Lesson Ninety- eight Electrocardiographic analysis for His bundle pacing at implantation(part one)
2020-12-18 12:40:40童鸿
心电与循环 2020年6期
Types of His capture
It is mandatory to record a 12-lead ECG at His bundle pacing(HBP)implantation because changes in QRS morphology during threshold tests may be subtle and missed if only limb leads are used.
In addition to capture of the HB, the His lead can capture ventricular and/or atrial tissue that can affect ECG findings. Type of capture depends on His lead position(Figure 1), the anatomical variant of the HB,capture thresholds, pacing output, and pacing configuration(e.g., anodal capture in case of extended bipolar pacing). Furthermore, in case of underlying BBB, HBP may correct the conduction disease either partially or totally, leading to additional variations in QRS morphology.It is important to correctly identify the following entities.
Selective His bundle pacing
With selective His bundle pacing(S-HBP), an isoelectric interval is visible in all 12 leads, that corresponds to the His-ventricular(HV)interval and separates the pacing spike from QRS onset (Figures 1 and 2). Analysis of the device electrogram also shows a delay between delivery of pacing and the local ventricular electrogram. The QRS morphology is most often identical to that in intrinsic rhythm. However,slight differences in the paced QRS morphology may be observed in case the His lead is positioned distally,such as at the right bundle branch and/or HB bifurcation. In these instances, activation through the conduction system will follow a different course compared with intrinsic conduction.The His lead may be positioned on either the atrial aspect or the ventricular aspect of the tricuspid valve. Leads implanted at sites where the HB is subendocardial and distant from the ventricular myocardium will display S-HBP as the only form of capture.
Nonselective His bundle pacing
With nonselective His bundle pacing(NS-HBP),the lead is usually positioned in the ventricle at a site where the HB is surrounded by or at proximity to myocardial tissue. However, supravalvular lead position with either higher output and/or ventricular myocardium adjacent to the atrioventricular septum near the HB can also result in NS-HBP. The ECG shows a pseudo-delta wave corresponding to local myocardial capture,resembling pre-excitation of a para-Hisian or fasciculo-ventricular accessory pathway(Figures 1 and 2B). The amplitude and duration of the pseudo-delta wave will depend on the surrounding myocardial fiber density and mass of the captured myocardium and the HV interval(Figures 2B, 2C). The pseudo-delta wave may also be slightly shorter than the HV interval in case the His lead is positioned distally. QRS may show an initial isoelectric segment in some leads(especially leadⅢ) if the initial vector of depolarization is perpendicular to those leads. In addition to the pseudo-delta wave, fusion with myocardial activation results in an increase in R-wave amplitude in leads I,II, and V6(Figures 1B, 2)due to summation of the vectors of myocardial capture and activation via the His-Purkinje system.A reduction in R-wave amplitude in these leads helps identify the transition between NS-HBP and S-HBP in cases where the pseudo-delta wave may not be apparent. NS-HBP has the advantage of providing backup myocardial capture in case of loss of His capture or exit block. It is also associated with higher R-wave sensing amplitudes compared with S-HBP. No significant differences in cardiac mechanical synchrony or clinical outcome have been found between S-HBP and NS-HBP, although there was a trend in lower mortality with S-HBP.
Correction of bbb
It has been reported that approximately 60% to 90% of patients with BBB have QRS narrowing with HBP.The finding that the level of conduction block may be located proximally within the HB with longitudinal dissociation of the conduction fibers was originally described in the 1970s both for left bundle branch block(LBBB)and for right bundle branch block(RBBB).BBB may be totally or partially corrected by HBP.Conduction blocks may exist at different levels in a given patient, and HBP may correct BBB at a proximal level,which may then unmask distal conduction disease,which results in a different QRS morphology.
Myocardial capture only
The QRS complex maysometimes be relatively narrow (and narrower than in intrinsic rhythm with BBB). It may be difficultin some instances to distinguish myocardial capture from NS-HBP.
Transitions in QRS morphology with decrementing output
A number of different transitions in QRS morphology before loss of capture may be observed with decrementing pacing output (and starting at maximum output)(Figures 1).
In patients with RBBB, it may be difficult to distinguish NS-HBP with and without correction of the conduction disorder (Figure 1F). This is because myocardial capture in these instances serves to narrow the QRS (Figure 3D and section on HOT-CRT),much as1LV fusion pacing with coronary sinus leads serves to narrow the QRS complex in patients with underlying LBBB(17).Therefore,measuring the duration from the stimulus to the end of the QRS is not useful in this instance to determine whether RBBB has been corrected. The presence of an S- and/ or s-wave in leads I and/or aVL and a qR- and/or Qr-wave in leads V1 and/or V2 is suggestive of NS-HBP with uncorrected RBBB.
Additional transitions to those previously mentioned may be due to inhomogeneous capture of conduction tissue at different outputs (probably due to longitudinal dissociation of the HB). Inhomogeneous capture may result in slight variations in QRS morphology, both in patients with a narrow intrinsic QRS and in those with underlying BBB.Inhomogeneous capture may also be due to slight variations in lead orientation with the cardiac or respiratory cycle and may result in alternating BBB morphology. Furthermore,transitions in morphology due to anodal capture or capture of the right atrium may be sometimes observed and should not be confounded with transitions due to loss of capture of conduction tissue.
Absence of transitions in QRS morphology before total loss of capture with decrementing output indicates either: 1) S-HBP; 2) ventricular myocardial capture only (i.e., para-Hisian pacing, which cannot be considered as being true HBP); and 3) similar thresholds of different tissues that are simultaneously captured. To better distinguish the different capture thresholds, pulse width may be narrowed because this serves to widen the difference in capture thresholds between the HB and the adjacent myocardium.
Impossible transitions with decrementing output are: 1) S-HBP / NS-HBP; 2) S-HBP / myocardial capture only; and 3)without correction of BBB / with correction of BBB.
Thresholds of different tissues may be almost identical,and different types of capture may be observed during consecutive beats at a given output,probably due to slight variations in lead orientation and tissue contact.This is usually observed during pacing with output close to the capture threshold(s).
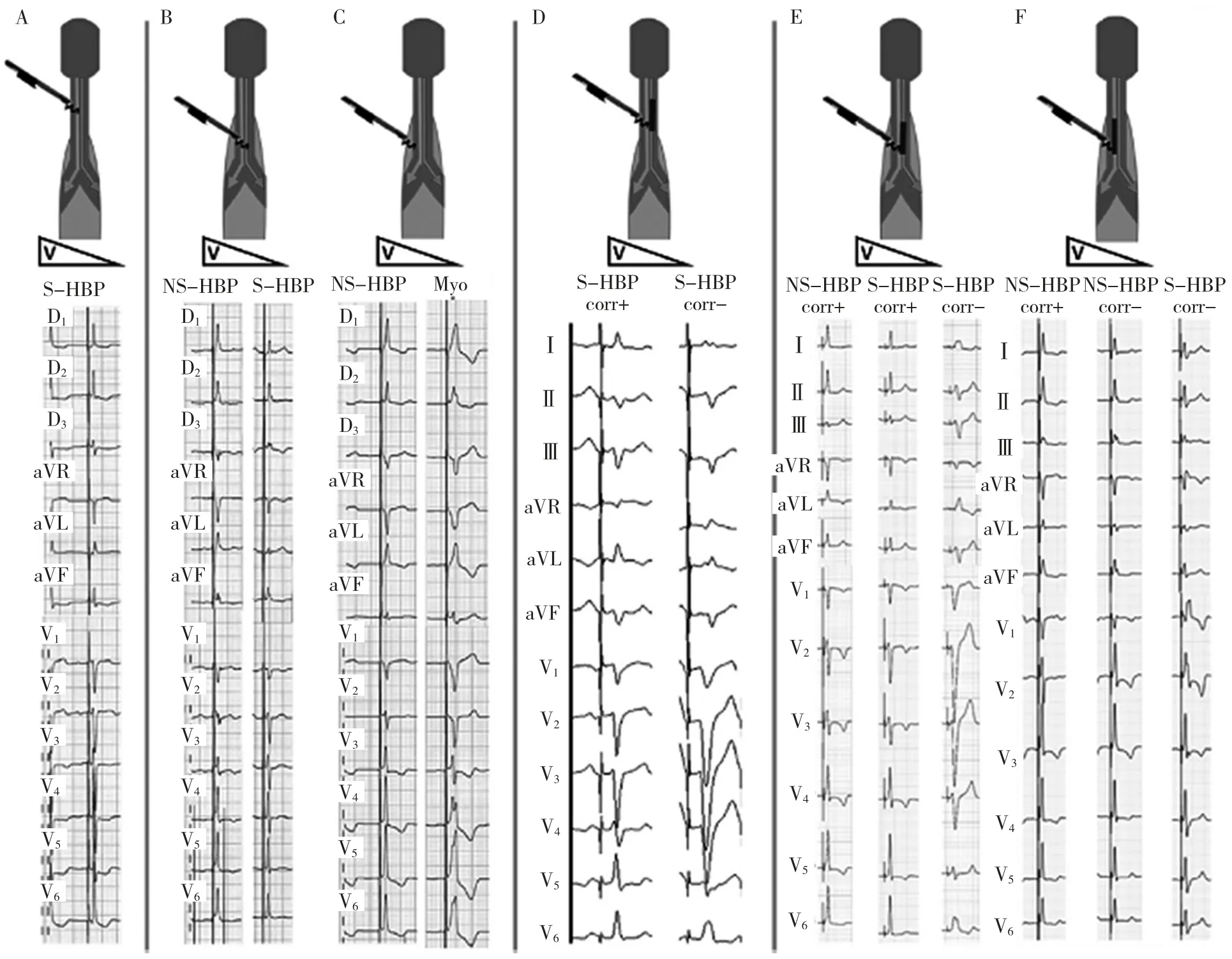
Figure 1 His Lead Position and Examples of Different Types of His Capture and Transitions in QRS Morphology With Decrementing Voltage Output. (A)Proximal position over a subendocardial His bundle with obligatory selective His capture(selective His bundle pacing [S-HBP]). Note the isoelectric interval between the pacing spike and QRS onset, visible in all 12 leads. (B)More distal position with a His bundle surrounded by a myocardial sleeve. There is close contact of the pacing lead and conduction tissue, resulting nonselective His bundle pacing (NS-HBP) with a pseudo-delta wave, which transitions to S-HBP with a reduction in output.(C)The lead is in less close contact with the conduction tissue, resulting in a transition between NS-HBP and myocardial(Myo) capture only.(D) Proximal position of the His lead with S-HBP in the setting of left bundle branch block (LBBB). At higher output, there is recruitment of conduction tissue resulting in correction (corr+) of the conduction delay and loss of correction (corr-) at reduced output. (E)More distal position of the lead with initial NS-HBP and correction of LBBB. (F)Right bundle branch block with initial correction and NS-HBP, with loss of correction(note the presence of an s wave in lead I and a more prominent R-wave in lead V2)followed by uncorrected S-HBP.
词 汇
configuration n.布局,配置,构造,构型,形状,轮廓
spike n.&v.尖状物,尖峰,大钉,动作电位;用大钉钉牢,用尖物刺入(或扎破),弃置不用,阻止
bifurcation n.分歧,分叉
resemble v.看起来像,像,类似于
summation n.总结,概括
unmask v.揭露,揭示
distinguish v.鉴别,区分,辨别
Inhomogeneous adj.不均质的,不均一的,多相的
underlying adj.在…下面的,基本的,潜在的,优先的
obligatory adj.强制的,必须的,有义务的,专性的,固性的,

Figure 2 Schematic Representation of Lead I and Ventricular Activation With Different Types of His Bundle Capture.(A)S-HBP with stimulus to QRS-onset interval corresponding to the His-ventricular(HV_ interval).(B) NS-HBP in the setting of a normal HV interval, with a small pseudo-delta wave and an increase in QRS amplitude. (C)NS-HBP in the setting of uncorrected LBBB and prolonged HV interval with widening of the paced QRS due to a large pseudo-delta wave and predominant activation of the left ventricle via cell-to-cell depolarization due delayed activation of the His-Purkinje system (D)NS-HBP in the setting of uncorrected right branch bundle block (RBBB)with narrowing of the QRS complex by virtue of pre-excitation of the right ventricle(activated late in intrinsic rhythm)and fusion with ventricular activation via the His-Purkinje system. In case of intrinsic bundle branch block which is corrected by His bundle pacing, the resulting paced QRS will resemble that of (A and B)in case of S-HBP or NS-HBP, respectively. HPS =His Purkinje system; other abbreviations as in Figure 1.
anodal adj.阳极的,正极的
decrement n.&v.递减,减少,消耗,减缩量,消耗量;减少,减缩
注 释
1.much as 本文中指“非常像,和…几乎一样”,例如:he works much as an experienced worker.他工作起来几乎与有经验的工人一样。也可解释为“尽管,虽然”,例如:Much as she hated cruelty,she couldn’t help watching the fight.虽然她对暴行极为憎恨,她还是不得不注视着这场斗殴。
参考译文
第98 课 希氏束起搏植入时的心电图分析(第一部分)
希氏束夺获的类型
希氏束起搏(His bundle pacing,HBP)植入时,如只记录肢体导联心电图,阈值测试过程的QRS 形态变化将会细微或缺失,因此,必须记录12 导联心电图。
希氏束电极不但夺获希氏束,也夺获心室和(或)心房组织,从而影响心电图图形。夺获类型决定于希氏束电极的位置(图1)、希氏束的解剖变异、夺获阈值、起搏输出和起搏配置(如在扩大双极起搏下的阳极夺获)。另外,在束支传导阻滞(bundle branch block,BBB)情况下,HBP 可以部分或完全纠正传导异常,这会增加QRS 形态的变化。正确识别下述本质实为重要。
选择性希氏束起搏
选择性希氏束起搏(selective His bundle pacing,S-HBP)时,所有12 导联均可见等电位间期,这与希氏-心室(HV)间期相一致,将起搏刺激波与QRS 波群起始部分开(图1 和2)。测试仪电图分析也显示在起搏刺激信号与局部心室电图之间有一延后。绝大多数情况下QRS 形态与自身节律相一致。不过,当希氏束电极位于远端如右束支和(或)希氏束分叉处时,可观察到起搏QRS 形态轻微不同。在此情况下,传导系统的激动过程会与自身传导的不同。希氏束电极可位于三尖瓣环的心房面或心室面。电极植入至内膜下希氏束而远离心室肌时,显示S-HBP 会是唯一的夺获。
非选择性希氏束起搏
非选择性希氏束起搏(nonselective His bundle pacing,NS-HBP)时,电极通常位于心室,该处的希氏束受心肌包绕或接近心肌组织。然而,当瓣上电极输出功率较高或心室肌毗连临近希氏束的房室间隔时,也能引起NS-HBP。心电图显示局部心肌夺获引起的假性delta 波,类似于希氏束旁或束支-心室旁道(图1 和图2B)。假性delta 波的振幅与间期决定于环绕心肌纤维的密度、所夺获心肌的量及HV 间期(图2B、2C)。如希氏束电极位于远端,假性delta 略短于HV间期。如起始除极向量垂直于导联时QRS 波群显示起始等电位节段(特别是Ⅲ)。除了假性delta 波,心肌激动的融入导致Ⅰ、Ⅱ和V6R 波振幅增大(图1B 和图2),这由心室夺获向量与通过希浦系统激动相加所致。当假性delta 波不明显时,这些导联的R 波振幅减小有助于确定NS-HBP 和S-HBP 之间的转换。NS-HBP 的优点是在希氏束夺获失败或传出阻滞时能提供后备的心室夺获。与S-HBP 比较,R 波的感知振幅也较高。尽管S-HBP 的病死率趋向较低,但S-HBP 和NS-HBP之间的心脏同步性或临床预后没有显著性差异。
束支传导阻滞纠正
据报道,合并BBB 的患者中近60%~90%HBP 时QRS波群变窄。1970 年代有关传导阻滞平面位于希氏束内近端并存在传导纤维纵向分离的最初描述是同时对于左束支传导阻滞(left bundle branch block,LBBB) 和右束支传导阻滞(right bundle branch block,RBBB)的。HBP 可完全或部分纠正BBB。对于特定的患者,传导阻滞可发生于不同层面,HBP 纠正近端的BBB 后,远端的传导病变得以显示,这可产生不同的QRS 形态。
仅为心肌夺获
QRS 波群有时较窄(较合并BBB 的自身节律窄)。这在有些情况下难以与NS-HBP 的心肌夺获相鉴别。
随着输出功率降低QRS 形态的移行
随着起搏输出功率的降低(从最大输出功率开始),在失去夺获之前可观察到多种QRS 形态移行变化(图1)。
对于RBBB 患者,可能难以辨别NS-HBP 是否纠正了传导病变(图1F)。这是因为这些情况下心肌夺获缩短了QRS波群(图2D),非常像LBBB 患者冠状窦电极的左心室融合性起搏,足以缩短QRS 间期。因此,在这种情况下测定从起搏信号到QRS 波群终末间期无助于确定RBBB 是否已得到纠正。Ⅰ和(或)aVL 出现 S 和(或)s 波以及 V1和(或)V2出现qR 和(或)Qr 提示 NS-HBP 未能纠正 RBBB。
除前面提到的以外,移行可由不同输出功率下传导组织的不均质夺获所引起(可能源于希氏束的纵向分离)。无论自身QRS 波群较窄或存在BBB 的患者,不均质夺获可引起QRS 形态轻微变化。不均质夺获也可源于电极指向心脏方向的轻微变化或呼吸周期变化,可引起交替性BBB 图形。此外,有时可观察到源于阳极夺获或右心房夺获的形态移行,不能与传导组织失去夺获的移行相混淆。
随着输出功率降低,在完全失去夺获之前缺乏QRS 形态移行提示存在以下几种情况之一:(1)S-HBP;(2)只有心室肌夺获(例如,希氏束旁起搏,这不能认为是真正的HBP);(3)不同组织阈值相似以致同步夺获。为了更好地区分不同的夺获阈值,可以缩短脉冲宽度,因为这可加大希氏束与邻近心肌之间的夺获阈值差异。
随着输出功率递减,不可能发生以下移行:(1)从S-HBP到 NS-HBP;(2)从 S-HBP 到只有心肌夺获;和(3)从 BBB 不能纠正到BBB 得到纠正。
不同组织的阈值几乎是一致的,在特定的输出功率下,连续搏动期间可观察到不同类型的夺获,可能与电极方向和组织接触的轻微变化有关。这通常见于起搏输出功率接近夺获阈值时。
图1希氏电极位置和随着电压输出降低不同类型希氏夺获和QRS 形态移行示例[A:置于心内膜下希氏束近端专一选择性希氏束夺获。注意起搏信号与QRS 波群起始之间的等电位间期,所有12 导联均能见到;B:较远端部位希氏束包绕于心肌袖中。起搏电极与传导组织接触紧密,导致NS-HBP而出现假性delta 波,随着输出功率降低而移行为S-HBP;C:起搏电极与传导组织接触不紧密,导致从NS-HBP 移行为单纯心肌夺获;D:LBBB 时希氏电极置于近端引起S-HBP。较高输出功率下,夺获传导组织而使传导延缓得以纠正(corr+),输出功率降低时失去纠正(corr-);E:电极置于较远端 时 初 始 为 NS-HBP 伴 LBBB 纠 正 ;F:RBBB 时 先 后 为NS-HBP 伴纠正,NS-HBP 不伴纠正(注意Ⅰ的s 波和V2的R 波)和 S-HBP 不伴纠正]
图2Ⅰ的模式图和不同类型希氏束夺获的心室激动[A:S-HBP 时刺激信号与QRS 波群起始之间的间期与HV 间期相一致;B:正常HV 间期下NS-HBP 伴随一小的假性delta波和QRS 波群增幅增大;C:未纠正LBBB 下的NS-HBP 和HV 间期延长伴随因假性大delta 波致起搏QRS 波群增宽以及由于希浦系统延迟激动而通过细胞-细胞除极的左心室为主激动;D:未纠正RBBB 下的NS-HBP 通过提前激动右心室(自身激动较迟)并与经希浦系统激动心室的融合而缩短QRS 波。当自身束支阻滞被希氏束起搏纠正后,S-HBP 和NS-HBP 引起的起搏QRS 波群将分别类似于A 和B]
猜你喜欢
中国临床医学影像杂志(2022年6期)2022-07-26 07:17:26
成都医学院学报(2021年2期)2021-07-19 08:35:20
自动化与信息工程(2021年1期)2021-03-12 11:20:48
心电与循环(2020年3期)2020-06-18 13:43:12
中国实验诊断学(2020年2期)2020-01-09 07:49:04
心电与循环(2019年6期)2019-12-10 01:37:40
国际心血管病杂志(2019年5期)2019-10-24 06:09:42
心电与循环(2019年2期)2019-04-10 12:09:24
心电与循环(2016年6期)2016-02-18 10:48:14
西南军医(2016年3期)2016-01-23 02:17:49