
Risk factors for overuse injuries in short-and long-distance running:A systematic reviewT
2021-02-03 07:08DennisvnPoppelMrtenvnerWorpAnoukSlekoornSylvivnenHeuvelMrienkevnMielkoopBrtKoesArinneVerhgenGwenolyneSholtenPeetersgT
Dennis vn Poppel*,Mrten vn er Worp,Anouk Slekoorn,Sylvi S.P.vn en Heuvel,Mrienke vn Mielkoop,Brt W.Koes,e,Arinne P.Verhgen,,f,Gwenolyne G.M.Sholten-Peeters,gT
aResearch Group Diagnostics,Avans University of Applied Sciences,Breda,4818 CR,the Netherlands
bStichting Academie Instituut Fysiotherapie PLUS,Utrecht,3581 MD,the Netherlands
cNederlands Paramedisch Institute,Amersfoort,3818 LA,the Netherlands
dDepartment of General Practice,Erasmus MC Medical University Center,Rotterdam,3015 CE,the Netherlands
eCenter for Muscle and Joint Health,University of Southern Denmark,Odense,5230,Denmark
fDiscipline of Physiotherapy,Graduate School of Health,University of Technology,Sydney,Chippendale NSW 2008,Australia
gDepartment of Human Movement Sciences,Faculty of Behavioral and Movement Sciences,Vrije Universiteit Amsterdam,Amsterdam,1081 HV,the Netherlands T
Received 17 February 2020;revised 25 March 2020;accepted 4 May 2020 Available online 12 June 2020
2095-2546/©2021 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/)
Abstract Purpose:The aim of this study was to review information about risk factors for lower extremity running injuries in both short-distance(mean running distance≤20 km/week and≤10 km/session)and long-distance runners(mean running distance>20 km/week and>10 km/session).Methods:Electronic databases were searched for articles published up to February 2019.Prospective cohort studies using multivariable analysis for the assessment of individual risk factors or risk models for the occurrence of lower extremity running injuries were included.Two reviewers independently selected studies for eligibility and assessed risk of bias with the Quality in Prognostic Studies Tool.The GRADE approach was used to assess the quality of the evidence.Results:A total of 29 studies were included:17 studies focused on short-distance runners,11 studies focused on long-distance runners,and 1 study focused on both types of runners.A previous running-related injury was the strongest risk factor for an injury for long-distance runners,with moderate-quality evidence.Previous injuries not attributed to running was the strongest risk factor for an injury for short-distance runners,with high-quality evidence.Higher body mass index,higher age,sex(male),having no previous running experience,and lower running volume were strong risk factors,with moderate quality evidence,for short-distance runners.Low-quality evidence was found for all risk models as predictors of runningrelated injuries among short-and long-distance runners.Conclusion:Several risk factors for lower extremity injuries have been identi fied among short-and long-distance runners,but the quality of evidence for these risk factors for running-related injuries is limited.Running injuries seem to have a multifactorial origin both in short-and long-distance runners.
Keywords:Musculoskeletal health;Protective factors;Running-related injury
1.Introduction
Running is one of the most popular physical activities around the world to achieve or maintain better physical health.1In the last 10 years,the number of runners has doubled,and this number is still increasing.2Running is bene ficial for the whole body:it improves endurance,decreases the risk of cardiovascular diseases and helps to lose weight.3,4Unfortunately,running is also associated with a high risk of injuries,especially in the lower extremities.5About 80%of runningrelated injuries(RRIs)are related to overload.6,7Tendons and ligaments mainly are at risk due to the relatively slow adaptation to training load.7
Because there are many different injury de finitions and running types,the incidence of RRIs varies considerably.8,9Runners have a high risk of getting injured,with incidence rates ranging from 7.7 to 17.8 per 1000 h of running.6The incidence of running injuries differs between different running distances.Short-distance runners(those who run 15 km or less)have an incidence ranging from 14.3%to 44.7%while longdistance runners(those who run half-marathons or marathons)seem to have more injuries(16.7%-79.3%).10
Several risk factors for RRIs have been identi fied.11,12These risk factors can be divided into personal factors(e.g.,age,weight,height),training-related factors(e.g.,distance,frequency,intensity,shoes),and health-related factors(e.g.,medication,previous injury,use of alcohol).10According to recent systematic reviews(SRs),a previous injury is the most important risk factor in short-and long-distance runners.10,12The use of orthotic inserts in shoes and hip abductor weakness are associated with an increased injury risk as well.10-13Inconsistent findings were found for other risk factors,such as body mass index(BMI),14-16age,15,17and training distance.18-20Nonetheless,none of these risk factors have been conclusively found to be the cause of a particular RRI.Also particular injuries may not be related to a single risk factor,but instead are the result of an interaction among several risk factors.
Previous studies have indicated that risk factors vary for different populations of runners.10,12,16For instance,it seems that inexperienced runners are twice as likely to get injured compared to experienced runners and that men and women have different risk pro files.9,10,21In addition,studies conducted on short-distance runners reveal that their risk factors differ from those of marathon runners.22,23For example,a study showed that short-distance runners seem to be at higher risk of injury when they have a BMI of greater than 30,have an age range between 45 and 65 years,exhibit non-competitive behaviors and have experienced a previous injury.22However,other studies found that long-distance runners seem to be at higher risk for a RRI when their BMI is greater than 26 and when they have had a previous injury.But for these runners,older age,interval training,and running more training kilometers per week were found to be protective.19,23,24
Because personal,training-related,and health-related factors such as age,ratio of female/male runners,kilometers of running per week,and running experience differ between short-and long-distance runners,22-24we hypothesize that risk factors for short-and long-distance RRIs will also differ between these groups.
None of the previous reviews explicitly address these differences in short-and long-distance recreational runners or describe separate risk factors for short-and long-distance runners as they relate to RRIs.Moreover,none of the SRs used the Grading of Recommendations Assessment,Development,and Evaluation(GRADE)approach to judge the overall quality of evidence or included both individual risk factors and risk models for short-and long-distance RRIs.
To develop injury prevention strategies for recreational runners,identifying risk factors is important.25If risk factors vary per distance,injury prevention strategies between short-and longdistance runners should be different.Therefore,the aim of this SR was to evaluate risk factors for lower extremity running injuries for short-and long-distance recreational runners separately.
2.Methods
2.1.Protocol and registration
This review was prospectively registered with PROSPERO(registration number CRD42019133799)and was written in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)guidelines.26
2.2.Data sources and search procedure
Electronic searches were performed by a librarian(SvdH),from inception until February 2019,in PubMed,CINAHL,Cochrane Library,SPORTDiscus,and PsychINFO,using MESH terms and free-text words.To identify relevant studies,several terms related to RRIs were used(Supplementary Table 1).Terms used to search for factors related to study design were:“cohort”,“prospective”,“observational”,and “longitudinal”.Details of the search strategy are available in Supplementary Table 1.References in the included articles were checked for relevant papers.
2.3.Study selection
Studies were included or excluded if they met the selection criteria reported in Supplementary Table 2.Two reviewers(AS and MvdW)independently screened titles and abstracts using the selection criteria.Full-text articles of all the selected studies were retrieved and independently assessed by the 2 reviewers,who applied the selection criteria(Supplementary Table 3).Disagreement was resolved by consensus.When no consensus could be reached,a third reviewer(DvP)made the final decision.
2.4.Risk of bias assessment
All risk factor studies were assessed for risk of bias(RoB)by 2 reviewers independently(MvdW and AS)using the Quality in Prognostic Studies(QUIPS)tool.27For risk model studies,RoB was determined using the Prediction model Risk Of Bias Assessment Tool(PROBAST).28Disagreement was resolved by consensus.A third reviewer(DvP)made the final decision in cases where no consensus could be reached.
2.5.Data collection and processing
The following data were extracted from the included studies:year of publication,follow-up period,population characteristics(age,BMI,or weight and height,sex),running distance,number of participants included and number of participants analyzed,the de finition of an injury,number of RRIs,the type of injury and risk factors,and whether or not the studies evaluated a risk model and adjusted for confounders.The data were processed in a data extraction table.All studies were classi fied as short-distance (mean running distance of≤20 km/week and≤10 km/session)or long-distance(mean running distance of>20 km/week and>10 km/session).If kilometers per week con flicted with kilometers per session,for instance,40 km/week with a frequency of 5 times/week,it was classi fied according to kilometers per week.In case the study population consisted of only males(or females),or when the results in a mixed population were analyzed separately,the results for males and females were also described separately.
Risk factors presented in each study were extracted and categorized as personal,training-related or health-related factors,for short-distance runners and long-distance runners separately.Outcome data for risk models were extracted,including betas,odds ratios(OR),relative risk ratios,hazard ratios and explained variance,or area under the curve.The results per potential risk factor are presented in following subgroups:general(if no subgroups in sex were made),male,and female.
2.6.Outcome
The main outcome variable was a RRI,de fined as“selfreported musculoskeletal complaints,in the lower extremity,caused by running activities”.23
2.7.Data synthesis
We summarized the findings in tables, figures,and text and distinguished 3 categories for the short-and long-distance recreational runners:males,females,and the total general group.A meta-analysis could not be performed due to clinical heterogeneity with respect to population and de finition of outcome(s).Cohen’sKwas used to determine the interobserver agreement of the RoB assessment.
The GRADE approach was used to categorize the overall quality of evidence into high,moderate,low,and very low quality.This categorization provides insight into the con fidence of the estimate of the effect.In the field of prognosis,longitudinal cohort studies initially provide high-quality evidence and can be downgraded or upgraded.29-35
Six study characteristics downgrade the quality of evidence(phase of investigation,study limitations,inconsistency,indirectness,imprecision,and publication bias).Two study characteristics upgrade the quality of evidence:(1)large(OR>2 or<0.5)or very large(OR>5 or<0.2)effect size and(2)exposure-response gradient.29-35Concerning study limitations,the evidence was downgraded when more than 75%of the participants were in low RoB studies.Limitations regarding imprecision were determined by the width of the 95%con fidence interval and sample size(n=2000-4000).32Limitations in indirectness were reported when the outcome variable was not fully appropriate(e.g.,when an outcome was not general for RRIs but was speci fic to patellar femoral pain syndrome)or when study populations differed.34Inconsistency was present if the direction of effect differed(protectivevs.risk factor,or no effect)between studies or when differences in risk estimates were found.33Last,the evidence was upgraded when more than 75%of the participants were found to have very large effect sizes(OR>5 or<0.2).35Single studies(n<4000)are initially rated as low-quality evidence because of downgrading by inconsistency and imprecision.32,34
If most of the studies regarding a speci fic risk factor,including more than 50%of the participants,found no significant association,results were described as evidence for not being a risk factor.If most of the studies,including more than 50%of the participants,found a significant association,a potential factor is described as a risk factor or a protective factor,depending on the association that was found.
3.Results
3.1.Study selection
A total of 1300 hits were identi fied from the electronic search of the literature,and 1 article was retrieved from the reference lists in the articles identi fied.A total of 53 duplicates were removed,and 1163 articles were excluded based on a review of titles and abstracts.Of the remaining 85 hits,49 articles were excluded based on full-text screening,7 articles were not full-text available.Finally,29 studies with a total of 18,853 participants were included in this review;25 studies presented risk factors(single factor studies)and 4 studies presented risk models(risk model studies)(Fig.1).
3.2.RoB assessment
The RoB in the domains “outcome measurement”and“prognostic factor measurement”was low.The domains“study attrition”and “study confounding”showed the highest RoB,mainly due to insuf ficient reporting(Table 1,Fig.2).TheKfor the overall interobserver agreement(using the QUIPS)between the 2 reviewers was 0.80(95%con fidence interval:0.75-0.83).
According to the PROBAST,3 risk model studies23,24,36had a low RoB and good applicability.One risk model study19had problems with the applicability because only male runners were included.
3.3.Study characteristics
3.3.1.PopulationTaggedEd
Seventeen studies examined risk factors(single-factor studies)in short-distance runners;14-16,20,22,37-48no risk model studies were found for short-distance runners.Eight studies examined risk factors(single-factor studies)for long-distance runners,49-56and three were risk model studies.19,23,36One study examined short-and long-distance runners in a risk model study.24Tables 2,3,and 4 describe the characteristics of the included studies.
3.3.2.Follow-up
In studies involving short-distance runners,the follow-up period ranged from 6 weeks to 1 year.The proportion of analyzed participants ranged from 69%to 100%of the included participants at baseline.In studies involving long-distance runners,the follow-up period ranged from 4 weeks to 2 years.The proportion of analyzed participants ranged from 67%to 100%of the included participants at baseline.
3.3.3.Risk factors
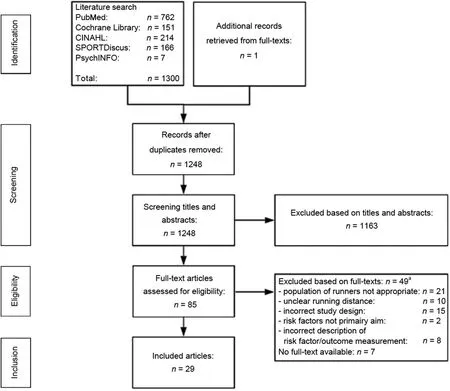
Fig.1.Flowchart of the literature search.aSome articles were excluded for more than 1 reason.
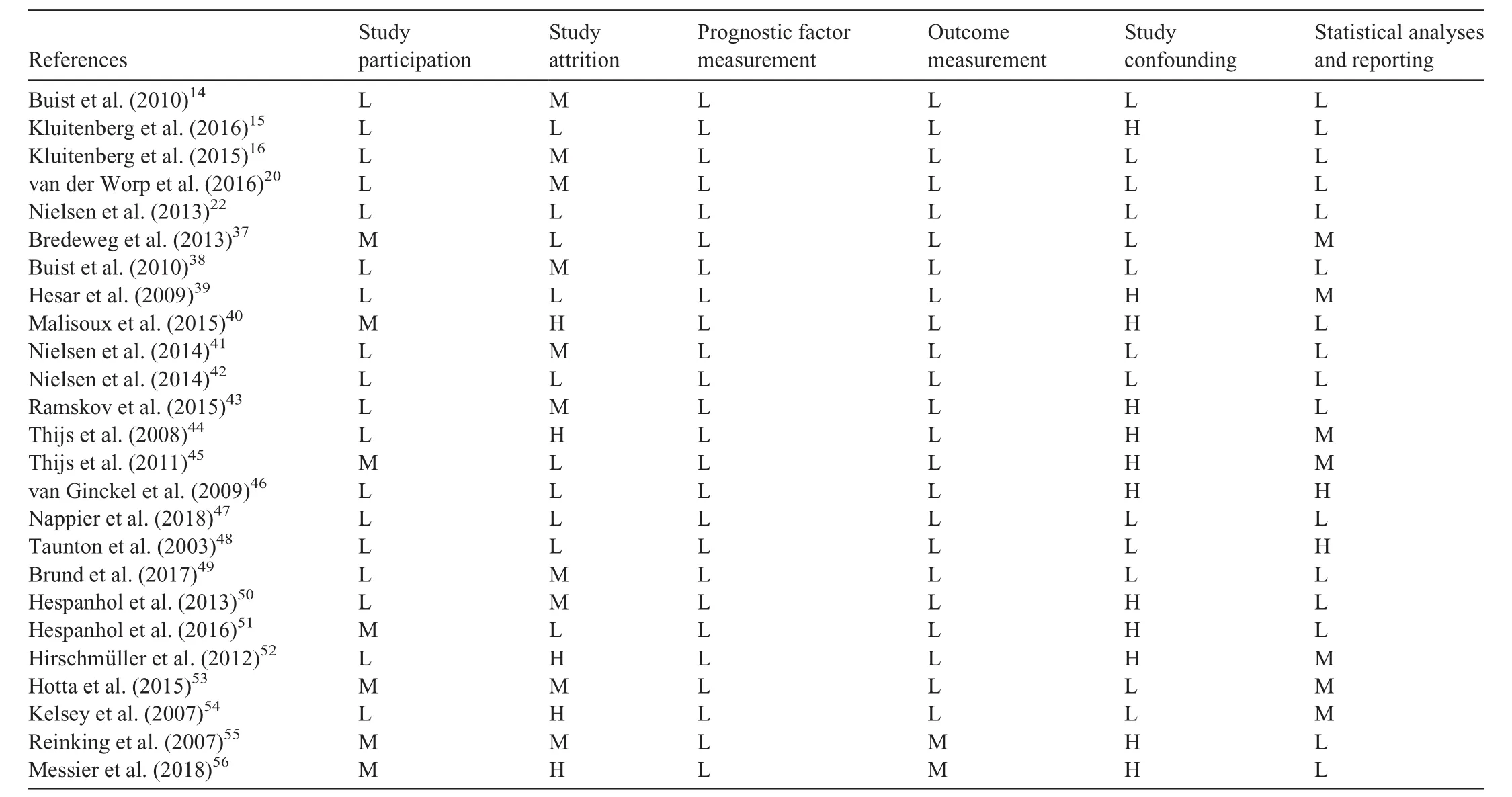
Table 1 Rating for individual studies.
A total of 38 potential risk factors were analyzed for short-distance runners,and 36 were analyzed for long-distance runners(Table 5 and Supplementary Tables 4-6).The overall results(GRADE approach)for risk factors for short-and long-distance runners are summarized in Supplementary Table 7.Risk factors evaluated in more than 1 study are described in the text.
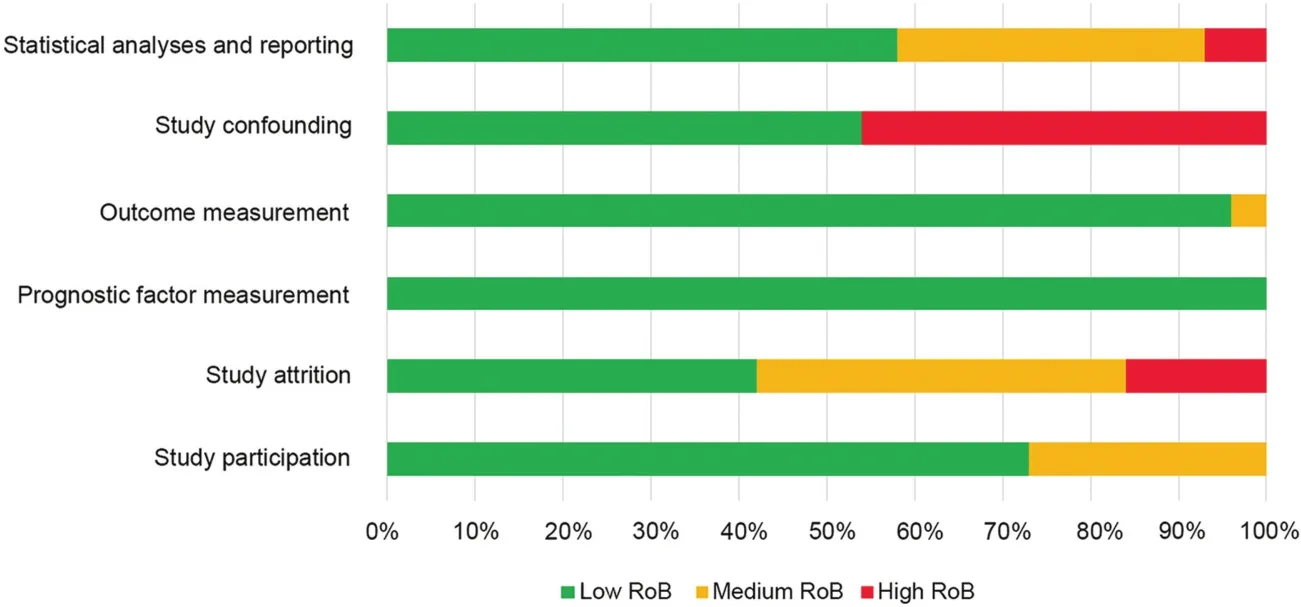
Fig.2.Risk of bias(RoB).
3.3.3.1.Short-distance runners
3.3.3.1.1.Personal factorsT
3.3.3.1.1.1.Age
Six studies evaluated age as a potential risk factor.14,16,20,22,38,48In a generic population,2 studies(low RoB)found no association,20,22and 1 study(low RoB)found higher age to be a risk factor(hazard ratio=1.02).16There is therefore moderate quality evidence(downgraded for inconsistency)for age being a risk factor for RRIs.
One study(low RoB)found older age to be a protective factor for injuries in male runners.38In a female population,2 studies(low RoB)found no association.14,38One study(medium RoB)found older age to be a risk factor.48In males,there is low quality evidence(single study,downgraded for inconsistency and imprecision)that older age is a protective factor,while in females we found low quality evidence(downgraded for limitations in design and inconsistency)that age is not a risk factor.
3.3.3.1.1.2.BMI
Six studies evaluated BMI as a potential risk factor.14,16,20,22,38,48In a generic population,2 studies(low RoB)found no association20,22and 1 study(low RoB)found higher BMI to be a risk factor.16We found moderate quality evidence(downgraded for inconsistency)for BMI being a risk factor.One study(low RoB)found higher BMI to be a risk factor for injuries in female runners.38In a male population,1 study(low RoB)found no association,371 study(low RoB)found higher BMI to be a risk factor,14and another study(medium RoB)found higher BMI(>26 kg/m2)to be a protective factor.48In females,we found low-quality evidence(single study,downgraded for inconsistency and imprecision)that higher BMI is a risk factor,and low quality evidence(downgraded for limitations in design and inconsistency)for BMI as a risk factor in male short-distance runners.
3.3.3.1.1.3.Running experience
Four studies evaluated previous running experience.16,20,22,38In a generic population,2 studies(low RoB)found no association.20,22One study(low RoB)found no running experience to be a risk factor for RRIs.16We found moderate quality evidence(downgraded for inconsistency)that having no previous running experience is a risk factor for RRIs.
One study(low RoB)found a significantly higher risk of injury in male and female runners when they had no previous running experience.38We found low quality evidence(single study,downgraded for inconsistency and imprecision)that having no previous running experience is associated with an increased injury risk in male and female runners.
3.3.3.1.1.4.Previous sports activity
A type of previous sports activity was included as a risk factor in 6 studies.14,16,20,22,38,48In a generic population,no association was found.16,20,22We found high quality evidence that previous sports activity is not associated with RRIs.
One study(low RoB)found a significantly higher injury risk in males when previous sports activities without axial loading were performed,141 study(low RoB)found no association in males but a higher injury risk in females,38and 1 study(medium RoB)did not provide data.47We found low quality evidence(single study,downgraded for inconsistency and imprecision)for previous sports activity being a risk factor for RRIs in females and males.
3.3.3.1.1.5.Behavior
Competitive/hyperactivevs.relaxed/laid back behavior was included as a risk factor in 2 studies,14,221 in a generic population,22and 1 in males only.14One study(low RoB)found behavior(relaxed/laid back)to be a significant risk factor;22the other study(low RoB)found no association in males.14We found low quality evidence(single study,downgraded for inconsistency and imprecision)that behavior was a risk factor for RRIs in a generic population,and low quality evidence(single study,downgraded for inconsistency and imprecision)for behavior not being a risk factor in men.
Four studies included foot morphology(plantar arch index,naviculardrop,orfootpronation)asa potentialrisk factor.14,20,42,48Two studies(low RoB)were performed in the generic population.20,42One study found no significant association,20and the other study revealed that runners with pronated feet had significantly fewer RRIs per 1000 km of running compared to runners with normal feet.42We found low quality evidence(downgraded for inconsistency and imprecision)for foot morphology(moderate foot pronation)not being a risk factor for RRIs.
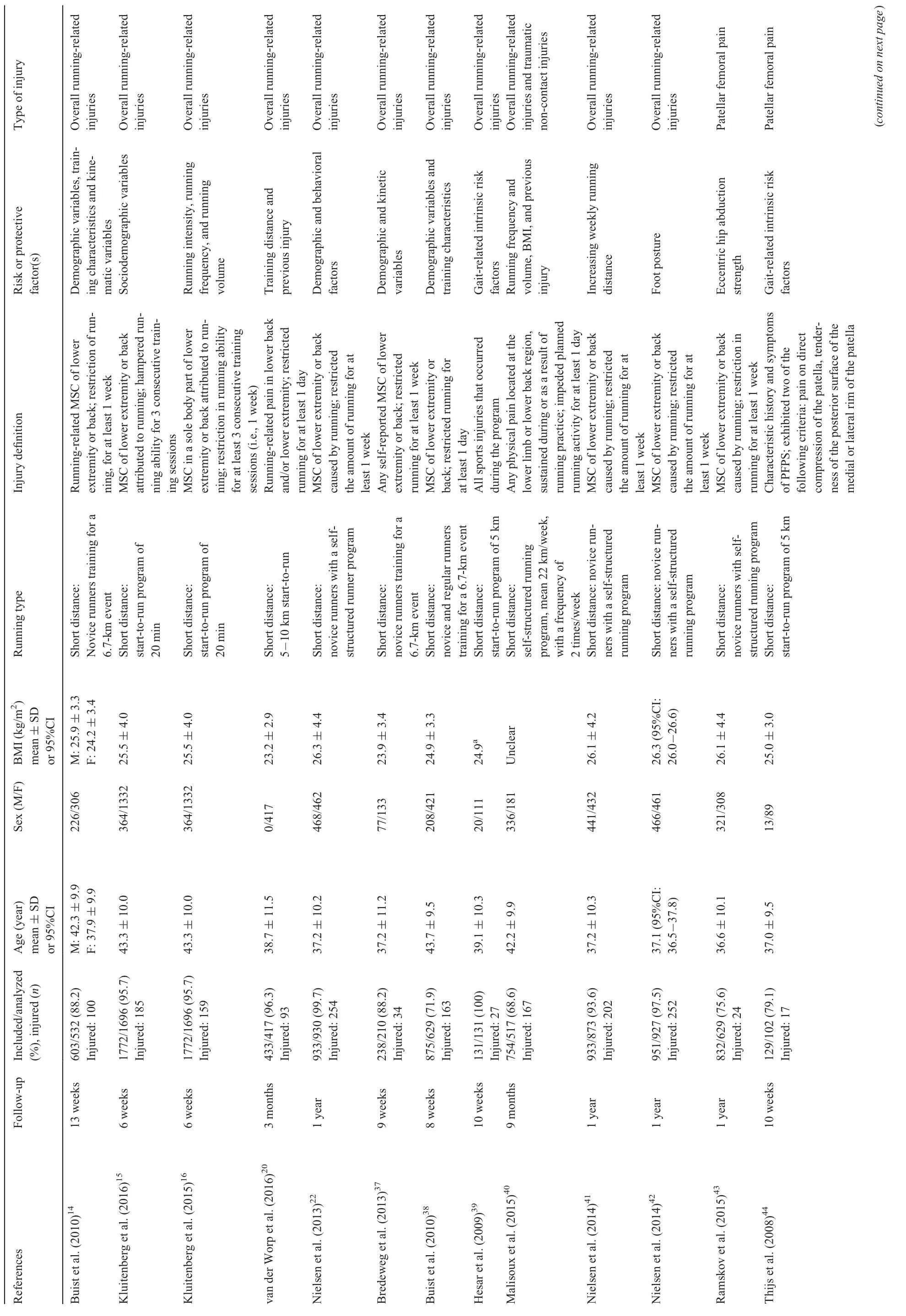
Table 2 Description of participants, injury type, and definition and risk factors in single-factor studies involving short-distance runners.
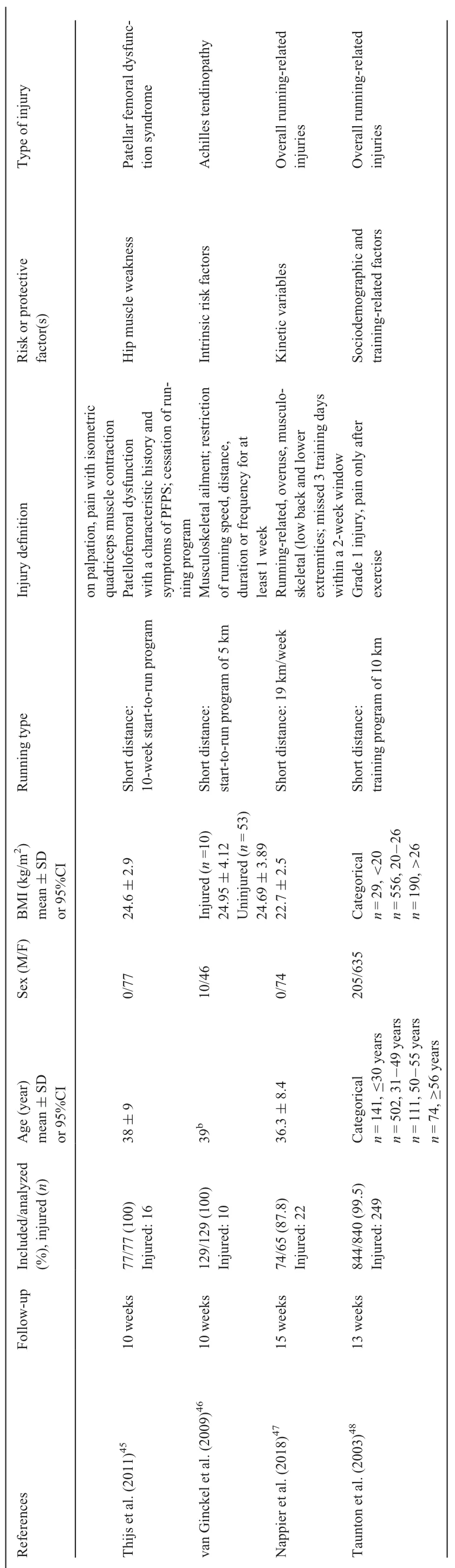
Table 2 (Continued)
One study(medium RoB)did not present data on the plantar arch as a possible risk factor.48One study(low RoB)found that normal navicular drop was a protective factor for RRIs compared to a high navicular drop in female runners.14We found low quality evidence(single study,downgraded for inconsistency and imprecision)for foot morphology(normal navicular dropvs.increased navicular drop)as a protective factor for RRIs in females.
3.3.3.1.2.Training-related factors
3.3.3.1.2.1.Running frequency
Three studies included running frequency as a potential risk factor.15,40,48In a generic population,2 studies(medium and high RoB)found no association for running frequency and RRIs in the generic population.15,40We found moderate quality evidence(downgraded for study limitations)for running frequency not being a risk factor for RRIs.One study(medium RoB)found that running 1 day/week or less is associated with an increased risk for RRIs in females.We found very low quality evidence(single study,downgraded for study limitations,inconsistency and imprecision)for running frequency as a risk factor for RRIs in females.48
3.3.3.1.2.2.Weekly running volume
Two studies included weekly volume(min/week)as a potential risk factor.15,40One study(medium RoB)found a weekly volume of more than 60 min to be a protective factor,15and the other study(high RoB)found a weekly volume of less than 2 h to be a risk factor for injuries.40We found moderate quality evidence(downgraded for study limitations)that lower weekly training volume is a risk factor.
3.3.3.1.2.3.Weekly running distance
Two studies included weekly running distance as a potential risk factor.20,41One study(low RoB)found no association between weekly running distance and injuries,41while 1 study(low RoB)found a higher running distance(>30 km/week)to be a risk factor for RRIs.We found low quality evidence(downgraded for inconsistency and imprecision)for running distance as a risk factor.
3.3.3.1.2.4.Type of terrain
Two studies included type of terrain as a potential risk factor.20,48One study,using a generic population(low RoB),found no significant association between type of terrain and injuries in short-distance runners.20We found low quality evidence(single study,downgraded for inconsistency and imprecision)that type of terrain is not a risk factor.The other study reported no data on this risk factor.48
3.3.3.1.2.5.Running shoe age
Three studies included running shoe age as a potential risk factor.16,20,48Two studies found no association16,20in a generic population.We found high quality evidence that running shoe age is not a risk factor for RRIs.One study(medium RoB)found running shoe age(4-6 months old)(compared to 1-3 months,7-12 months,or 1-2 years old)to be a protective factor in male runners and a risk factor in female runners.48There is very low quality evidence(single study,downgraded for limitations in design,inconsistency,and imprecision)that running shoe age is a protective factor in male runners and a risk factor for RRIs in female runners.

Table 3 Description of participants, injury type and definition, and risk factors in single-factor studies involving long-distance runners.
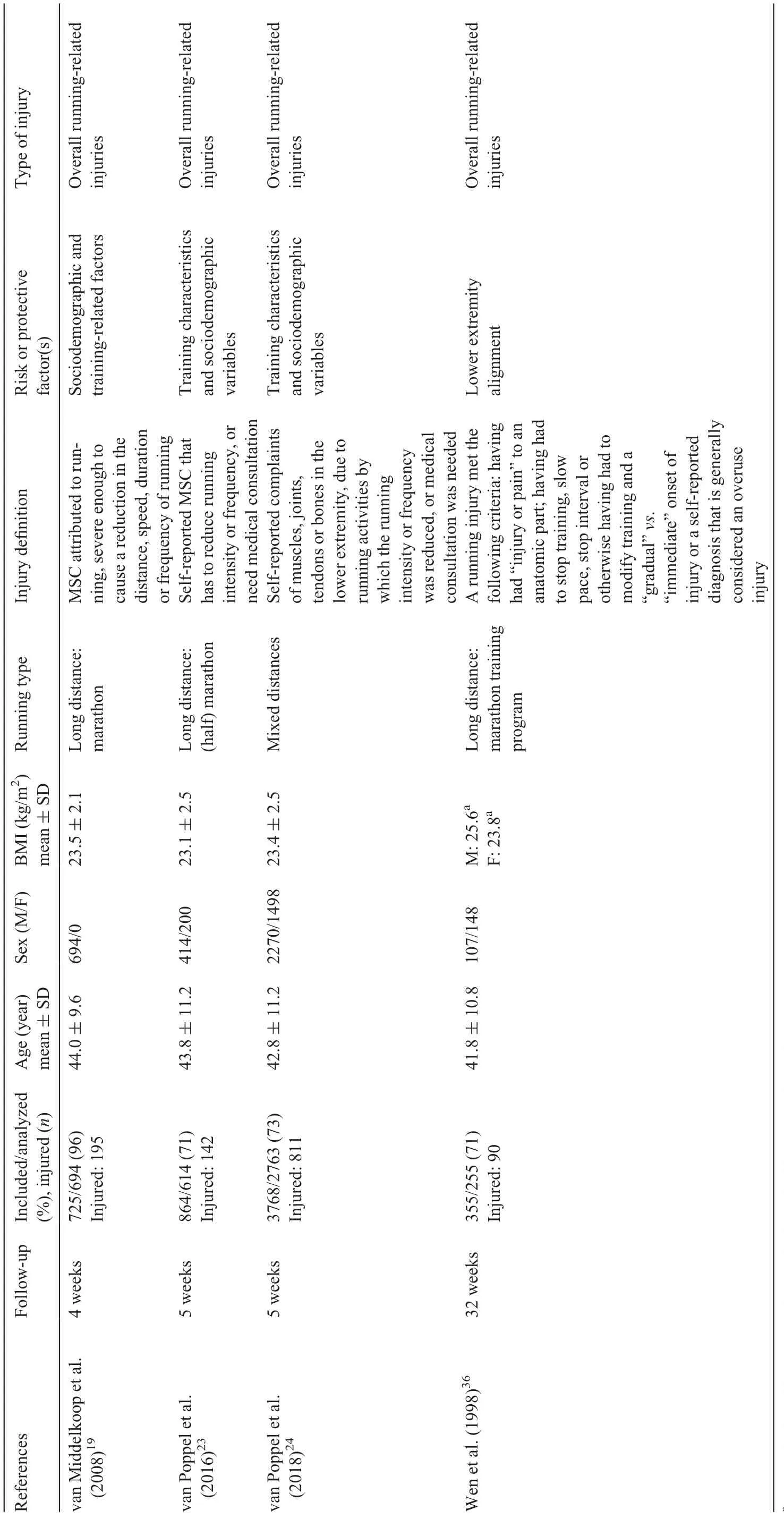
Table 4 Description of participants, injury type and definition, and risk factors in risk model studies involving short- and long-distance runners.
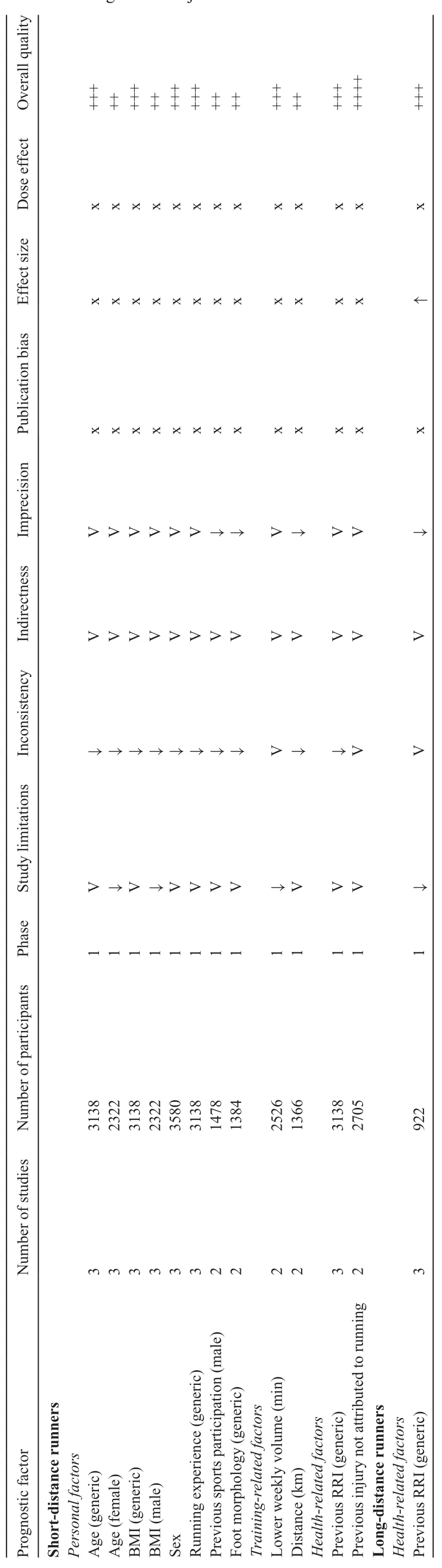
Table 5 Grading assessment quality of evidence (GRADE) summary table of the most important significant risk factors in 2 or more studies.
3.3.3.1.2.6.Hip strength
Two studies included hip abduction strength as a potential risk factor.43,45One study(medium RoB)in a generic population found hip abduction strength to be a risk factor for RRIs(very low quality evidence)(single study,downgraded for study limitations,inconsistency,indirectness,and imprecision).43The other study(high RoB)did not present data on this association.45
3.3.3.1.2.7.Intrinsic gait-related factors
Three studies included intrinsic gait-related factors as risk factors.38,44,46All 3 studies assessed different kinds of risk factors.One study(high RoB)found significantly more laterally directed force distribution underneath the forefoot at the forefoot flat and significantly decreased total displacement of the center of force(COF)to be risk factors for the development of Achilles tendinopathy.39
One study(medium RoB)found that force distribution was significantly more laterally directed at first metatarsal contact and at forefoot flat.39Furthermore,the mediolateral force ratio showed more displacement of the force from medial to lateral in the initial contact phase.During the forefoot contact phase and the foot flat phase,the COF was more laterally directed in the injured group.At heel-off,the x-component of the COF is situated significantly more laterally.During the forefoot pushoff phase,the x-component of the COF is situated significantly more medially.The velocity of the mediolateral and the anteroposterior displacement of the COF at forefoot flat was significantly slower.Anteroposterior displacement of the COF at forefoot flat was significantly higher in the injured group.The absolute force time integral underneath metatarsal 5 was significantly higher in the participants who sustained an RRI.46One study(high RoB)found a significantly shorter time to the vertical peak force underneath the lateral heel to be a predisposing factor for patellofemoral pain syndrome,but no risk estimates were presented.44
In conclusion,there is very low quality evidence based on single studies(downgraded for study limitations,inconsistency,indirectness,and imprecision)that intrinsic gait-related factors are risk factors for RRIs.
3.3.3.1.2.8.Peak force
Two studies included active peak of ground reaction force as a potential risk factor.37,47One study(moderate RoB)published no data on this positive association,37and 1 study(low RoB)found no association in females.47We found low quality evidence(single study,downgraded for inconsistency and imprecision)that active peak is not a risk factor for RRIs in a female population.
3.3.3.1.3.Health-related factorsT
3.3.3.1.3.1.Previous RRIs
Four studies included previous RRIs as a potential risk factor;14,16,20,22three of these studies included both male and female recreational runners.Two studies(low RoB)found no association,16,22while 1 study(low RoB)found that a previous RRI is a risk factor for RRIs.20We found moderate quality evidence(downgraded for inconsistency)that previous RRIs is not a risk factor.
One study(low RoB)found that a previous RRI is associated with new RRIs in male runners(low quality evidence)(single study,downgraded for inconsistency and imprecision).14
3.3.3.1.3.2.Musculoskeletal injury
Two studies(low RoB)found that a previous injury(musculoskeletal complaint)not attributed to running is a risk factor(high quality evidence)for new RRIs in short-distance runners.16,22
3.3.3.2.Long-distance runners
3.3.3.2.1.Personal factorsT
3.3.3.2.1.1.Age
Two studies included age as a potential risk factor;52,54one study(high RoB)in a generic population did not present data.52One study(medium RoB)found higher age to be a protective factor for RRIs in female runners.54We found very low quality evidence(single study,downgraded for study limitations,inconsistency,indirectness,and imprecision)that age is a protective factor in females.
3.3.3.2.1.2.BMI
Two studies assessed BMI as a potential risk factor but did not present data.52,54Three studies included weight as a potential risk factor;52,54,56one of these studies(high RoB)presented data and found no association.56We found very low quality evidence(single study,downgraded for study limitations,imprecision,and inconsistency)that weight is not a risk factor for RRIs in a generic population.Two studies included height as a potential risk factor,but did not present data.52,54
3.3.3.2.2.Training-related factors
Two studies included training volume as a potential risk factor.54,55One study(medium RoB)found no statistically significant association in female runners.54The other study(high RoB)presented no data.55We found very low quality evidence(single study,downgraded for study limitations,inconsistency,and imprecision)that training volume is not a risk factor for RRIs.
3.3.3.2.3.Health-related factors
The association between previous RRIs and new RRIs was assessed in 4 studies.50,52,54,55Three studies(1 medium RoB,2 high RoB)found associations between previous RRIs and new RRIs in a generic population.50,52,55One of these studies(high RoB)found an association for Achilles tendinopathy speci fically.52We found moderate quality evidence(downgraded for study limitations and indirectness,and upgraded for effect size)that a previous RRI is a risk factor for new RRIs.
One study(medium RoB)found a previous RRI to be a risk factor for stress fractures in female long-distance runners.54We found very low quality evidence(single study,downgraded for study limitations,indirectness,inconsistency,and imprecision)that a previous RRI is a risk factors for RRIs in female long-distance runners.
3.3.4.Risk models
We found a total of 11 risk models in 4 studies involving short-and long-distance runners(distances included 5-km,10-km,half marathon,and marathon).19,23,24,36One study found a risk model for RRIs in 5-km and 10-15-km runners.23One study found a risk model for RRIs in half marathon runners,24and 4 studies found a risk model for RRIs in marathon runners.19,23,24,36One study found a risk model for foot and shin injuries,but no knee injury risk model was found.36One study also found a risk model for knee and calf injuries.19All models varied in terms of the relevant predictors,and all but one had an area under the curve of approximately 70%or higher.Because all models were in the derivation stage,they were graded low quality.Three studies,which developed 8 risk models,were applicable in regard to population,prediction outcome and analysis.23,24,36One study,which developed 3 models,had concerns about the applicability due to the fact that only male marathon runners were included.19There is no evidence that these models are predictive for RRIs.The results for risk models involving short-and long-distance runners are summarized in Table 6 and Supplementary Table 8.
4.Discussion
To the best of our knowledge,no previous reviews have addressed differences in risk factors between short-and long-distance recreational runners and used the GRADE approach to judge the overall quality of evidence.In this SR,several risk factors were found for both short-and long-distance runners.
We found that a previous RRI was the strongest risk factor(with moderate quality evidence)for an injury in long-distance runners.In a generic population,previous injuries that were not attributed to running was the strongest risk factor(with high quality evidence)in short-distance runners.Higher BMI,higher age,sex(male),having no previous running experience,and lower running volume(<2 h/week)were strong risk factors(with moderate quality evidence)for short-distance runners.Low quality evidence was found for risk models as predictors for RRIs in short-and long-distance runners.
Since 2000, five SRs assessing risk factors for running injuries of the lower extremities have been published.5,10,12,16,57None of these reviews included studies having prospective designs with multivariable analysis and none aimed at identifying differences between short-and long-distance runners.
Differences in associations between injuries and risk factors may be explained by differences in selection criteria,study designs,and the RoB tools and data synthesis methods used.Inclusion criteria differed among the SRs,which lead to differences in the studies included in the reviews.For instance,1 review only included studies with overall lower extremity injuries and not with speci fic injuries.57The other 4 SRs included studies with several different designs,including randomized controlled trials,retrospective cohort studies and cross-sectional studies.Different methods were used for quality assessment for the articles included in the reviews.Our SR used the QUIPS tool as an assessment tool to assess RoB,but the other reviews used different tools to assess the RoB in their included studies.As a consequence,differences in the methodological quality of included studies can be found in the different SRs.For example,the study by Hirschmller et al.52was classi fied as high quality in the SR by van der Worp et al.,10but in our review the same study was classi fied as having low quality(high RoB).This difference might result in different conclusions.In contrast to our study,none of the SRs used the GRADE approach to assess the quality of the evidence.
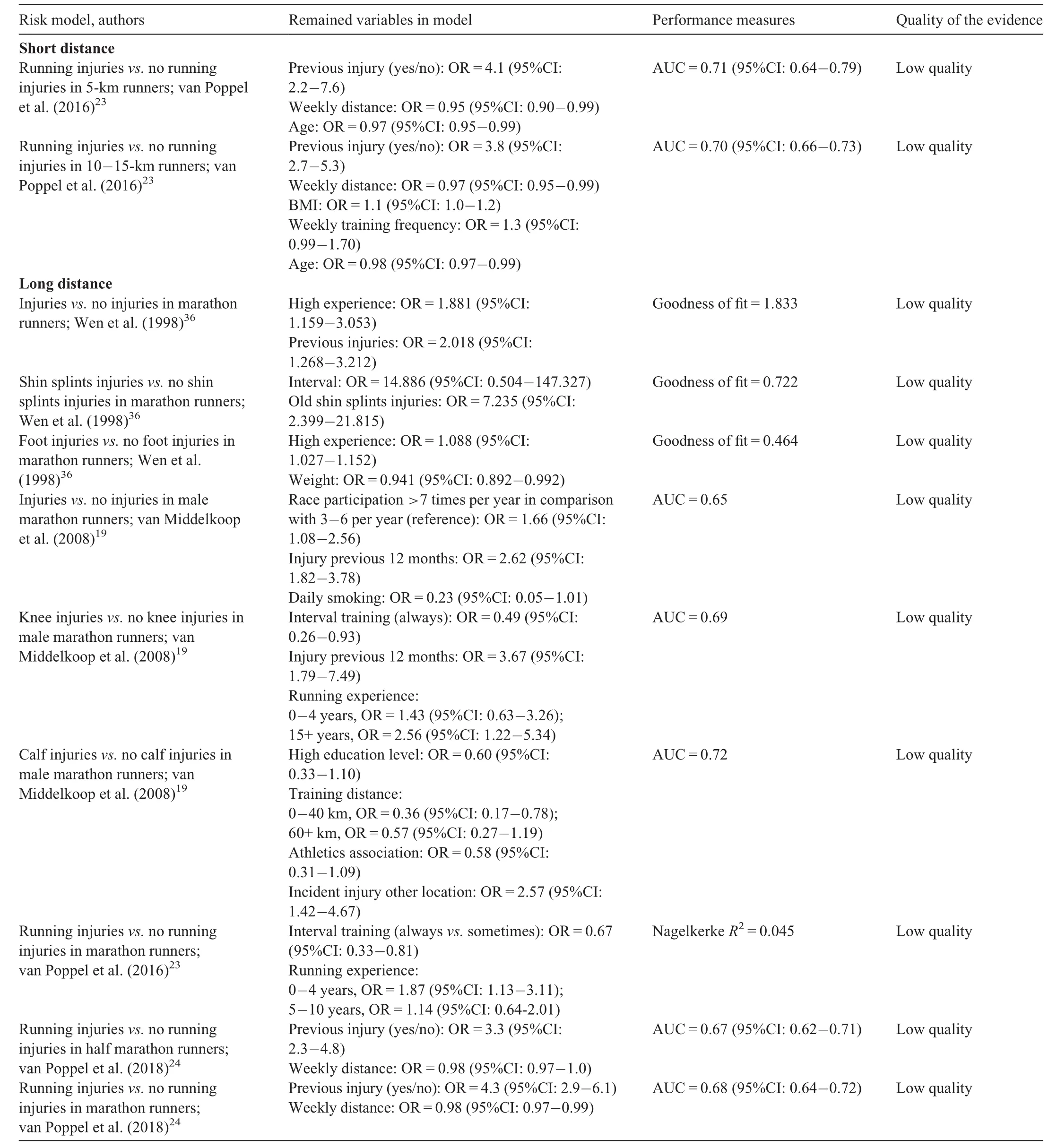
Table 6 Risk models.
Previous reviews found a previous injury to be a risk factor.5,10,12,16,57In our study,a previous RRI was also found to be the strongest risk factor for injuries among long-distance runners,but the de finition of a “previous injury”differed in the included studies and ranged from missing sports practice with an unclear timeframe54to injuries due to running in the 12 months preceding an event.23It remains unclear whether a higher injury risk is related to an incomplete healing of a previous injury,changed biomechanics due to a previous injury or other reasons.Although there is no uniform de finition of previous RRIs and current RRIs,many articles con firmed the association and it may be assumed that a previous injury increases the risk of a new injury.It is unclear why this association was not found in short-distance runners.In our review,2 studies(out of four)on short-distance runners found a previous RRI to be a risk factor for a new RRI.A possible explanation for the lack of association between previous RRIs and current RRIs among short-distance runners is that most studies on short-distance runners included novice runners.Because some novice runners just started running and thus have no history of injuries,they therefore cannot have had previous RRIs.For these runners,having a previous injury not attributed to running was the strongest risk factor.A possible mechanical explanation is that individuals without previous running experience who already have musculoskeletal complaints are more likely to get injured when they do run because their biomechanical loading capacity is lower.16
We found moderate quality evidence showing that no previous running experience is a risk factor for running injuries among short-distance runners.Also,limited evidence showing that no running experience was risk factor for running injuries was found in 3 other SRs.5,10,12The risk level for injury depends on the distances that are run by those who lack running experience.A possible explanation for why short-distance runners without running experience have a higher risk of injury is that novice runners build up their training too quickly,resulting in a lack of time for their tissue to adapt to training loads.In line with these studies,we found moderate quality evidence for lower running volume as a risk factor RRIs among short-distance runners.15,40However,this conclusion must be interpreted carefully,since running more than 60 min/week is protective and does not necessarily mean that running less than 60 min/week is a risk factor.An association between being older and RRIs might be suggested since experienced runners are often older.Although we found inconsistent evidence for age as a risk factor in our review,older age runners may have a higher risk of osteoarthritis,which could explain why more experienced runners are at higher risk of injury than less experienced runners.58
We found low quality evidence for higher BMI being a risk factor for RRIs.14,16,38Another SR investigated this association but did not find BMI to have a significant effect on running injuries.12This difference in our findings and the findings in the SR could be explained by the difference in the types of injuries sustained.Many studies examined BMI as a risk factor for overall injuries but not for speci fic types of injuries.For instance,lower BMI is associated with lower bone mineral density,which could therefore increase the risk of stress fractures.Increased BMI was significantly associated with the development of medial tibial stress syndrome.This is possibly due to the heavier impact loads that are likely associated with increased BMI.59-62
Only prospective cohort studies were included in our review because this study design is considered to be best for determining risk factors.29,63A second strength is that our review mainly used results from multivariable analyses,and only used risk factors that were adjusted for confounders.27Moreover,this is the first SR of RRIs that used the GRADE approach for data synthesis.
In only a few studies22,46,52-54was it unclear which confounders were used.Moreover,in the studies that adjusted the analyses for confounders,the type of confounders often differed.In addition,different methods of reporting risk factors were used,including odds,hazards,or relative risk ratios,which sometimes makes it dif ficult to compare risk or protective factors.For instance,higher BMI was often not presented with clear cut-off points.Furthermore,SRs should de fine injury-speci fic risk factors since these factors have different in fluences on different injuries.12,64However,very few studies summarize injury-speci fic risk factors,and the large diversity of injury de finitions,populations,and research methods in studies makes it dif ficult to make comparisons across studies.
Although 5 electronic databases were searched and selection bias was minimized using an adequate selection procedure and an inclusion form,it is possible that additional articles eligible for inclusion were missed.Also,unpublished studies could have been missed.31Differences in risk factors for shortand long-distance runners may be explained by the fact that some factors were examined in short-distance studies but not in long-distance studies,andvice versa.
In our study,running distance was dichotomized into short distance and long distance.However,the population of runners is quite heterogeneous in many studies,especially regarding their training patterns.The studies included in our review included participants who were either short-distance runners or long-distance runners(and the proportion was probably be balanced).Some risk factors might not apply to 1 category or the other,as stated in our study.Also,the criteria used to classify runners into short-and long-distance runners is arguable.In two of the 29 studies,running distance was around the cutoff point,so the distance was hard to classify for these 2 studies.40,47Finally,about two-thirds of the studies included in our review focused on short-distance runners,many of whom novice runners.Thus,the risk factors identi fied in our review for could be more speci fic to short-distance novice runners rather to short-distance runners in general.This may explain the observed differences in risk factors for short-and long-distance runners.Given these limitations,our results have to be interpreted with caution.
None of the studies included in our review directly compared the risk factors for RRIs between the 2 groups of interest,and this kind of study design should be encouraged in future research.More high-quality prognostic studies that compare the 2 groups are needed in order to improve insight into differences in risk factors between short-and long-distance runners.Study findings should be presented separately for these groups,not only in regard to distance but also in regard to the location and type of injury.Also,a uniform de finition of previous RRIs should be used,for example,the de finition recommended in a Delphi approach.65
5.Conclusion
Evidence regarding risk factors for RRIs is limited.Running injuries seem to have multifactorial origins.There is a need for additional high-quality studies on risk factors for RRIs before strong conclusions can be drawn about the relevance of speci fic risk factors.Furthermore,consensus must be reached on the de finition of running injuries,and large cohort studies are needed to investigate different types of risk factors(personal,training related,and health related),with an emphasis on the differences between short-and long-distance runners.In our review,we identi fied the following important risk factors for RRIs among short-distance runners:previous injuries not attributed to running,higher BMI,higher age,sex(male),having no previous running experience,and lower running volume.For long-distance runners,having previous RRIs was the most important risk factor.T
Authors’contributions
SvdH carried out the literature search;MvdW and AS carried out the inclusion of studies and quality assessment of the studies;DvP performed the data-analysis;DvP,MvM,APV,BWK,GSP participated in its design and coordination and helped to draft the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.T
Supplementary materials
Supplementary material associated with this article can be found in the online version at https://doi.org/10.1016/j.jshs.2020.06.006.
 Journal of Sport and Health Science2021年1期
Journal of Sport and Health Science2021年1期
- Journal of Sport and Health Science的其它文章
- Author biographies of Editor-in-Chief’s choice
- Association between physical activity and digestive-system cancer:An updated systematic review and meta-analysisT
- Physical exercise may exert its therapeutic in fluence on Alzheimer’s disease through the reversal of mitochondrial dysfunction via SIRT1-FOXO1/3-PINK1-Parkin-mediated mitophagyT
- Exercise interventions for older adults:A systematic review of meta-analysesT
- he mirror’s curse:Weight perceptions mediate the link between physical activity and life satisfaction among 727,865 teens in 44 countriesT
- Sensor-based physical activity,sedentary time,and reported cell phone screen time:A hierarchy of correlates in youthT