitis; Tacrolimus; Albumin
INTRODUCTION
The incidence of ulcerative colitis (UC) is increasing worldwide[1 ]. Although corticosteroid treatment is the highest priority treatment option for patients with moderate to severe UC, there are patients with steroid dependence or resistance, and approximately 20 %-30 % of them do not improve following steroid treatment[2 ,3 ]. Although therapeutic agents such as biologics and calcineurin inhibitors are used as medical treatments to replace steroids, if none of these advanced treatments are successful,colectomy must be performed for these patients.
Treatment with oral tacrolimus, a calcineurin inhibitor, has been reported to be effective in patients with steroid-dependent and steroid-resistant UC[4 ,5 ]. Recently, in addition to studies on short-term results of tacrolimus for UC, studies on medium-tolong-term treatment results have also been reported[6 -9 ]. Although the efficacy of tacrolimus has been demonstrated in these reports, there are patients who have failed to respond to this treatment and are forced to switch to other treatments, such as biologic therapy and colectomy. Continuing refractory treatment unnecessarily prolongs hospital stay and increases the risk of immunosuppressive and perioperative complications due to poor nutritional status[10 ,11 ]. When oral tacrolimus initially became available as a therapeutic agent for UC, only anti-tumor necrosis factor (TNF)α antibody agents were indicated for UC as biologics; however, various advanced treatments, including small-molecule Janus kinase inhibitors, anti-interleukin 12 /23 antibodies, and anti-integrin antibodies are now available[12 -14 ]. This means that we now have many alternative treatment options for tacrolimus refractory cases. Hence,the decision to switch to another treatment must be made as soon as possible and accurately in refractory cases.
Several studies have validated the therapeutic response to tacrolimus in UC.Nishidaet al[15 ] proved that the neutrophil-to-lymphocyte ratio was an independent prognostic factor after the induction of tacrolimus therapy. Banet al[16 ] reported that the factors predicting colectomy after the induction of calcineurin inhibitor were cytomegalovirus antigenemia (C7 HRP) positivity, a cumulative prednisolone dose of 10000 mg or more before the start of treatment, and a combination of hematocrit and the Onodera-prognostic nutritional index[16 ]. This study also demonstrated that the serum albumin (Alb) level before the induction of tacrolimus was useful as a predictor of early colectomy. Further, Herrlingeret al[17 ] reported that ABCB1 single-nucleotide polymorphisms predict the therapeutic response to tacrolimus.
In this study, we retrospectively examined the clinical course after the induction of remission by tacrolimus and the factors involved in its clinical outcome. As a prognostic factor that can be easily measured in clinical practice, changes in serum Alb levels before and after the induction of remission with tacrolimus were evaluated.
MATERIALS AND METHODS
Patients
Patients with UC who were treated with tacrolimus and had a medical record at the Hamamatsu University School of Medicine between August 2010 and January 2020 were enrolled in this study. The diagnosis of UC was made based on typical medical history and clinical features, as well as endoscopic and histological evaluation, in line with recent guidelines. Patients with inflammatory bowel disease (IBD) who were not diagnosed with UC, such as indeterminate colitis or unclassified IBD, were excluded.Patients were diagnosed with moderate to severe UC based on clinical activity index,biological data, and endoscopic findings.
Study design
This was a retrospective observational study conducted in a single center. The purpose of this study was to identify prognostic factors that may lead to clinical failure in patients with UC treated with tacrolimus. The primary outcome measure of this study was clinical failure in which a switch to colectomy or biologics was performed within 3 mo after tacrolimus induction. Secondary endpoints were comparison of biological data and clinical findings between the remission and failure groups.
Disease assessment
Enrolled patients were evaluated for clinical disease activity using the Rachmilewitz index[18 ]. The values of serum C-reactive protein (CRP), Alb, hemoglobin (Hb), and white blood cell (WBC) count and differential were measured in our facility on admission and more than twice per week.
Endoscopic assessment
Colonoscopy was performed on all enrolled patients before tacrolimus induction. UC mucosal status was assessed using the Mayo endoscopic subscore (MES)[19 ]. MES was assessed according to the following criteria: 0 , normal or inactive disease; 1 , mild disease with erythema, decreased vascular pattern, mild friability; 2 , moderate disease with marked erythema, absence of vascular patterns, friability, and erosions; and 3 ,severe disease with spontaneous bleeding and ulceration. Mucosal healing was defined as MES 0 or 1 .
Tacrolimus therapy and follow-up
The initial tacrolimus dose was started at 0 .05 mg/kg twice daily. The blood trough levels of tacrolimus were measured 2 to 3 times a week, and tacrolimus doses were adjusted. The dose of tacrolimus was increased until a high trough level of 10 -15 mg/mL was achieved. In this study, we defined day 1 as the day when a high trough level was reached after the start of oral tacrolimus administration. Oral administration of tacrolimus at a dose capable of maintaining a high trough level was continued for 2 wk, and then the dose was reduced to a low trough level (5 -10 ng/mL). In this study,patients who underwent colectomy or switched to biologics within 3 mo after day 1 were defined as having clinical failure.
Statistical analysis
Statistical analyses of the data were performed using SPSS version 24 (IBM, Armonk,NY, United States) and SAS version 9 .4 (SAS Institute, Cary, NC, United States)software. Differences between median values were compared using the Mann-Whitney U test and Fisher’s exact test. Receiver operating characteristic (ROC) analysis was conducted to determine the optimal Alb cut-off value (week 2 /week 0 ) for predicting failure within 3 mo. The accuracy of the predicted failure ratio was evaluated using the area under the ROC curve. The cumulative remission rate was analyzed using Cox proportional hazard regression and Kaplan-Meier analysis, and was compared using the log-rank test.P< 0 .05 was considered as statistically significant.
Ethical statement
This retrospective study protocol was reviewed and approved by the Ethics Committee of Hamamatsu University School of Medicine (number 20 -356 ). This study was conducted in accordance with Good Clinical Practice principles in adherence to the Declaration of Helsinki.
MSCT对狭窄度≥70%、50%~70%者诊断的敏感度、准确度、特异度、阳性预测值等较狭窄度<50%者均显著较高,且P<0.05。见表2。
RESULTS
Patient characteristics
The characteristics of forty-seven UC patients enrolled in this study are shown in Table 1 . The mean patient age was 44 .9 years, and the mean disease duration was 3 .2 years. Patients with extensive colitis and left sided colitis numbered 42 and 5 ,respectively. On colonoscopy, 38 patients (80 .9 %) had MES 3 , and nine patients (19 .1 %)had MES 2 . Twelve patients (25 .5 %) had a history of treatment with biologics. The mean time to high-level trough with tacrolimus was 8 .1 d.
Comparison of the remission and failure groups
During the 3 -mo follow-up from the start of the study, 17 of 47 patients (36 .2 %)experienced clinical failure. On comparison of the remission and failure groups, as shown in Table 2 , the failure group was older and tended to have a longer disease duration than the remission group, but this finding was not statistically significant. In addition, a history of treatment with biologics did not show a significant difference between the two groups.
IMF:亚洲需加强政策缓冲以应对不确定性。5月25日,IMF副总裁张涛在亚洲货币政策论坛上发言表示,亚洲需重建货币和财政缓冲,增强经济韧性以应对未来不确定性。张涛指出,亚洲经济短期向好但面临潜在风险:如外债大幅增加,公共债务占GDP比重从2007年的46%上升到59%,私人部门债务高企;财政平衡继续恶化,平均赤字已达GDP的1.1%。
Comparison of biological data between remission group and failure group
We compared biological data between the remission and failure groups before the start of treatment (week 0 ), 1 wk after the start of observation (week 1 ), and 2 wk after the start of observation (week 2 ) (Table 3 ). No significant difference was observed regarding the biological data before the start of treatment (week 0 ) between the two groups. There was no significant difference in biological data in week 1 , and only serum Alb level in week 2 showed a significant difference between the remission and failure groups (P= 0 .015 ).
In order to compare the changes in biological data before and after the start of treatment between the remission group and the failure group, the percentage of each value based on week 0 was calculated (Table 4 ). The week 1 /week 0 ratio showed no significant difference in Alb, CRP, Hb, and WBC values. The week 2 /week 0 ratio was significantly different only for Alb values between the remission and failure groups (P= 0 .003 ).
Prediction of subsequent relapse using week 2 / week 0 Alb ratio
Since it was shown that the week 2 /week 0 Alb ratio may be a factor predicting clinical failure for 3 mo, ROC analysis was performed using this ratio (Figure 1 ). The cut-off Alb ratio for week 2 /week 0 was 1 , and its sensitivity and specificity were 0 .539 and 0 .867 , respectively. The AUC was 0 .751 (95 %CI: 0 .604 -0 .898 ).
Furthermore, in order to investigate the reason for the cut-off value of 1 by week 2 ,we investigated the change in the Alb ratio (Figure 2 ). The Alb ratio increased significantly from week 0 to week 1 and showed a further increase from week 1 to week 2 (P = 0 .036 and P < 0 .001 , respectively). In addition, when the Alb ratio was examined from the viewpoint of whether it was more or less than 1 in value, 40 .4 % of the patients in week 1 had an Alb ratio ≤ 1 (Figure 2 ). In contrast, at week 2 , the number of patients with Alb ratio ≤ 1 decreased to 27 .2 %, and the number of patients with an Alb ratio > 1 increased to 72 .8 %.
Comparison of failure prediction using week 2 / week 0 Alb ratio
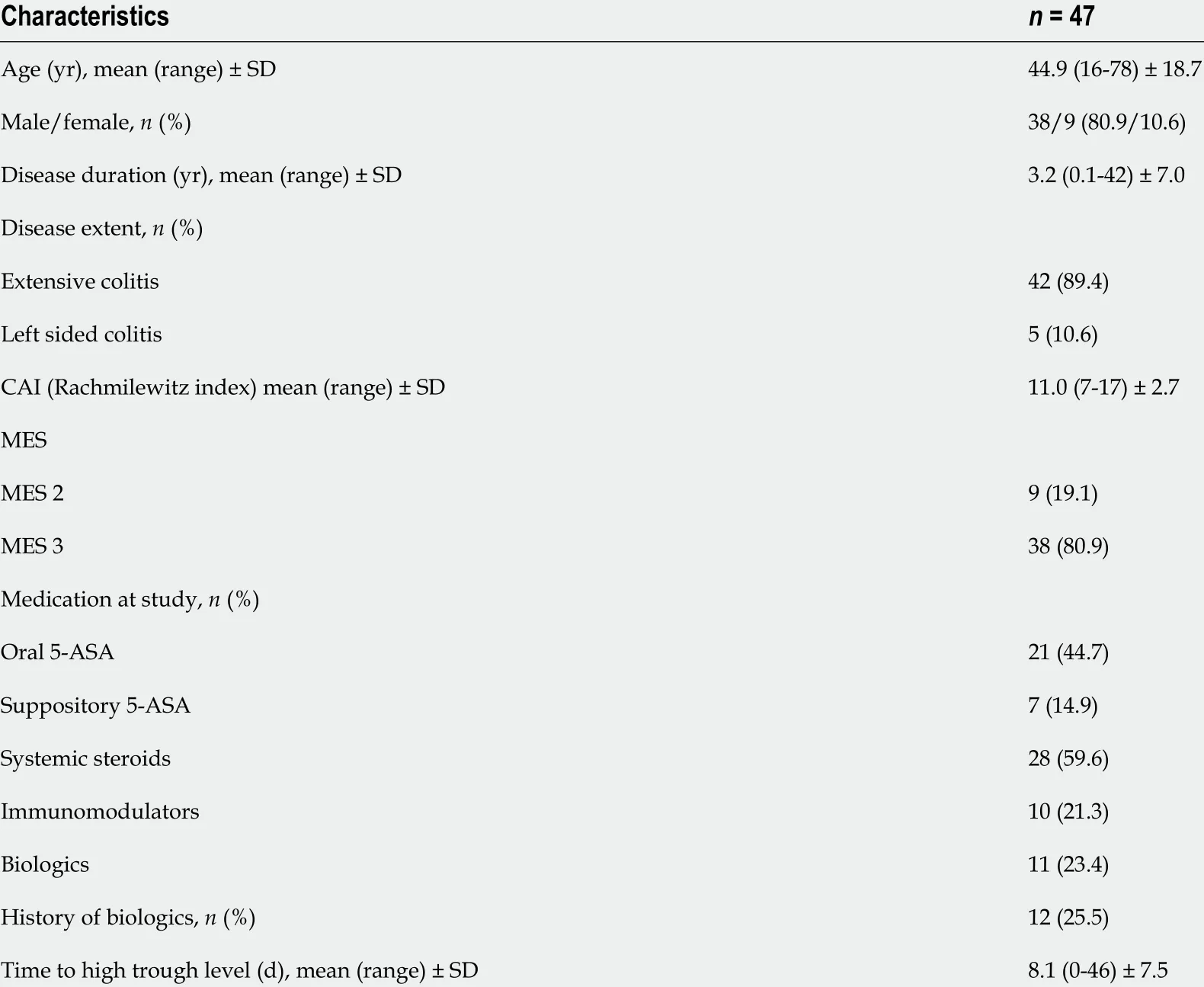
Table 1 Baseline characteristics of patients
DISCUSSION
This study aimed to explore factors that could predict the prognosis of oral tacrolimus for UC. In particular, the analysis focused on biological data, which is a marker widely used in clinical practice. Tacrolimus is a calcineurin inhibitor used in patients with steroid-dependent or refractory UC and is indicated for moderate to severe cases.However, there are some cases in which colectomy is unavoidable due to ineffective treatment with tacrolimus. Approximately 6 .1 %-66 .7 % patients who were treated with tacrolimus underwent colectomy[6 -8 ,20 -26 ]. Therefore, the possibility of performing colectomy in the future should be considered, especially when starting treatment with tacrolimus for patients with very severe UC.
Conventionally, surgical treatment for IBD has many potential perioperative complications, and poor nutrition further increases the risk of postoperative complications[11 ,27 ]. Unnecessarily prolonging preoperative medical treatment will worsen the nutritional status of patients with UC, and surgical treatment in that malnourished state will further increase the risk of postoperative complications. It is extremely important to judge the effectiveness of treatment for UC at an early stage and to consider the next treatment before the general condition worsens. In this study, we searched for prognostic factors that could predict the efficacy of tacrolimus based on clinical laboratory data.
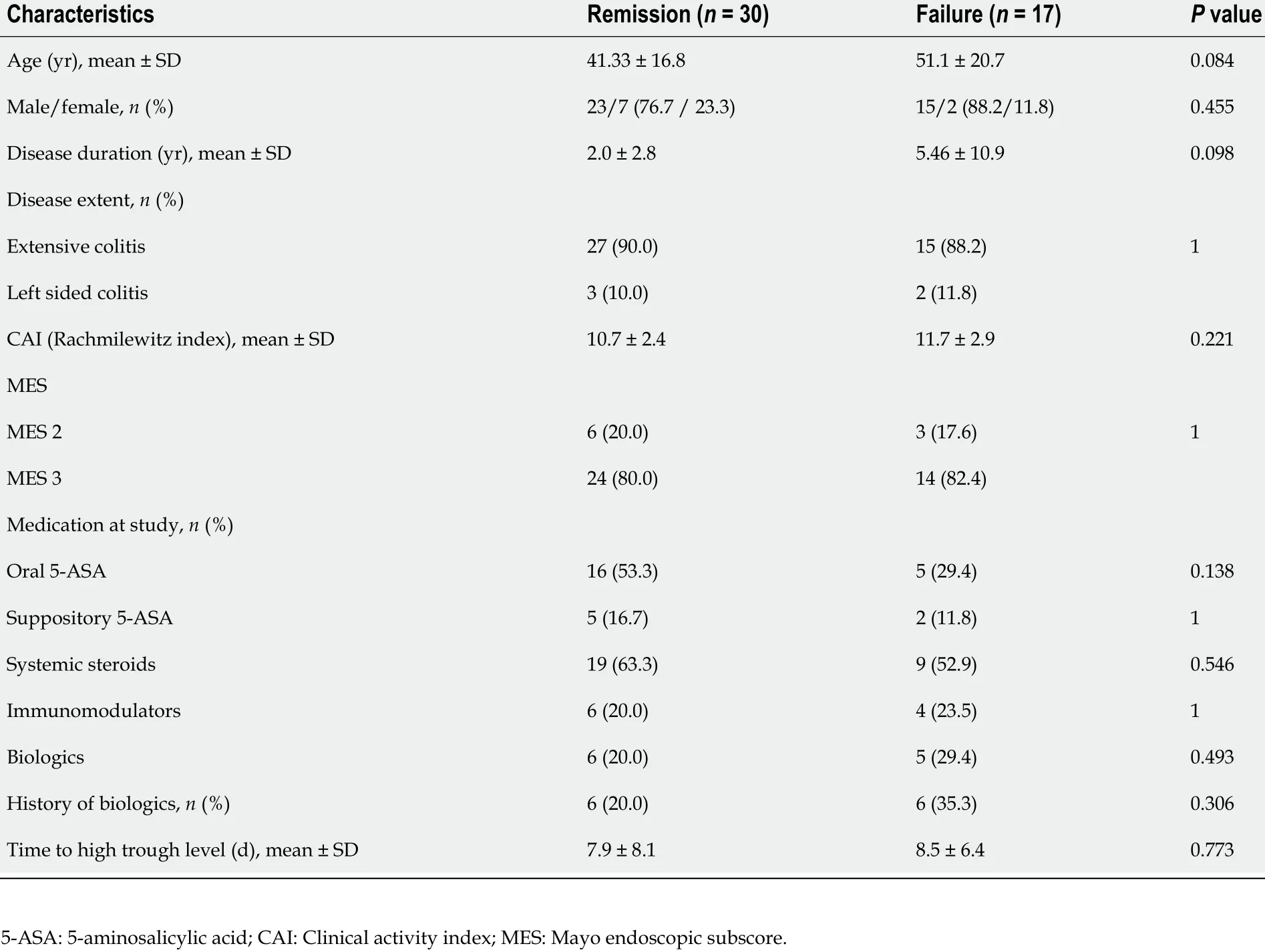
Table 2 Comparison between the failure and remission groups before tacrolimus induction
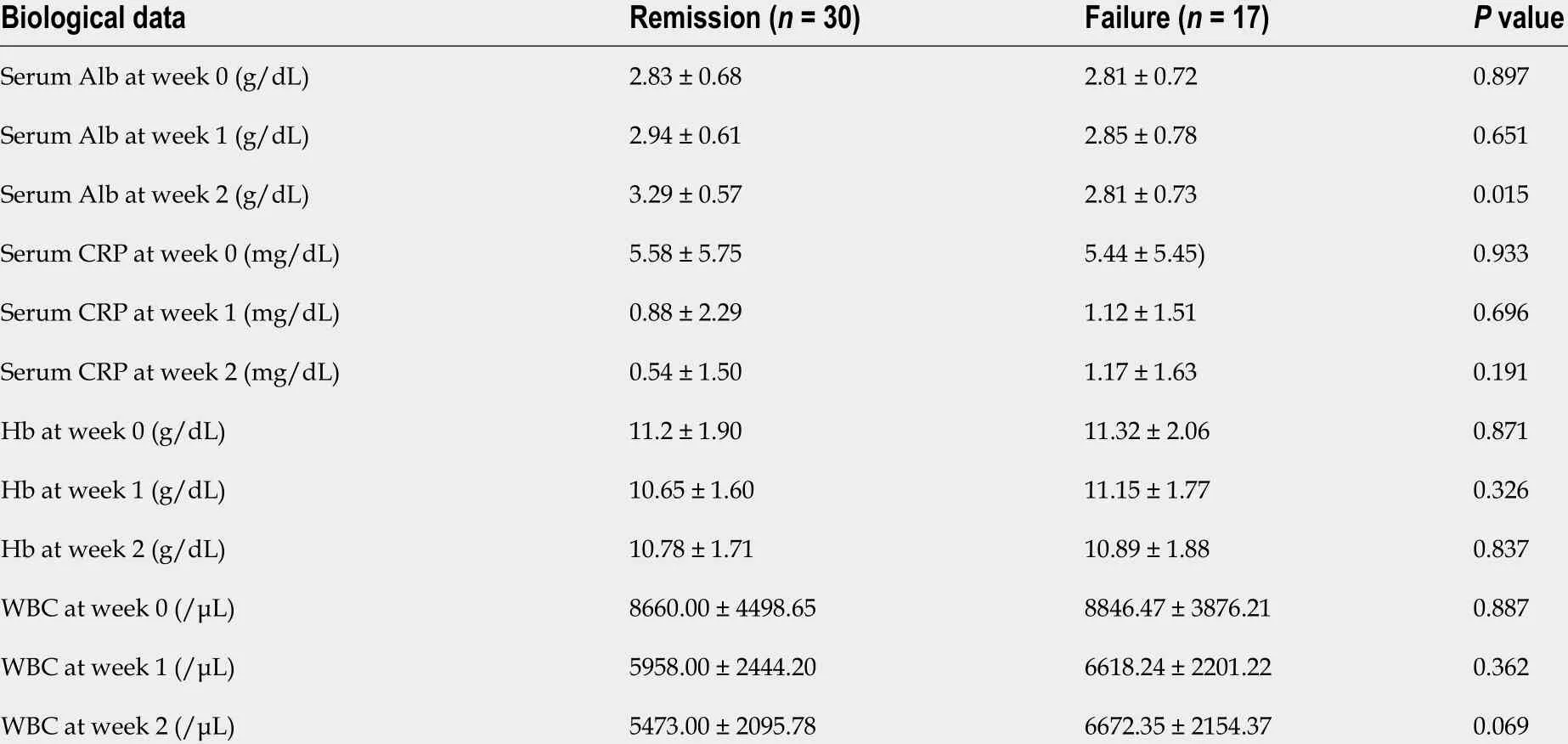
Table 3 Comparison of biological data before and after tacrolimus induction
In this study, we investigated the values of Alb, CRP, Hb, and WBC before the induction of tacrolimus (week 0 ) and at 1 - and 2 wk after achieving high trough levels(week 1 and week 2 , respectively). There was a significant difference in serum Alb levels at week 2 between the remission and failure groups, but there was no significant difference in CRP, a biomarker that reflects systemic or local inflammation. Since eachAlb value before the start of treatment varies with each patient, the ratio of week 1 Alb value or week 2 Alb value divided by week 0 Alb value was calculated in this study.As a result, the week 2 /week 0 Alb ratio showed a significant difference between the remission and failure groups. In the treatment of ulcerative colitis with tacrolimus, a sufficient therapeutic effect is exhibited, and mucosal healing is induced, by promptly reaching the effective range of blood concentration after the start of tacrolimus treatment. Therefore, in cases in which tacrolimus is effective, albumin is elevated because leakage of albumin from the intestinal tract is limited by mucosal healing.However, mucosal healing is not achieved in patients in whom tacrolimus is ineffective; therefore, it is thought that albumin loss from the intestinal tract persists and hypoalbuminemia does not improve. Although not shown in the data, the clinical activity index, which evaluated bloody stools and diarrhea, showed a greater improvement from week 0 to week 2 in the non-failure group than in the failure group.
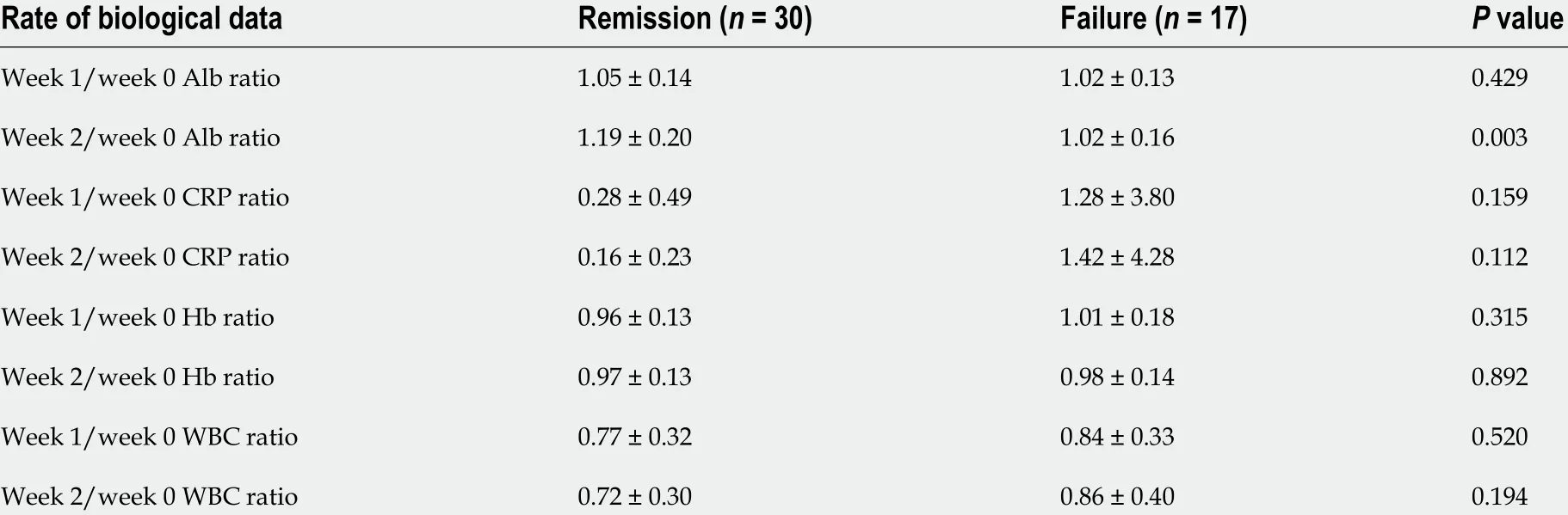
Table 4 Comparison of biological data ratio after tacrolimus induction
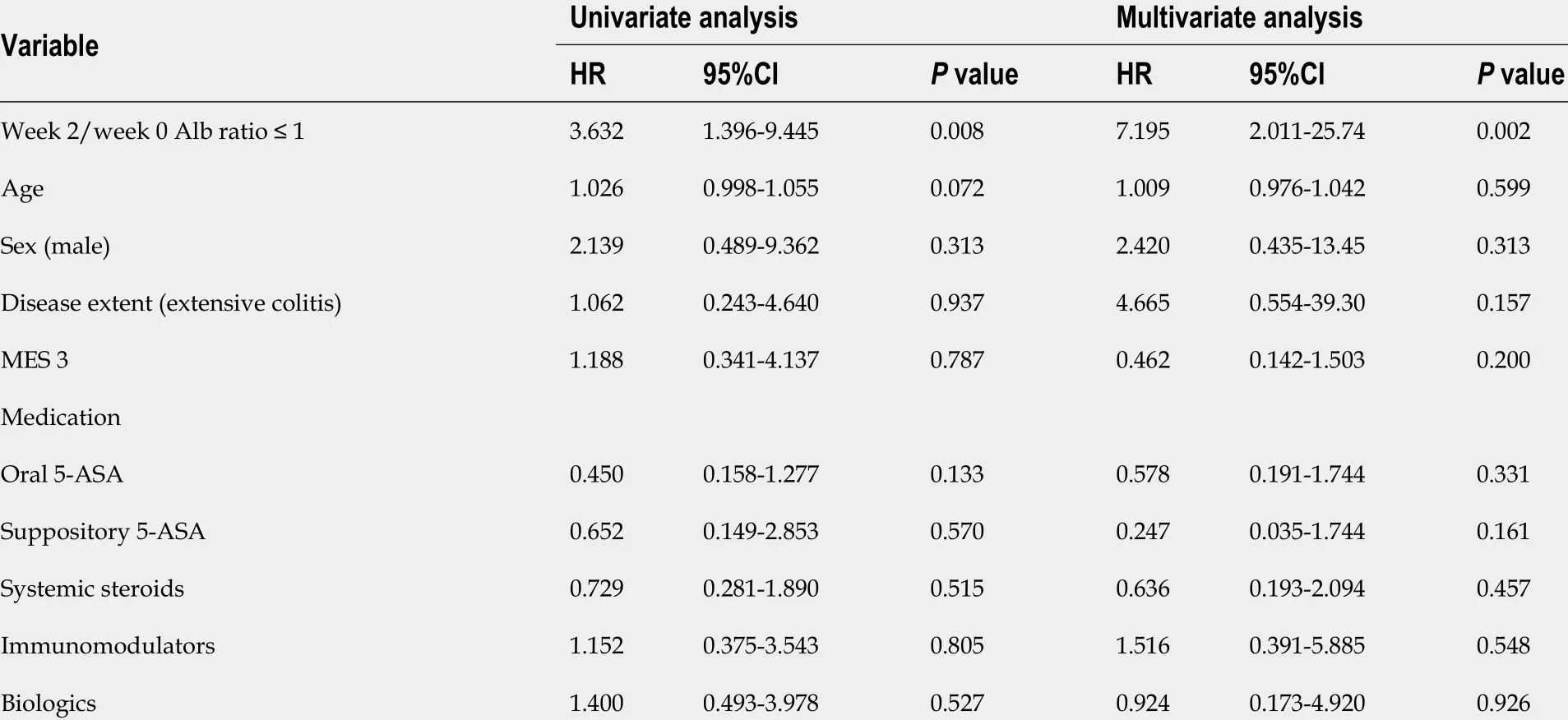
Table 5 Multivariate analysis for predicting failure during 3 mo after tacrolimus induction
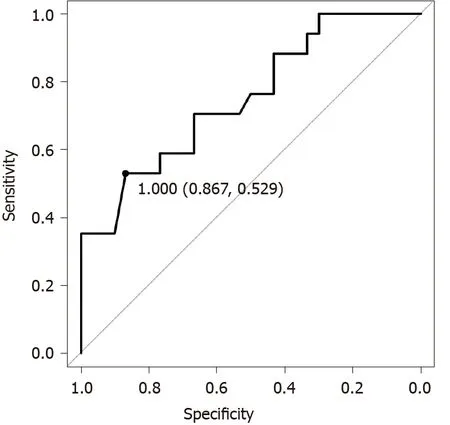
Figure 1 Receiver-operating characteristic analysis for prediction of failure during 3 mo after the reach of tacrolimus high trough level.
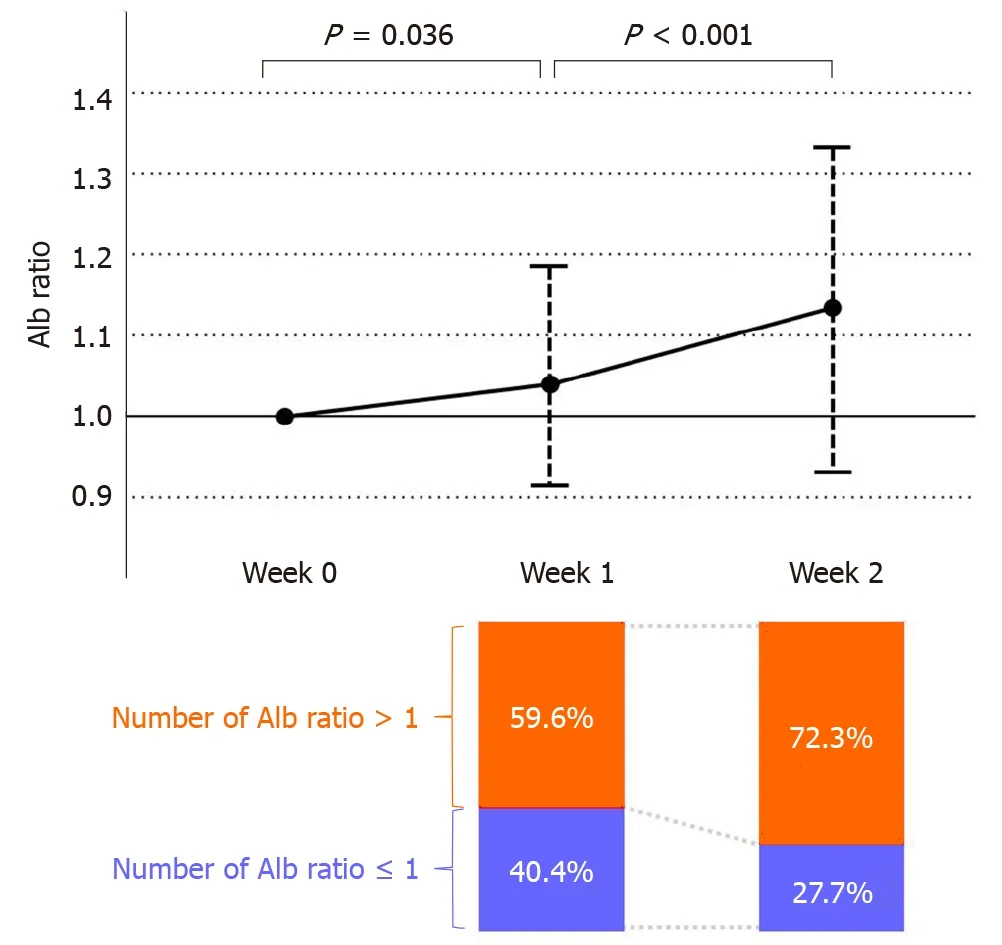
Figure 2 Changes in serum albumin ratio of each week and the percentage of the number of serum albumin ratio > 1 and ≤ 1 . Serum albumin (Alb) ratio at week 1 and week 2 shows the week 1 /week 0 and week 2 /week 0 Alb ratio, respectively. The percentage of the number of Alb ratio > 1 and ≤ 1 at week 1 and week 2 are shown in the bar graph.
We considered the factors leading to the significant difference in the Alb value by week 2 between groups; however, no significant difference was shown in Week 1 . As shown in Figure 2 , a significant increase in the Alb ratio was observed from Week 0 to Week 1 , and a further significant increase was observed from Week 1 to Week 2 overall. Furthermore, as a result of examining the proportion of patients with an Alb ratio of 1 as the cut-off value in weeks 1 and 2 , patients with an Alb ratio ≤ 1 (patients whose Alb value did not change or decrease in week 1 compared to week 0 ) comprised 40 .4 %, which was close to half. The reason for this may be that frequent diarrhea and bloody stools before the administration of tacrolimus may cause intravascular dehydration, resulting in higher Alb levels in blood. However, it was considered that after starting treatment, blood might have been diluted due to intravenous hydration in many patients, resulting in a temporary decrease in Alb levels. For this reason, the Alb level tends to decrease temporarily after the start of treatment, so it is too early to evaluate the Alb level by week 1 , and judgment at week 2 was considered to be appropriate.
Leeet al[28 ] reported that determination of Alb levels at week 2 was important for anti-TNF treatment in UC, which is similar to our analysis. This report showed that the Alb value 2 wk after the start of anti-TNF treatment was associated with primary nonresponse, endoscopic outcomes, time-to-colectomy, and anti-TNF failure.
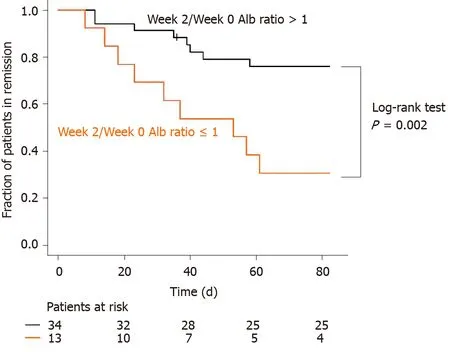
Figure 3 Kaplan-Meier time-to-relapse curve of patients with ulcerative colitis in relation to the week 2 /week 0 albumin ratio > 1 and ≤ 1 .
Several reports have attempted to predict the effect of tacrolimus on UC. Miyoshiet al[7 ] reported that colonoscopy evaluation 3 mo after remission induction with tacrolimus showed that groups with MES 0 and 1 had a better subsequent clinical course than the groups with MES 2 and 3 . In addition to this report, there have been several other reports on the treatment responsiveness and prognosis of tacrolimus on UC. In the report by Banet al[16 ], an analysis focusing on Alb was performed similar to that in our study. Their study also examined patients with UC who received calcineurin inhibitors, including cyclosporine and tacrolimus, and who underwent colectomy within 60 d of their remission induction. The study reported that the mean Alb levels of the early colectomy group and the non-early colectomy group before tacrolimus treatment were 2 .95 and 3 .41 , respectively, and that low Alb levels were a risk for early colectomy (P= 0 .0256 ). However, in our study, the mean Alb levels before the start of tacrolimus in the failure and remission groups were 2 .81 and 2 .83 ,respectively, showing no significant difference. The mean Alb levels before the induction of tacrolimus in all cases were 3 .3 and 2 .82 in the study by Ban et al[16 ] and the present study, respectively; however, more patients had hypoalbuminemia before the start of treatment in our institution. This seems to be the reason for the difference in the results between the two clinical studies. In our study, 17 of 47 patients had clinical failure during a 3 -mo follow-up, and the remission rate was 63 .8 %. Although there are differences in the observation period and the severity of enrolled patients,previous reports of the effects of tacrolimus on UC have reported a remission rate ranging from 9 .4 -75 .6 %[4 -8 ,21 -26 ,29 ].
In this study, even if the Alb level at week 0 was low, we could predict an effective remission if the albumin ratio was high in our study. Specifically, in the sub-group of Alb < 3 (n = 25 ), the week 2 /week 0 Alb ratio of the failure group was significantly higher than that of the remission group (P= 0 .003 ). In addition, a ROC analysis of the Alb < 3 sub-group showed a cut-off value of 1 .235 and AUC of 0 .853 with a 95 %CI of 0 .705 -1 .000 . We considered that the AUC of Alb < 3 was higher than the AUC of all cases because low Alb levels at Week 0 could be slightly increased after treatment improved the condition of UC.
Limitations
This study has several limitations. First, this is a single-center retrospective study with few enrolled patients. Second, we did not evaluate certain fecal biomarkers that have recently become widely used. Fecal biomarkers used in UC not only reflect endoscopic scores, but can also predict clinical relapse. There have been several recent reports on the usefulness of fecal calprotectin and fecal immunochemical occult blood test [30 -35 ]. However, it has not been verified whether these biomarkers are useful for evaluating the therapeutic effect and predicting prognosis in treatment using tacrolimus for UC, which is a subject for future research. In addition, this study evaluated Alb levels 2 wk after achieving high trough levels of tacrolimus as it is not beneficial for patients to postpone the decision to convert to surgical treatment beyond this time point. Indeed, early conversion to surgical treatment in steroid-refractory acute severe UC has been reported to improve postoperative prognosis[36 ,37 ].Conversely, prolongation of preoperative medical treatment for refractory cases has been reported to worsen the postoperative prognosis of UC[38 ,39 ]. Alternatively,switching to other biologics may not improve the condition of UC patients, but rather increase the risk of complications. Therefore, we thought that the prediction of the prognosis in moderate to severe UCviathe Alb ratio, as shown in this study, could be a supportive factor in determining the next treatment.
CONCLUSION
In conclusion, a lower Alb value in week 2 than in week 0 after achieving trough level of tacrolimus predicts clinical failure in patients with UC. In these cases, changes to other treatment options, including surgical total colectomy, should be considered as soon as possible.
ARTICLE HIGHLIGHTS
猜你喜欢
今日农业(2021年19期)2022-01-12
中华骨与关节外科杂志(2021年8期)2021-11-30
西安邮电大学学报(2021年6期)2021-05-10
电子产品世界(2021年6期)2021-02-10
中国现代医生(2020年2期)2020-04-09
中国外汇(2019年19期)2019-11-26
新西部下半月(2017年6期)2017-07-19
新课程·中旬(2017年2期)2017-03-29
 World Journal of Gastroenterology2021年22期
World Journal of Gastroenterology2021年22期
- World Journal of Gastroenterology的其它文章
- Role of imaging in evaluating the response after neoadjuvant treatment for pancreatic ductal adenocarcinoma
- High fecal calprotectin levels are associated with SARS-CoV-2 intestinal shedding in COVID-19 patients: A proof-of-concept study
- Liver injury in COVID-19 : Detection, pathogenesis, and treatment
- Enhancer of zeste homolog 2 contributes to apoptosis by inactivating janus kinase 2 / signal transducer and activator of transcription signaling in inflammatory bowel disease
- Interplay between nuclear factor erythroid 2 -related factor 2 and inflammatory mediators in COVID-19 -related liver injury
- Helicobacter pylori promotes invasion and metastasis of gastric cancer by enhancing heparanase expression