
Epidemiology and risk factors for sports- and recreation-related eye injury: a multicenter prospective observational study
2021-01-17 13:08DongEunLeeHyunWookRyooSungbaeMoonJaeYunAhnJungHoKimJongYeonKim
Dong Eun Lee, Hyun Wook Ryoo, Sungbae Moon, Jae Yun Ahn, Jung Ho Kim, Jong-Yeon Kim
1Department of Emergency Medicine, Kyungpook National University Chilgok Hospital, School of Medicine, Kyungpook National University, Daegu 41944, Republic of Korea
2Department of Emergency Medicine, Kyungpook National University Hospital, School of Medicine, Kyungpook National University, Daegu 41944, Republic of Korea
3Department of Emergency Medicine, Yeungnam University College of Medicine, Daegu 42415, Republic of Korea
4Department of Public Health, Kyungpook National University Hospital, Daegu 41944, Republic of Korea
Abstract
INTRODUCTION
With increase in free time and improve socioeconomic status, the number of individuals participating in sports and recreational activities has increased[1-2]. Depending on sports and recreational activities, various body parts may be injured, especially in the case of severe eye injury; permanent impairment, such as loss of vision, may occur; and quality of life may be reduced. Even mild eye injury can cause inconvenience in daily life, burden of treatment costs, and loss of labor.
There are over 600 000 cases of sports- and recreation-related eye injuries annually worldwide[3-4], and there are diあerences in the major sports activities that cause eye injuries depending on the region. Previous studies reported that eye injuries most commonly occurred during floorball and soccer games in Europe but during basketball and baseball games in the USA[5-10]. While there is some variation from sport to sport, >90% of sports- and recreation-related eye injuries can be prevented by using appropriate eye protection[3,11]. Therefore, for the prevention of eye injury, it is important to identify the epidemiological characteristics and risk factors of sports- and recreation-related eye injury in each region and devise an active preventive plan accordingly. In Korea, the acquisition and analysis of eye injury data registry has not been implemented. To assess this issue, we established a regional eye injury registry system that collects data of patients with eye injury who visited the ophthalmology Outpatient Department (OPD) and Emergency Department (ED) of four teaching hospitals in Daegu Metropolitan City of approximately 2.48 million individuals. This study aimed to identify the epidemiological characteristics of sports- and recreation-related eye injury in the community and analyze the risk factors associated with visual impairment at the first hospital visit using the regional eye injury registry
SUBJECTS AND METHODS
Ethical ApprovalThe study was approved by the Institutional Review Board (IRB) of Kyungpook National University Hospital (No.2019-02-010) and followed the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients.
We performed a multicenter prospective observational study of patients using the regional eye injury registry data. This study evaluated patients who have sports- and recreation-related eye injury from data collected from August 2016 to July 2018. Among patients visiting the ED or ophthalmology OPD of participating institutions who had eye injury, patients injured by sports- and recreation-related causative activity were included.
Daegu Metropolitan City has a population of approximately 2.48 million and an area of 883.54 km2. The Daegu eye injury registry is a multicenter network of four participating institutions for data collection and cooperative research in Daegu Metropolitan City. All participating institutions are tertiary teaching hospitals that have ED and Ophthalmology Departments and can provide medical care for eye injury patients 24h a day and 7d a week. Considering previous studies[2,12-13], the eye injury registry form was revised through expert meeting, which consisted of board-certified emergency medicine, ophthalmology and preventive medicine physicians and statisticians and was conducted to improve and modify data collection items. The initial report form focused on investigating epidemiologic data and risk factors regarding eye injuries. Additionally, the follow-up report form at 6mo was also created to evaluate and record ophthalmologic followup results after eye injury. Data are collected according to standardized templates for eye injury to facilitate uniform reporting using precisely defined variables and outcomes[14]. Data are cleaned and error checked before consolidation with the master dataset. The quality management performed and provided regular feedback on the accuracy of data input to research coordinators and investigators of each facility.
The outcome variables were presence of visual impairment at the first hospital visit. It was defined as visual impairment if the patient complained of decreasing visual acuity at the first hospital visit compared with the time before injury. We used the following Daegu eye injury registry variables: 1) patient demographics (i.e., sex and age); 2) injury details and risk factor of eye injuries (i.e., occurrence time of injury, place of injury, causative activity, causative material, information about protective eyewear use); 3) clinical characteristics of injuries (i.e., injury type, diagnosis, route of hospital visit, result of the first hospital visit, visual acuity (VA) and presence of visual impairment at the first hospital visit and 6-month follow-up). Eye injuries were classified with the widely used Birmingham Eye Trauma Terminology System[12]. Protective eyewear use was defined as the use of any eyewear with the objective of preventing injury regardless of the type of protective equipment, excluding glasses with corrective lenses and sunglasses. Initial and follow-up VA was measured as best-corrected VA with reference to the logarithm of the minimum angle of resolution (logMAR) and classified into five categories: no light perception (NLP), light perception (LP) to hand motion (HM), finger count (FC) to 0.1, 0.1 to 0.4 and ≥0.5. Follow-up VA was defined as the vision at the most recent follow-up visit within 6mo. Visual impairment was defined as the presence of patient complaints in decreased vision of the injured eye. The clinical diagnosis was categorized using the International Classification of Disease 10thedition and included only diagnostic codes for trauma[14].Statistical AnalysisCategorical variables are reported as counts and percentages. Patients were divided into two groups according to visual impairment at the first hospital visit. Pearson’s Chi-squared tests were conducted to assess the significance of the differences between the two groups. Distributions of sex, age, place, and causative materials were analyzed according to causative activities. To examine the association between causative activities and visual impairment at the first hospital visit, Logistic regression analysis was used. We included potential confounding variables such as age, sex, time of injury, route of hospital visit, and alcohol-related injury. The results are expressed as odds ratios (ORs) and 95% confidence intervals (CIs). All statistical tests were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA), andP-values <0.05 were considered statistically significant.
RESULTS
Among 4287 patients registered in the Daegu eye injury database between August 1, 2016, and July 31, 2018, 349 patients with sports- and recreation-related eye injury were analyzed (Figure 1). Of these patients, 84.2% were men. The proportion of teenagers and individuals in their 20s were 26.9% and 23.2%, respectively. Moreover, 45.6% (n=159) of patients had visual impairment at the first hospital visit. No diあerence was observed in sex and age distributions according to visual impairment at the first hospital visit. Injuries thatoccurred in school and injuries caused by sporting goods had higher rates of initial visual impairment. The rates of initial visual impairment were 44.9% and 49.1%, respectively, in the ED and ophthalmic OPD visits. Although protective eyewear was used, four eye injuries occurred, with one patient having visual impairment at the first visit (Table 1).

Table 1 General characteristics of the study population according to visual impairment at the first hospital visit n (%)

Figure 1 Study population.
Soccer was the most common causative activity of sports- and recreation-related eye injury, followed by baseball, badminton, hiking, combat sports, basketball, tennis and golf. The proportion of patients who complained of visual impairment at the first hospital visit was 66.7% and 57.9% in badminton and soccer, respectively, which was higher than those in other causative activities (Table 2).
The proportion of women injured during sports and recreation activities was higher in golf and badminton than in other activities, at 40.0% and 31.4%, respectively. Eye injuries while playing soccer in teenagers and individuals in their 20s hadrates of 50.0% and 31.6%, respectively. Baseball-related eye injuries had a similar proportion in teenagers and individuals in their 20 and 30s. Badminton-related eye injuries were noted in 25.5% of teenagers and individuals aged >50y, followed by 23.5% of those in their 40s. The most common age group according to sports and recreation activities were those aged >50y (74.3%) during hiking, individuals in their 20s (62.5%) during basketball, and individuals in their 40s (42.9%) during tennis (Table 3).
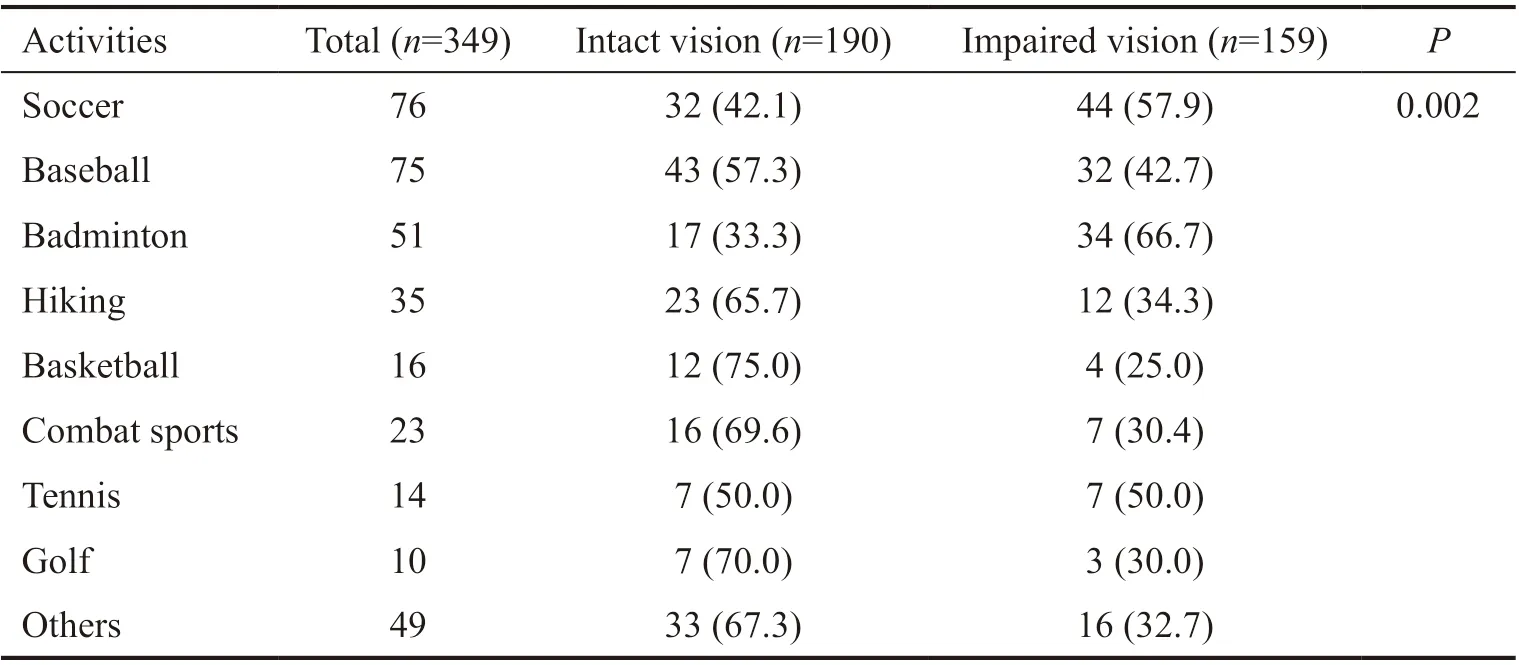
Table 2 Visual results of the first hospital visit according to causative activities n (%)
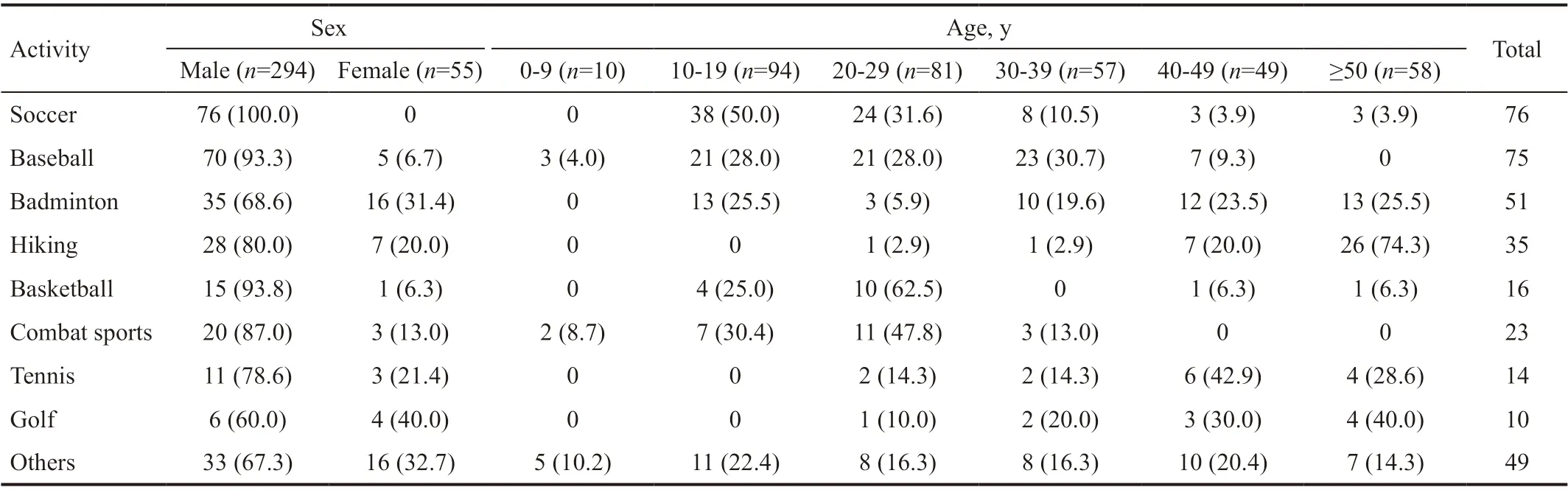
Table 3 Distribution of sex and age according to causative activities n (%)

Table 4 Distribution of place and causative material according to causative activities n (%)
The proportion of eye injuries caused by sports goods was higher than other materials in sports activities, such as in soccer, baseball, and badminton. In contrast, basketball- and combat sports-related eye injuries had high rates of injuries caused by human contact, and hiking-related eye injuries were caused by branches. Sports and leisure facilities were the major places of sports-related eye injuries. Moreover, eye injuries related to soccer, baseball and badminton activities occurred in school, 19.7% (n=15), 8% (n=6) and 11.8% (n=6), respectively (Table 4).
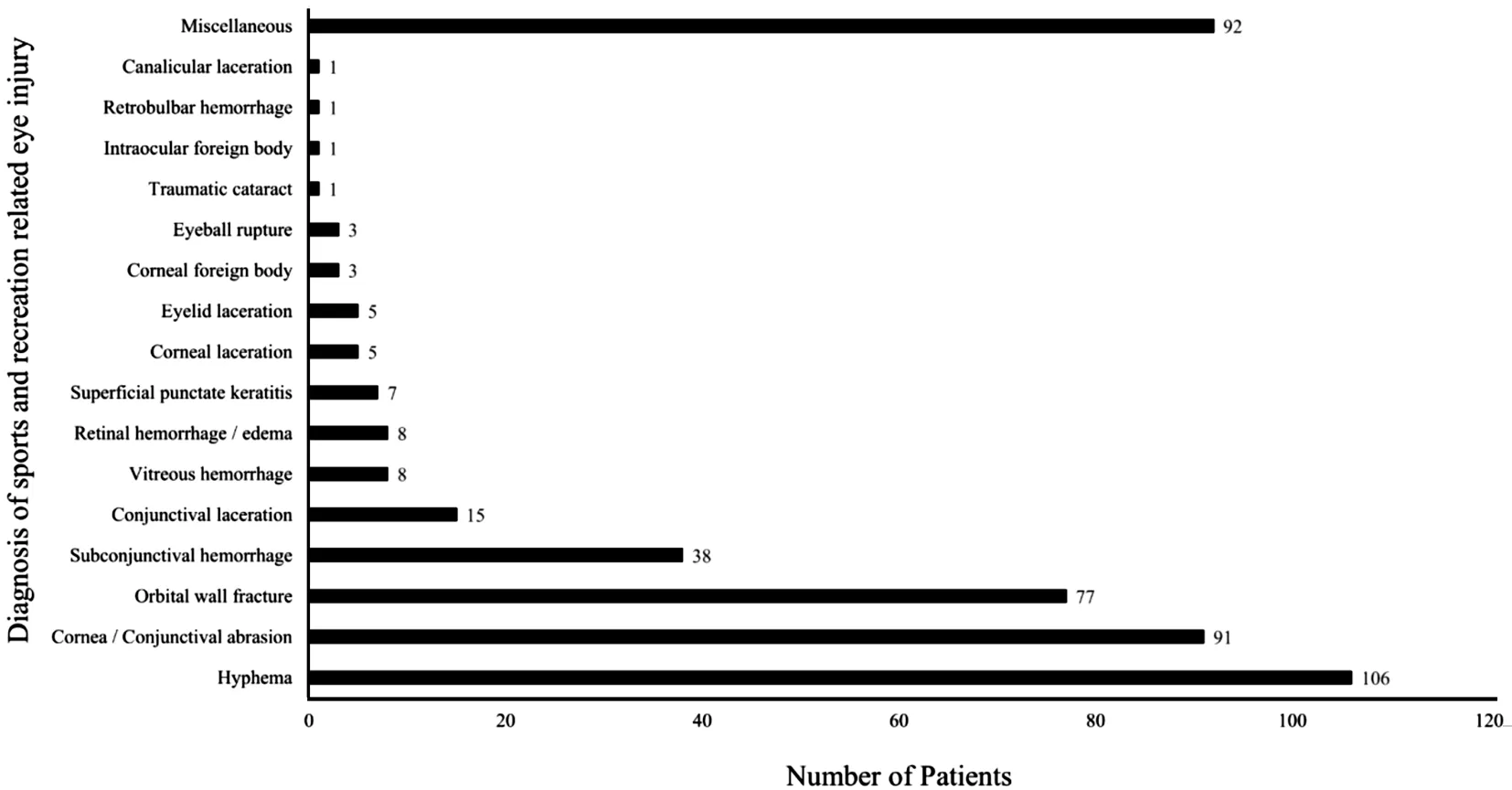
Figure 2 Distribution of diagnosis of sports-related eye injury.
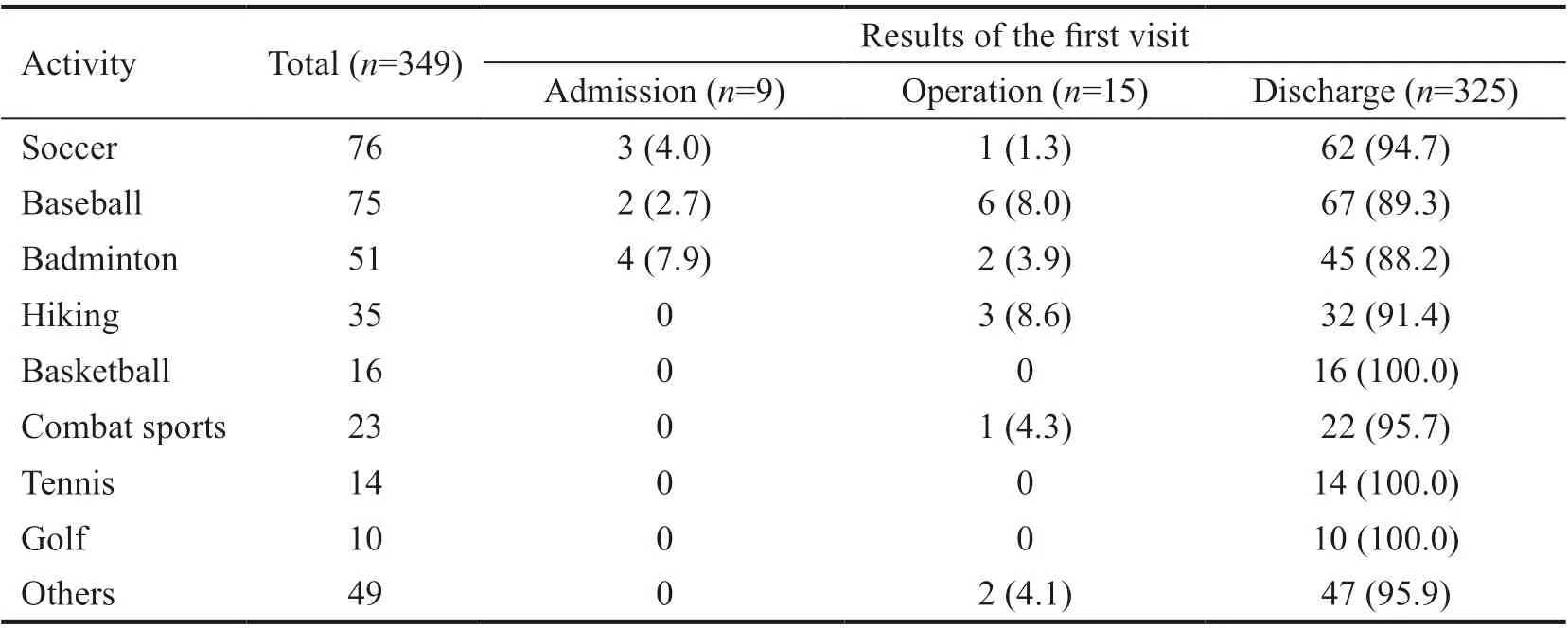
Table 5 Results of the first hospital visit according to causative activities n (%)
As a result of the initial hospital treatment, surgery was performed in 8.0% and 8.6% of eye injuries related to baseball and hiking, respectively. Among other events, two cases of surgery were performed in fishing-related eye injuries (Table 5). The distribution of diagnoses of eye injuries was decreased in the following order: hyphema, conjunctival abrasion, orbital wall fracture and subconjunctival hemorrhage (Figure 2). Hyphema was most common in football- and badmintonrelated eye injuries, and orbital fractures were common in basketball- and combat sports-related eye injuries. During hiking, corneal or conjunctival abrasion was the most common diagnosis of eye injury. One patient was diagnosed with intraocular foreign body (IOFB) during fishing. Two patients and one patient were diagnosed with eyeball rupture during baseball and fishing, respectively.
Among the 349 included patients with sports- and recreationrelated eye injuries, there were 354 eye injuries. VA at the first hospital visit was most commonly ≥0.5 (232 eyes, 65.5%), followed by 0.1 to 0.4 in 67 eyes (18.9%), LP to HM in 22 eyes (6.2%), FC to 0.1 in 14 eyes (4.0%), NLP in 3 eyes (0.8%) and absence of an initial VA examination in 16 eyes (4.5%). Of 159 patients (161 eyes) who initially complained of visual impairment, initial VA was ≥0.5 in 88 eyes (54.7%), followed by 0.1 to 0.4 in 43 eyes (26.7%), LP to HM in 18 eyes (11.2%), FC to 0.1 in 8 eyes (5.0%), NLP in 2 eyes (1.2%) and no presenting VA measurement in 2 eyes (1.2%). Among 159 patients who complained of decreased VA at the first hospital visit, 59 patients (37.1%) had improved followup VA, 17 patients (10.7%) showed no change in VA, 11 patients (6.9%) had decreased follow-up VA, and two patients did not have initial VA or follow-up VA. Moreover, 70 patients (44.0%) who complained of decreased VA at the first hospital visit had no outpatient follow-up. Badminton and soccer were associated with visual impairment at the first hospital visit compared with combat sports (OR, 4.57; 95%CI, 1.58-13.22 for badminton and OR, 3.14; 95%CI, 1.16-8.53 for soccer). After adjustment for potential confounders, badminton and soccer were still associated with visual impairment at the first hospital visit compared with combat sports (OR, 5.18; 95%CI, 1.67-16.09 for badminton and OR, 3.87; 95%CI, 1.36-10.99 for soccer; Table 6).
DISCUSSION
There are diあerent sports and recreation activities depending on the socioeconomic status and environment of the region. Thus, it is necessary to analyze epidemiological characteristics and risk factors for eye injuries by region to prepare a specific regional prevention program for sports- and recreation-relatedeye injuries. This study aimed to identify the epidemiological characteristics of eye injury associated with sports and recreation within a region and the activities associated with visual impairment at the first hospital visit. Men, teenagers, and individuals in their 20s had higher rates, and the frequency of eye injuries during sport activities was the highest in soccer, followed by baseball and badminton. Compared to combat sports, soccer and badminton were significantly associated with visual impairment at the first hospital visit. This study is significant in that it identified the epidemiological characteristics and risk factors of sports- and recreationrelated eye injuries in a region using a prospective multicenter eye injury registry, thus providing a basis for prevention. In the future, we intend to conduct regional-level eye injury prevention programs and monitor the results of these projects using the regional eye injury registry established in the present study. The advantage of this study is that the outpatients were included in the subject pool and the status of the subjects was confirmed in follow-up observations. Moreover, sports- and recreation-related eye injuries tend to be associated with socioeconomic status and culture. Most of the previous studies regarding sports- and recreation-related eye injuries were based on data from North America and European countries. The present study might therefore contribute to the prevention of sports- and recreation-related eye injuries in Asian countries that share similar cultural characteristics.
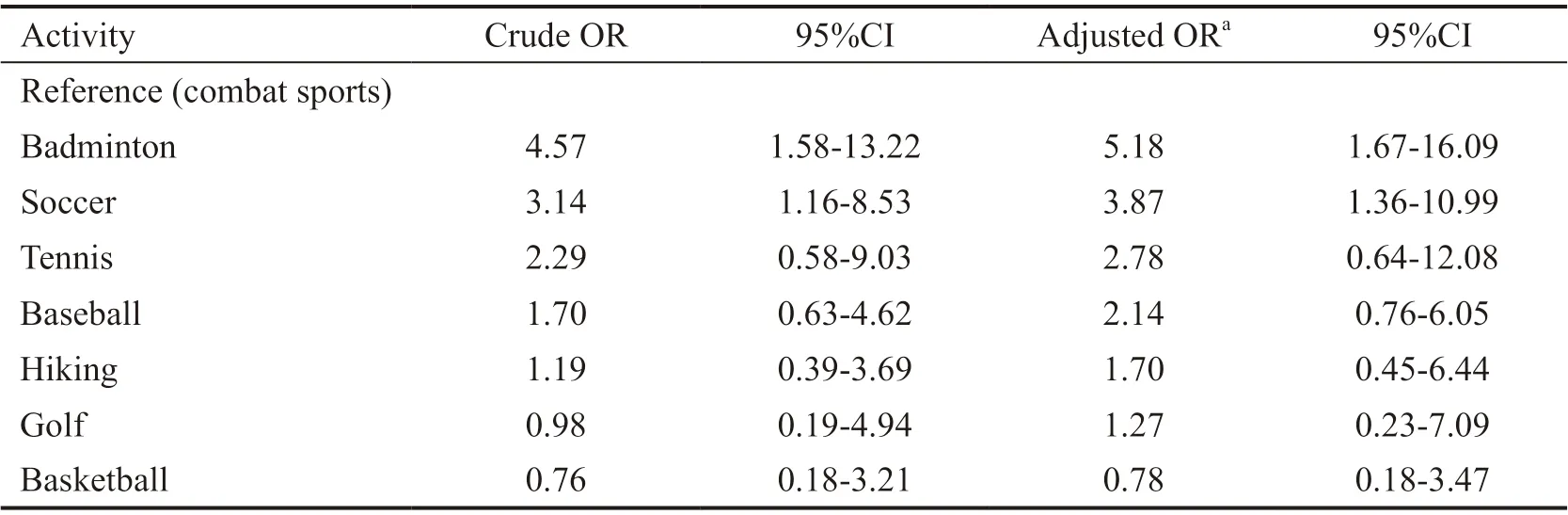
Table 6 Association between causative activities and visual impairment at the first hospital visit
The ratio of sports- and recreation-related eye injuries to overall eye injuries was 8.1%, similar to 7.6%-8.3% reported in previous studies in Korea[1-2]. Injury proportions were higher in men and also those in their 10s to early 20s in age distribution, similar to those in previous studies[1-2,7,15]. In this study, the most frequent diagnosis of eye injury was hyphema. Previous studies reported that sport related eye injuries accounted for 34.3% of the patients who was diagnosed with hyphema on ED visit, and hyphema was commonly caused by blunt trauma[16-17]. Among the patients diagnosed with hyphema, the proportion of patients with eye injuries associated with soccer and badminton activities was approximately 31.1% and 30.2%, respectively. Additionally, regarding the patients with eye injuries inflicted during soccer and badminton activities, there was a high rate of visual disturbance complaints at the initial hospital visits. According to Capão Filipeet al[6], eye injuries related to soccer were often due to contact with the ball and of more serious nature than those in other sports. These results are similar to the findings of this study. There are several cases of hyphema associated with blunt trauma caused by a ball or shuttlecock, which may explain why there were many complaints of visual impairment at the initial hospital visits. Of the 89 patients who complained of early visual disturbance, 11 had decreased vision in the 6-month follow-up. Among the 11 patients, six were injured due to soccer activities, while six were diagnosed with hyphema. It was confirmed that patients who complained of visual disturbance due to a blunt trauma in the early stages may not recover after a certain period of time, leading to long-term sequelae.
In Sweden, it became mandatory for children aged <15y to wear eye protection during floor sport activities, and the risk of eye injury was reduced to minimum[8,18]. In Canada, the proportion of eye injuries is higher during badminton activities than those in other racquet sports. To prevent eye injuries, the regulations for wearing eye protection that had been applied to doubles and youth players were expanded to doubles and experienced players[19]. In this study, the proportions of eye injuries caused by sporting goods in soccer and badminton were 77.6% (n=59) and 98% (n=50), respectively. Particularly, in the case of injuries caused by sporting goods, such as shuttlecocks, prevention efforts by wearing eye protection are expected to have a significant impact on eye injuries. Therefore, in the case of eye injuries associated with soccer and badminton that frequently occurred in teenagers and schools, it seems possible to prevent them by having eye protection equipment available in school sports activities and encouraging young athletes to wear it. Given that most eye injuries associated with sports activities occurred in sports facilities, it would be necessary to deploy eye protection equipment in club sports facilities.
In baseball-related eye injuries, the proportion of damage caused by sporting goods reached 97.3% (n=73), and there were 32 cases of orbital wall fracture. In the USA, among children’s eye injuries associated with baseball and softball, the proportion of eye injuries cause by a ball was 71.6%. Therefore, since injuries caused by baseball are difficult to prevent simply by wearing eye protection, it is recommended that athletes wear face protection helmets in youth baseball[9]. Moreover, to prevent eye injuries during baseball activities, it is necessary to apply regulations on wearing face protection helmets to youths and hobbyists and provide eye protection equipment or face protection helmets to sports facilities and schools in Korea.
In this study, the number of eye injuries due to fishing was relatively low but involved two cases of open globe injury (IOFB and eyeball rupture), both requiring surgery. Recreational fishing is one of the most popular outdoor activities in the USA, where fishing damage accounted for 16% of eye injuries in sports, and 44% of fishing-related eye injuries were reported to be open globe[20]. In our study, eye injuries related to fishing seem to require particular attention because they are mostly open globe injuries compared to those related to other sports and recreation activities, although their frequency is low. Eye injuries during hiking accounted for a high percentage of scratches that are caused by inducing materials, such as tree branches, during outdoor activities. Because eye injuries that occur during recreation activities, such as fishing and hiking, are likely to have a weak physical impact, wearing simple eye protection will be sufficient for prevention.
A previous study reported that eye injuries due to inappropriate wearing of eye protection in soccer may lead to a secondary damage[2]. In this study, a case of failing to prevent eye injury due to improper wearing of eye protection was reported in soccer, dodge ball, board, and ski activities. Particularly, in the case of eye injury during skiing, the inducing substance turned out to be goggles. Previous studies have emphasized the necessity of wearing eye protection in line with the American Society for Testing and Materials Standards[5,10-11,19-20]. Given that the present study also shows cases in which improper eye protection failed to prevent eye injuries, the importance of wearing suitable eye protection cannot be fully emphasized. Therefore, it is necessary to clearly establish the types and levels of protection for each sport or recreational activity, such as baseball, soccer, fishing, and hiking, and deploy proper protection equipment and train and promote its use according to the standards.
This study has some limitations. First, similar to other multicenter observational studies, this study has a potential limitation in the integrity and validity of data. Data were collected using standardized templates and guidelines, and eあorts were made to reduce the possibility of potential biases through regular quality control. Second, there might have been a selection bias, given that 36% of the participants were transferred from other hospitals; that is, these patients had more serious symptoms. Third, a follow-up was conducted 6mo after the injury in this study. However, given that eye injuries have a long-term risk of visual impairment, a longer-term follow-up may be needed. Lastly, since the characteristics of eye injury associated with sports and recreation vary according to region and age group, it may be diきcult to generalize these results to other regions or countries.
In this study, sports- and recreation-related eye injuries predominantly occurred in participants in their 10 and 20s, and men. The rate of eye injury was the highest in soccer, followed by baseball and badminton, while these eye injuries occurred mainly in sports facilities and schools. Therefore, intervention efforts are needed to deploy protection equipment in sports facilities and schools and promote its use during soccer, baseball and badminton activities, especially for those in their 10 and 20s.
ACKNOWLEDGEMENTS
Foundation:Supported by the Korea Centers for Disease Control and Prevention (No.2016E3300500).
Conflicts of Interest: Lee DE,None;Ryoo HW,None;Moon S,None;Ahn JY,None;Kim JH,None;Kim JY,None.
 International Journal of Ophthalmology2021年1期
International Journal of Ophthalmology2021年1期
- International Journal of Ophthalmology的其它文章
- Response of L V Prasad Eye Institute to COVID-19 outbreak in India: experience at its tertiary eye care centre and adoption to its Eye Health Pyramid
- Preliminary studies of constructing a tissue-engineered lamellar corneal graft by culturing mesenchymal stem cells onto decellularized corneal matrix
- Therapeutic potential of Rho-associated kinase inhibitor Y27632 in corneal endothelial dysfunction: an in vitro and in vivo study
- Changes of matrix metalloproteinases in the stroma after corneal cross-linking in rabbits
- A multi-omics study on cutaneous and uveal melanoma
- Eあects of quercetin on diabetic retinopathy and its association with NLRP3 inflammasome and autophagy