
Estimating the weight of children in Nepal by Broselow, PAWPER XL and Mercy method
2018-09-03 03:29KarunShresthaPrakritiSubediOshnaPandeyLikhitaShakyaKailashChhetriDarleneHouse
Karun Shrestha, Prakriti Subedi, Oshna Pandey, Likhita Shakya, Kailash Chhetri, Darlene R. House,
1 Department of General Practice and Emergency Medicine, Patan Academy of Health Sciences, Lalitpur, Nepal
2 Department of Emergency Medicine, Indiana University School of Medicine, Indianapolis, IN, USA
KEY WORDS: Child; Resuscitation; Anthropometry; Nepal
INTRODUCTION
Pediatric care requires an accurate weight for medication dosing, fluid resuscitation and appropriate equipment sizes. In emergencies, delaying resuscitation while weighing a child is impractical. Additionally,current practice using parental weight estimations or agebased formulas can be inaccurate.[1–6]An accurate weight estimate is therefore critical for management of pediatric emergencies.
Length-based weight estimation methods such as the Broselow tape have been validated and widely used in developed countries; however, recent studies in both developing and developed countries have shown the Broselow tape to lack sufficient accuracy for weight estimation.[7–9]Additionally, it has previously been argued that the use of Broselow tape can improve patient care with provided pre-calculated medication dosages and equipment sizes for estimated weights to reduce physician error and alleviate stress during pediatric resuscitations.[10,11]However, a recent meta-analysis done by Wells et al[9]has found insufficient evidence to suggest that it reduced errors or contained sufficient drug dosing information for resuscitations. With these recent studies, the Broselow tape is undergoing scrutiny regarding continued use for weight estimation,especially with newer length- and habitus-based systems demonstrating better accuracy over the Broselow tape,especially in developing countries where there are high levels of malnutrition.[9,12]
These newer methods that utilize length and habitus like PAWPER tape and Mercy method have been shown to be effective in developing countries.[13–15]The second generation PAWPER XL model has been shown to be more accurate than the previous version of PAWPER tape and said to have potential to be accurate across a wide variety of populations.[16]However, only a few studies have evaluated these methods in developing countries like Nepal, where malnutrition is prevalent(stunted 36%, wasted 10% and underweight 27%).[17–21]To our knowledge, no studies have been done to evaluate weight estimation methods in Nepal.
Therefore, the objective of this study is to evaluate the accuracy of Broselow tape, PAWPER XL tape,and Mercy method for weight estimation of Nepalese children visiting the emergency department and underfourteen clinic of Patan Hospital.
METHODS
A prospective, cross-sectional study was conducted from June 2017 through November 2017 to assess the accuracy of the Broselow tape, PAWPER XL tape, and Mercy method in estimating weight among pediatric patients presenting to Patan Hospital in Kathmandu,Nepal. The study received ethical approval from Institutional Review Committee- Patan Academy of Health Sciences (IRC-PAHS).
The study included children presenting to the emergency department and under-14 clinic at Patan Hospital, Nepal. All children under 14 years of age were eligible for the study. A standard weight was measured using the calibrated weight scale with patients wearing light clothing (defined as one layer of clothes) to the nearest 0.1 kg. A calibrated digital infant scale with accuracy to 0.1 kg was used for infants and a digital standing scale with accuracy to 0.1 kg was used for older children. Heavy outer clothing and shoes were removed.The estimated weight was measured by Broselow tape,PAWPER XL tape, and Mercy method.
A trained researcher measured all children. If children required immediate evaluation, measurements were taken after evaluation or stabilization. One investigator collected the demographic information (age and gender) and measured the estimated weight via the three different weight estimation methods. This data was recorded on a data collection form. A second investigator,blinded to age and estimated weight took the actual weight via the calibrated scale and recorded the actual weight on the data collection form.
The Broselow-Luten 2007, edition B, available in Nepal at the time of research was used. The child was laid supine on the bed and measurements were taken from head to heel. The zones on the Broselow tape were numbered with each numbered zone corresponding to an estimated weight. The person taking measurements was blinded to the relationship between the number and estimated weight. The number on the tape into which the child’s length fell was recorded. When entering the data for analysis, the numbered zone recorded was decoded and the Broselow tape estimated weight corresponding to that numbered zone was entered.
Patients were also measured according to the PAWPER XL tape by measuring in the supine position from head to heel. An estimate was then made according to length and visual assessment of body habitus according to body habitus pictures and instructions provided with the PAWPER XL tape (1 – very thin or under weight, 2 – slim, petite, small, 3 – average,normal, 4 – chubby, over weight, 5 – obese, 6 and 7 –severely obese). Weight adjustment was made according to the body habitus score on the tape per tape usage instructions.[22]
For the Mercy method, humeral length was measured from the upper edge of the posterior border of the acromion process to the tip of the olecranon process with the arm hanging down and the elbow positioned at a 90°angle. Mid-upper arm circumference was measured at the midpoint of the humerus with the arm hanging down at the child’s side. The humerus length and the mid upper arm circumference were measured and added together to give the estimated weight.[23]
Statistical analysis
To detect a 5% difference between the actual weights and Broselow estimated weight, each of the 9 categories on the Broselow tape required a sample size of 73 children, with a minimum aggregate sample of 657 children. This also provides an adequate sample size for the PAWPER XL and Mercy method analysis. A Bland-Altman analysis was performed to determine the limits of agreement between the different methods of weight measurement. The mean percentage error (MPE) for overall estimation bias, limits of agreement (LOA), and the root mean squared percentage error (RMSPE) for the estimation of precision were calculated. The difference between the actual weight and the estimated weights was calculated in terms of percentage error; and therefore, a negative value for MPE indicates overestimation while a positive value indicates underestimation of the actual weight. Additionally, the percentage of weight estimation within 10% and 20% were calculated for overall accuracy (PW10 and PW20).
RESULTS
The study included 813 children with an adequate sample size in each Broselow category. The mean age was 4.2 years (ranging from 4 days to 14 years), mean weight 15.8 kg with 60% male. The demographic variables by weight categories and habitus are summarized in Table 1. Only one child in the study required urgent resuscitation and stabilization before obtaining weight estimation measurements.
The mean percentage error (MPE) was lowest for PAWPER XL at 0.7 % (10.5) followed by –1.0% (11.8)for Broselow and 4.2% (11.9) for Mercy. The root mean squared percentage error (RMSPE) was lowest for PAWPER XL at 10.6% followed by 11.8% for Broselow and 12.7% for Mercy. The predicted weight within the PW10 was highest for the PAWPER XL tape at 71.5%followed by 63.2% for Broselow and 58.1% for Mercy.Similarly for the predicted weight within PW20 of actual weight, it was 95.2%, 91.5% and 91.3% for PAWPER XL,Broselow and Mercy respectively (Table 2). A Bland Altman plot was done to evaluate the agreement between the actual weight and the mean percentage error (MPE)for each method (Figure 1).
Color zone estimation for Broselow tape was thesame zone as the actual weight in 60.3% of patients.Otherwise, Broselow tended to overestimate by one color zone. However, the Broselow tape was not applicable in 34 children in our study due to the tape’s limited length of 142 cm.

Table 1. Patient demographics

Table 2. Measures of bias, precision, and accuracy for methods of weight estimation
DISCUSSION
To our knowledge, this study provides the first evidence that the PAWPER XL tape provides the most accurate weight estimation of children in Nepal.
PAWPER XL
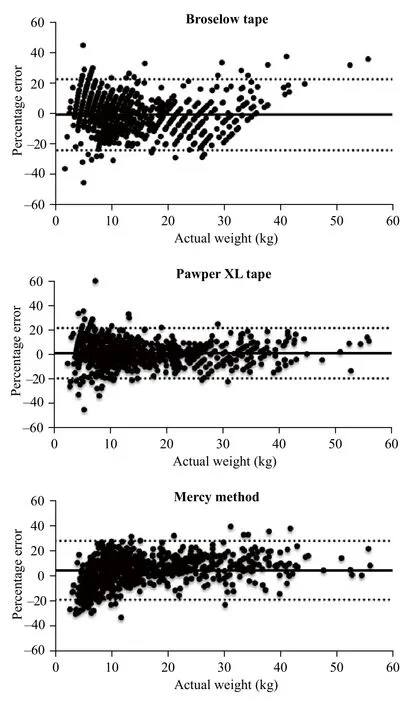
Figure 1. Bland Altman plots of percentage error for actual weights.The solid line represents the mean percentage error and the dotted lines represent the 95% limits of agreement.
The PAWPER XL tape was the only weight estimation method that met the minimum criteria for accuracy in Nepal. Overall, the PAWPER XL tape had better precision and accuracy with a lower bias than the other methods evaluated. Accuracy remained high for children weighing over 20 kg unlike the other methods.Our results were similar to Wells et al[16]evaluation of the PAWPER XL tape, although not as accurate which may be either due to our study population or primary use of the body habitus with no use of the mid-arm circumference. There are only few studies validating the use of new PAWPER XL tape and its accuracy.[22]Therefore,our fi ndings further support its accuracy for use in weight estimation of children in developing countries like Nepal.
The PAWPER XL tape had the best accuracy for children with a body habitus score of <3, which was a significant portion of our study population, indicating that the addition of a body habitus score may allow for improved weight estimation accuracy in thin or underweight children. Similarly, the meta-analysis of studies done with the PAWPER tape in developing countries found PAWPER to out-perform the other weight estimation methods.[24]This provides further evidence that the PAWPER XL tape may be the best weight estimation method in developing countries due to the included habitus assessment.
BROSELOW tape
The Broselow tape only had moderate accuracy for weight estimation in Nepal. This is consistent with other studies, including both recent meta-analysis evaluating weight estimation methods in developing countries and the Broselow tape alone.[9,24]In general, the Broselow tape has shown to be less accurate compared to newer length- and habitus-based systems such as the Mercy method and the PAWPER tape.[9]While the Broselow tape performed better than Mercy method in this study,neither met the acceptable standard for accuracy in our study. Additionally, the length of the Broselow tape at 142 cm limits its use in the pediatric population while the other methods were able to give estimations for all patients. It was believed that the Broselow tape was advantageous as it provides pre-calculated drug dosages and equipment sizes; however, recent reviews have shown the tape to provide incomplete information to function as an adequate resuscitation aid.[9,25]Therefore,Broselow tape lacks the accuracy to be used here in Nepal as in many other parts of the world.
Mercy method
In our study, the Mercy method performed the worst among the three tapes with the lowest precision and accuracy. Our finding is contradictory to other studies,which have shown Mercy method to be accurate.Many of the previous studies showed that Mercy tape performed better than Broselow tape for weight estimation.[21,26]Batmanabane et al[20]found the Mercy tape performed extremely well for children in India with predicted weights within 10% and 20% for 70% and 96% of enrolled children respectively. Similarly, the study done in Mali by Dicko et al[19]demonstrated that the Mercy method offered the best accuracy compared to Broselow and age-based estimations, with estimated weights within 20% of actual for 97% of the children.
Our study, however, found that the Broselow tape performed slightly better than the Mercy tape. This may be due to the complexity of calculation that involves addition of two measurements (MUAC and humeral length). The requirement of two measurements and addition could give rise to human error, which is our aim to avoid when estimating weights during resuscitations.
Future studies further validating weight estimation methods, especially the PAWPER XL tape as the only method with acceptable accuracy in this study, need to be performed in other areas of Nepal. Additionally, in order to implement application of these weight estimation methods, distributors need to make these tapes more easily accessible in resource-limited settings. With improved availability, further study as to the impact of implementation of the PAWPER XL tape with the associated Flipper card, a quick reference for pediatric drug dosages, on resuscitations would be helpful.
Limitations
This study has several limitations. Not all eligible children presenting to the emergency department and clinic were able to be included in the study due to time constraints of researchers' availability. However, when available, all children during that time frame were included so we believe this is a good representation of the patient population. Also, the study was performed in Kathmandu in a referral center, which may bias our population to those families that have more resources.There may also be more malnutrition in rural settings,which may make these weight estimation methods less valid or make one more valid over the other. Therefore,further studies need to be done in such rural settings to further validate the use of these weight estimation methods in Nepal. Also, due to lack of availability, an older version of the Broselow tape was used, so we cannot comment on the accuracy of the recent version in this population; however, the newer 2011 A version,which was adjusted to reduce underestimation in obese populations, would likely have performed worse than the older version, which has been demonstrated in other low and middle-income countries.[27]Additionally, we had to contact the makers of the Mercy tape and PAWPER tapes to get access to them for this study, highlighting the need for easier accessibility of these methods for implementation into clinical practice in resource-limited settings.
CONCLUSION
The PAWPER XL tape was accurate for predicting the weight of children in Nepal. The Broselow tape and Mercy method were found to be inaccurate for estimating weights, so their use should be avoided in Nepal.
ACKNOWLEDGEMENT
We would like to thank the entire department of General Practice and Emergency Medicine, Patan Academy of Health Sciences.
Funding:None.
Ethical approval:The study received ethical approval from Institutional Review Committee- Patan Academy of Health Sciences (IRC-PAHS).
Conflicts of interest:The authors declare that there are no confl icts of interest regarding the publication of this paper.
Contributors:KS proposed the study, analyzed the data and wrote the first drafts. All authors contributed to the design and interpretation of the study and to further drafts.
 World journal of emergency medicine2018年4期
World journal of emergency medicine2018年4期
- World journal of emergency medicine的其它文章
- Social attitude and willingness to attend cardiopulmonary resuscitation training and perform resuscitation in the Crimea
- Sub-dissociative dose ketamine administration for managing pain in the emergency department
- Effect of sedative agent selection on morbidity,mortality and length of stay in patients with increase in intracranial pressure
- Utility of point-of-care musculoskeletal ultrasound in the evaluation of emergency department musculoskeletal pathology
- Accuracy of abdominal ultrasound for the diagnosis of small bowel obstruction in the emergency department
- Ultrasonographic assessment of paediatric ocular emergencies: A tertiary eye hospital based observation