皮内针调理肝肺法治疗慢性难治性咳嗽的临床效果
2020-12-14 04:17刘志国李海霞王蕾边永君李光熙李国勤荣毅亢秀红
中国医药导报 2020年30期
关键词:皮内针
刘志国 李海霞 王蕾 边永君 李光熙 李国勤 荣毅 亢秀红


[摘要] 目的 研究皮內针调理肝肺法治疗慢性难治性咳嗽的临床效果。 方法 根据Excel生成随机数字表,采用随机、对照、单盲的方法将2015年6月—2016年3月中国中医科学院广安门医院门诊诊断为肝火犯肺型慢性难治性咳嗽24例患者分为治疗组和对照组,每组各12例。两组均予以基础治疗,在此基础上,治疗组给予皮内针治疗,对照组给予真穴安慰针治疗。治疗4周及治疗结束4周随访1次。以咳嗽症状积分、莱切斯特咳嗽量表(LCQ)和咳嗽视觉模拟评分(VAS)得分作为主要评估指标。 结果 研究过程中对照组脱落3例,失访2例,出差1例,剩余9例。咳嗽症状积分:日间咳嗽时间点比较差异、交互作用差异均有统计学意义(均P < 0.05),组间比较差异无统计学意义(P > 0.05)。夜间咳嗽评分时间点比较差异有统计学意义(均P < 0.05),组间比较及交互作用差异均无统计学意义(均P > 0.05)。组内比较:治疗4周后、疗程结束后4周,治疗组日间咳嗽积分和夜间咳嗽积分均较治疗前降低,对照组夜间咳嗽积分较治疗前降低(均P < 0.05)。VAS评分:咳嗽程度、咳嗽频率评分组间比较、时间点比较差异均有统计学意义(均P < 0.05),交互作用差异无统计学意义(P > 0.05)。夜间咳嗽评分时间点比较差异有统计学意义(均P < 0.05),组间比较及交互作用差异均无统计学意义(均P > 0.05)。组内比较:治疗4周后、疗程结束后4周,两组的咳嗽程度、咳嗽频率和夜间咳嗽评分均较治疗前降低(均P < 0.05)。组间比较:治疗4周后、疗程结束后4周,治疗组的咳嗽程度、咳嗽频率评分均低于对照组(均P < 0.05)。LCQ评分:生理部分、心理部分、社会部分评分时间点比较差异有统计学意义(均P < 0.05),组间比较及交互作用差异均无统计学意义(均P > 0.05)。总分的组间比较、时间点比较、交互作用差异均无统计学意义(均P > 0.05)。组内比较:治疗4周后、疗程结束后4周,治疗组生理部分、心理部分、社会部分评分均高于治疗前,差异均有统计学意义(均P < 0.05),疗程结束后4周,对照组心理部分、社会部分评分均高于治疗前,差异均有统计学意义(均P < 0.05)。 结论 皮内针治疗慢性难治性咳嗽安全有效。治疗效果主要体现在减轻咳嗽的严重程度及减少咳嗽的频率方面。
[关键词] 皮内针;难治性咳嗽;咳嗽视觉模拟量表;莱切斯特咳嗽量表;咳嗽症状积分
[中图分类号] R265.11 [文献标识码] A [文章编号] 1673-7210(2020)10(c)-0173-05
Clinical effect of treating chronic refractory cough with intradermal needle regulating liver and lung
LIU Zhiguo1,2 LI Haixia3 WANG Lei1 BIAN Yongjun1 LI Guangxi1 LI Guoqin1 RONG Yi1 KANG Xiuhong4
1.Department of Respiratory, Guang′anmen Hospital, China Academy of Chinese Medical Sciences, Beijing 100053, China; 2.Training Center, Guang′anmen Hospital, China Academy of Chinese Medical Sciences, Beijing 100053, China; 3.Department of Dermatology, Chongqing Traditional Chinese Medicine Hospital, Chongqing 402760, China; 4.Department of Gastroenterology, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing 100010, China
[Abstract] Objective To study the clinical effect of treating chronic refractory cough with intradermal needle regulating liver and lung. Methods According to Excel, a random number table was generated, and the 24 patients diagnosed as liver fire invading lung type chronic refractory cough in the outpatient clinic of Guang′anmen Hospital, China Academy of Chinese Medical Sciences from June 2015 to March 2016 were divided into treatment group and control group by random, controlled and single blind method, with 12 cases in each group. Both groups were given basic treatment, on this basis, the treatment group was given intradermal needle treatment, and the control group was given true acupoint comfort needle treatment. Treatment was performed for four weeks, and one follow-up was performed after four weeks of treatment. Cough symptom score, Leicester cough questionnaire (LCQ) and cough visual analogue scale (VAS) scores were used as the main evaluation indicators. Results During the study, three cases of abscission, two cases of loss of follow-up, one case of business trip and the remaining nine cases were in the control group. Cough symptom scores: there were statistically significant differences in the time points and the interaction of daytime cough between the two groups (all P < 0.05), but no statistically significant differences between the two groups (P > 0.05). The differences of night cough score at time points were statistically significant (all P < 0.05), while the differences between the two groups and interaction were not statistically significant (all P > 0.05). Intra-group comparison: after four weeks of treatment and four weeks after the end of the treatment course, the scores of daytime cough and night cough in the treatment group were all lower than those before treatment, and the scores of night cough in the control group were lower than those before treatment (all P < 0.05). VAS score: there were statistically significant differences in the scores of cough degree and cough frequency between groups and at time points (all P < 0.05), but no statistically significant difference in the interaction (P > 0.05). The differences of night cough score at time point were statistically significant (all P < 0.05), while the differences between the two groups and interaction were not statistically significant (all P > 0.05). Intra-group comparison: after four weeks of treatment and four weeks after the end of treatment course, cough degree, cough frequency and night cough score of the two groups were all lower than those before treatment (all P < 0.05). Comparison between groups: after four weeks of treatment and four weeks after the end of treatment course, the scores of cough degree and cough frequency in the treatment group were lower than those in the control group (all P < 0.05). LCQ scores: there were statistically significant differences in the time points of the physiological, psychological and social part scores (P < 0.05), while the differences between the two groups and interaction were not statistically significant (all P > 0.05). There were no statistically significant differences between the two groups, time points and interaction in the total score (all P > 0.05). Intra-group comparison: after four weeks of treatment and four weeks after the end of treatment course, the treatment group physical parts, psychological part, social part scores were higher than those before treatment, the differences were statistically significant (all P < 0.05), four weeks after the end of treatment course, the control group psychological part, social part scores were higher than those before treatment, the differences were statistically significant (all P < 0.05). Conclusion Intradermal needle is safe and effective in treating chronic refractory cough. The therapeutic effect is mainly reflected in reducing the severity and frequency of cough.
[Key words] Intradermal needle; Refractory cough; Cough visual analogue scale; Leicester cough questionnaire; Cough symptom score
咳嗽是呼吸科门诊最常见的临床症状之一。难治性咳嗽是指病因诊断不明和/或疗效欠佳的慢性咳嗽。现有咳嗽指南推荐的诊治流程要求在仔细询问病史和体检基础上,选择必要的辅助检查以查明慢性咳嗽的可能病因,结合针对病因的治疗反应来证实或排除诊断[1-2]。文献报道8%~10%的成年人口患有慢性咳嗽[3],尤其是女性(80%)[4]。患者反复使用抗生素或镇咳药物治疗,效果不佳,给患者生理、心理造成严重影响[5]。目前尚不清楚慢性咳嗽的发生机制,其发病机制可能包括咳嗽反射超敏反应、外周敏感化和中枢敏感化等[6-7],常见的危险因素是病毒感染、空气污染、环境暴露、寒冷的气候和吸烟。ACCP指南确定了四类治疗方法-非药物疗法、吸入糖皮质激素、神经调节疗法和其他疗法[8-9]。而常规治疗的副作用却不能令人满意。许多医生推荐使用非药物疗法,例如健康的生活方式教育[10]、言语干预[11]和呼吸训练[12]等。针灸疗法(AT)作为中药的非药物疗法已被广泛用于治疗多种疾病,例如哮喘[13],慢性阻塞性肺疾病(COPD)[14]、抑郁症[15]等。研究显示针灸治疗咳嗽效果显著[16],但操作不方便。皮内针疗法是以特制的小型针具固定于腧穴的皮内或皮下,进行较长时间埋藏的一种针灸方法,操作简便易行[17]。本研究旨在系统评估皮内针治疗慢性难治性咳嗽的效果。
1 资料与方法
1.1 诊断标准
1.1.1 西医诊断标准 根据中华医学会呼吸病学分会哮喘学组制定的2009年版《咳嗽的诊断与治疗指南》[18]慢性咳嗽的诊断标准:①X线胸片或胸部CT无明显异常;②以咳嗽为主要甚至惟一的症状;③咳嗽持续时间>8周;④无明显的咳嗽原因;⑤经过常规治疗但效果不佳且病因未查明者。
1.1.2 中医诊断分型标准 中医诊断标准参照《咳嗽中医诊疗专家共识意见(2011版)[19]中属于肝火犯肺证者。肝火犯肺型咳嗽症见:上气咳逆阵作,咳时面红目赤,咳引胸痛,可随情绪波动增减,烦热咽干,口干口苦,常感痰滞呕喉,咯之难出,量少质黏,胸胁胀痛,舌质红,苔薄黄少津,脉弦数。
1.2 纳入标准
①符合上述慢性难治性咳嗽的西医诊断标准;②符合上述肝火犯肺证的中医诊断标准;③中西医常规治疗时间>1个月,咳嗽症状积分下降<2分;④年龄18~75岁;⑤患者同意并签署知情同意书。
1.3 排除标准
①有其他慢性呼吸系统疾病者,如肺间质纤维化、慢性支气管炎、肺部肿瘤、肺气肿、肺心病、COPD、呼吸衰竭等;②已明确诊断慢性咳嗽的病因:包括上气道咳嗽综合征、嗜酸性粒细胞性支气管炎、变应性咳嗽、咳嗽变异性哮喘、胃食管返流综合征、药物反应、肺部感染、肺及气管内膜结核、成人百日咳等;③妊娠期和哺乳期妇女;④诊断合并有心、肝、肾及造血系统等严重原发病的患者。
1.4 一般资料
选择2015年6月—2016年3月中国中医科学院广安门医院(以下简称“我院”)门诊诊断为肝火犯肺型慢性难治性咳嗽的患者24例作为研究对象,样本筛选自此期间的2800例慢性咳嗽患者。按随机数字表法,采用随机、对照、单盲的方法将24例患者分为治疗组和对照组,每组各12例。治疗组男3例,女9例,平均年龄(47.53±12.50)岁,平均病程(13.33±9.14)年;對照组男0例,女12例,平均年龄(49.15±14.94)岁,平均病程(13.28±9.56)年。两组性别、年龄、病程比较,差异无统计学意义(P > 0.05),具有可比性。本研究经我院医学伦理委员会审核通过,患者知情同意并签署知情同意书。
1.5 治疗方法
基础治疗:使用白三烯受体拮抗剂、镇咳药等西药及中药治疗。
治疗组在基础治疗的基础上,增加皮内针治疗,针具为苏州华佗医疗器械有限公司生产的图钉型皮内针,规格为0.2 mm×1.5 mm,针灸穴位为印堂、双侧尺泽、双侧列缺、双侧合谷、双侧太冲。将皮内针贴于穴位表面,按压1 min。治疗共8次,每周2次,20 min/次。共治疗4周。对照组在基础治疗的基础上,增加真穴安慰针(图钉型皮内针去掉针尖、只余胶布和环形针柄制成)治疗,穴位同治疗组。不进行按压刺激。共治疗10次,前2周每周3次,后2周每周2次,共治疗4周。每次针具需在患者身上持续24 h,患者回家到时间后自行取下。
1.6 观察指标
疗程结束后4周通过医院就诊的方式进行随访。治疗前、治疗4周后、疗程结束后4周记录患者咳嗽症状积分、视觉模拟评分(VAS)、莱切斯特咳嗽量表(LCQ)评分。
1.6.1 咳嗽症状积分 咳嗽症状积分是一种分栏式评分法,于1994年由Hsu等[20]首先提出,该评分表根据咳嗽发生时间分为日间和夜间两部分,再按咳嗽频率、强度和对睡眠及日常活动影响程度划分为0~5分,6个等级,0分为无咳嗽,5分为最剧烈的咳嗽。我国2009年版咳嗽指南[18]中推荐使用的咳嗽积分表是从咳嗽症状积分表演变而来的,它将原来按咳嗽严重程度划分为0~5分的6个等级缩减为0~3分的4个等级。0分为无咳嗽;1分偶有短暂性咳嗽或入睡时短暂咳嗽或偶有夜间咳嗽;2分频繁咳嗽,影响日常生活或因咳嗽轻度影响夜间睡眠;3分频繁咳嗽,严重影响日常生活或因咳嗽严重影响夜间睡眠。
1.6.2 VAS VAS[21]由一条10 cm长的线组成,刻度从0~10 cm。0分为无痛;≤3分为有轻微的咳嗽,能忍受;4~6分为咳嗽严重并影响睡眠,尚能忍受;7~10分:咳嗽难忍,影响食欲,影响睡眠。
1.6.3 LCQ LCQ[22]由Birring于2003年創立,涉及生理、心理和社会3个方面。共有19个项目,每个项目分为7个级别。19项各项均按1~7分进行评分,生存质量越低得分越低。判读标准:LCQ的最小重要性差异(MID)为1.3分,即患者觉得有意义的最小健康变化,分值升高1.3分说明治疗有临床意义。
1.7 统计学方法
数据使用epidata3.0建库,使用SPSS 20.0统计学软件对所得数据进行分析。计量资料采用均数±标准差(x±s)表示,两组组间比较采用独立样本t检验;重复测量的计量资料采用重复测量方差分析。计数资料采用例数表示,组间比较采用χ2检验。以P < 0.05为差异有统计学意义。
2 结果
试验结束后,对照组脱落3例,失访2例,出差1例,完成有效病例21例。
2.1 两组治疗前后咳嗽症状积分比较
整体分析发现:日间咳嗽时间点比较差异、交互作用差异均有统计学意义(P < 0.05),组间比较差异无统计学意义(P > 0.05)。夜间咳嗽评分时间点比较差异有统计学意义(P < 0.05),组间比较及交互作用差异均无统计学意义(均P > 0.05)。组内比较:治疗4周后、疗程结束后4周,治疗组日间咳嗽积分和夜间咳嗽积分均较治疗前降低,对照组夜间咳嗽积分较治疗前降低(均P < 0.05)。见表1。
2.2 两组治疗前后咳嗽VAS评分比较
整体分析发现:咳嗽程度、咳嗽频率评分组间比较、时间点比较差异均有统计学意义(均P < 0.05),交互作用差异无统计学意义(P > 0.05)。夜间咳嗽评分时间点比较差异有统计学意义(P < 0.05),组间比较及交互作用差异均无统计学意义(均P > 0.05)。组内比较:治疗4周后、疗程结束后4周,两组的咳嗽程度、咳嗽频率和夜间咳嗽评分均较治疗前降低(均P < 0.05)。组间比较:治疗4周后、疗程结束后4周,治疗组的咳嗽程度、咳嗽频率评分均低于对照组(均P < 0.05)。见表2。
2.4 两组治疗前后LCQ问卷评分比较
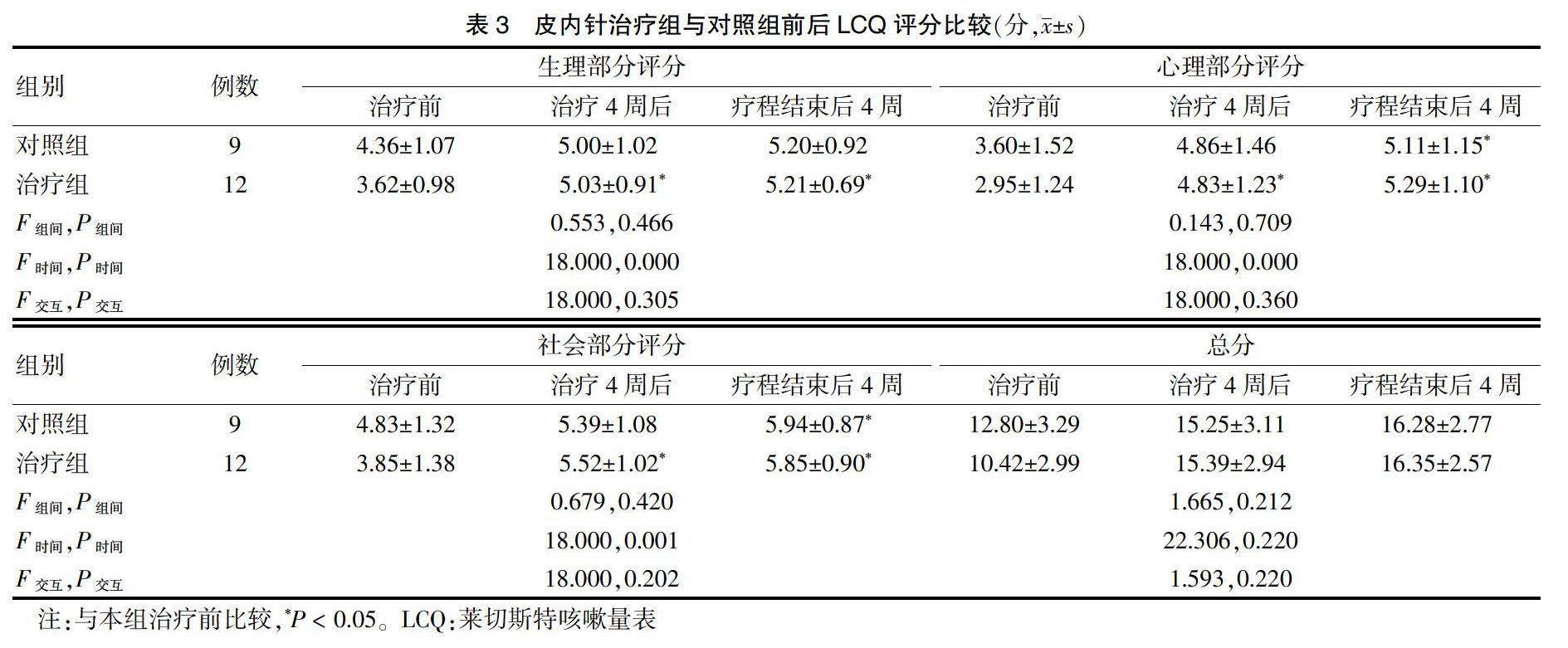
整体分析发现:生理部分、心理部分、社会部分评分时间点比较差异有统计学意义(均P < 0.05)。组间比较及交互作用差异均无统计学意义(均P > 0.05)。总分组间比较、时间点比较、交互作用差异均无统计学意义(均P > 0.05)。组内比较:治疗4周后、疗程结束后4周,治疗组生理部分、心理部分、社会部分评分均高于治疗前,差异均有统计学意义(均P < 0.05),疗程结束后4周,对照组心理部分、社会部分评分均高于治疗前,差异均有统计学意义(均P < 0.05)。见表3。
3 讨论
本研究结果显示,皮内针治疗能显著改善慢性难治咳嗽患者的症状,也可以一定程度上改善慢性难治咳嗽患者的生活质量,停药后针刺治疗仍起作用。在慢性难治咳嗽的治疗中,普通针刺疗法较常采用,皮内针的治疗使用较少。传统的针刺疗法虽然有效,但其治疗频率通常是每周2~3次,缺乏持续缓解咳嗽的作用,且刺激相对较大,容易出现晕针、出血等不良反应。而皮内针能对皮肤产生微弱而持久的刺激,调节经络和脏腑的功能,适用于慢性顽固性疾病或留针时间较长的疼痛性疾病。在本研究中,治疗组的针头为0.2 mm×1.5 mm的推针式皮内针,刺激较小,不影响其日常活动。与普通针刺疗法比较,皮内针操作简便,无特殊场地要求,刺激量小、对患者伤害小,即使是害怕针灸的患者也能接受并很容易实施。因此,对于慢性难治咳嗽患者,皮内针治疗是一种值得推广的中医技术。
此外,实验中还发现,罹患慢性难治咳嗽的女性患者比例远高于男性患者,这与咳嗽的流行病学研究一致[23]。本研究患者中中年女性多见,这个年龄段的女性处于更年期,情绪焦虑,精神紧张,容易引起精神障碍,导致习惯性咳嗽或心理性咳嗽的发生[24-26]。今后,如何对慢性难治咳嗽开展规范治疗、在基层或社区医院推广皮内针疗法、进一步研究女性患者更多罹患慢性难治咳嗽的病因病机,将是我们研究的重点方向。
[参考文献]
[1] 余莉,陈强,邱忠民.难治性咳嗽的诊治[J].中华结核和呼吸杂志,2016,39(5):383-386.
[2] Irwin RS,Madison JM. Anatomical diagnostic protocol in evaluating chronic cough with specific reference to gastroesophageal reflux disease [J]. Am J Med,2000,108(Suppl 4a):126S-130S.
[3] Chung KF,Pavord ID. Prevalence,pathogenesis,and causes of chronic cough [J]. Lancet,2008,371(9621):1364-1374.
[4] He L,Li B,Chen Y,et al. Diagnosis and treatment of chronic cough in the elderly [J]. Guide of China Medicine,2012, 10:47-49.
[5] Iyer VN,Lim KG. Chronic cough:an update [J]. Mayo Clin Proc,2013,88(10):1115-1126.
[6] Chung KF. Approach to chronic cough:the neuropathic basis for cough hypersensitivity syndrome [J]. J Thorac Dis,2014,6(Suppl 7):S699-707.
[7] Haque RA,Usmani OS,Barnes PJ. Chronic idiopathic cough: a discrete clinical entity [J]. Chest,2005,127(5): 1710-1713.
[8] Randel A. ACCP Releases Guideline for the Treatment of Unexplained Chronic Cough [J]. Am Fam Physician,2016,93(11):950.
[9] 顾永丽,温燕,孙增先,等.特异性神经调节剂用于治疗难治性慢性咳嗽的研究进展[J].中华结核和呼吸杂志,2020,43(5):460-463.
[10] Vertigan AE,Theodoros DG,Gibson PG,et al. Efficacy of speech pathology management for chronic cough:a randomised placebo controlled trial of treatment efficacy [J]. Thorax,2006,61(12):1065-1069.
[11] Chamberlain S,Garrod R,Birring SS. Cough suppression therapy: does it work? [J]. Pulm Pharmacol Ther,2013, 26(5): 524-527.
[12] Murry T,Branski RC,Yu K,et al. Laryngeal sensory deficits in patients with chronic cough and paradoxical vocal fold movement disorder [J]. Laryngoscope,2010,120(8):1576-1581.
[13] Jiang C,Jiang L,Qin Q. Conventional Treatments plus Acupuncture for Asthma in Adults and Adolescent:A Systematic Review and Meta-Analysis [J]. Evid Based Complement Alternat Med,2019,2019:9580670.
[14] Yu M,Gao L,Kong Y,et al. Safety and efficacy of acupuncture for the treatment of chronic obstructive pulmonary disease: A systematic review protocol [J]. Medicine (Baltimore),2019,98(37):e17112.
[15] Li W,Yin P,Lao L,et al. Effectiveness of Acupuncture Used for the Management of Postpartum Depression:A Systematic Review and Meta-Analysis [J]. Biomed Res Int,2019,2019:6597503.
[16] 陳金凤,张文竹,王靖轩,等.针刺自主神经相应区域治疗慢性咳嗽[J].长春中医药大学学报,2018,34(5):919-922.
[17] 蒙剑华,李志明,刘梅英.皮内针联合中药治疗面肌痉挛的临床疗效观察[J].当代医学,2020,26(29):5-7.
[18] 中华医学会呼吸病学分会哮喘学组.咳嗽的诊断与治疗指南[J].中华结核和呼吸杂志,2016,39(5):323-354.
[19] 中华中医药学会内科分会肺系病专业委员会.咳嗽中医诊疗专家共识意见(2011版)[J].中医杂志,2011,52(10):896-899.
[20] Hsu JY,Stone RA,Logan-Sinclair RB,et al. Coughing frequency in patients with persistent cough: assessment using a 24 hour ambulatory recorder [J]. Eur Respir J,1994,7(7):1246-1253.
[21] Fukumitsu K,Kanemitsu Y,Asano T,et al. Tiotropium Attenuates Refractory Cough and Capsaicin Cough Reflex Sensitivity in Patients with Asthma [J]. J Allergy Clin Immunol,2018,In practice 6:1613-1620.
[22] Birring SS,Prudon B,Carr AJ,et al. Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ) [J]. Thorax,2003,58(4):339-343.
[23] Morice AH,Jakes AD,Faruqi S,et al. A worldwide survey of chronic cough:a manifestation of enhanced somatosensory response [J]. Eur Respir J,2014,44(5):1149-1155.
[24] Everett CF,Kastelik JA,Thompson RH,et al. Chronic persistent cough in the community:a questionnaire survey [J]. Cough,2007,3:5.
[25] 杨存珍,陈如冲,李斌恺,等.女性慢性咳嗽患者生活质量及尿失禁调查[J].中华哮喘杂志:电子版,2010,4(4):252-255.
[26] 宗岩.从肝论治女性更年期咳嗽变异性哮喘54例[J].江苏中医药,2014(8):42-43.
(收稿日期:2020-07-16)
[基金项目] 中国中医科学院广安门医院国家中医临床研究示范基地科研专项暨所级科研基金课题(2014S282)。
通讯作者
猜你喜欢
成都中医药大学学报(2022年2期)2022-07-09
中华养生保健(2020年5期)2020-11-16
湖南中医药大学学报(2020年7期)2020-08-12
健康必读·下旬刊(2020年1期)2020-01-17
医学信息(2019年20期)2019-12-02
医学信息(2019年6期)2019-06-09
云南中医中药杂志(2018年6期)2018-12-27
中国社区医师(2018年20期)2018-12-11
中国民族民间医药·下半月(2018年4期)2018-09-18
云南中医中药杂志(2015年4期)2015-08-20