
心型脂肪酸结合蛋白和N-末端脑钠肽前体在脓毒症心肌损伤中的临床研究
2017-04-01 02:42齐洪娜张建军何佳起王维展李雅琴
中国全科医学 2017年9期
齐洪娜,张建军,何佳起,王维展,李雅琴
·论著·
心型脂肪酸结合蛋白和N-末端脑钠肽前体在脓毒症心肌损伤中的临床研究
齐洪娜1*,张建军2,何佳起1,王维展1,李雅琴1
目的 探讨心型脂肪酸结合蛋白(H-FABP)和N-末端脑钠肽前体(NT-proBNP)在脓毒症心肌损伤早期的表达水平及临床价值。方法 选择2014年6月—2016年3月河北医科大学附属哈励逊国际和平医院急诊重症监护病房(EICU)和重症医学科收住院的诊断为严重脓毒症、脓毒性休克患者98例为研究对象,其中严重脓毒症组50例、脓毒性休克组48例。根据入院时超声心动图(UCG)左心室射血分数(LVEF)将患者分为心肌损伤组(LVEF≤50%)62例和非心肌损伤组(LVEF50%)36例,同期选取体检健康者50例作为对照组。脓毒症患者于入院1、6、24 h,对照组于体检时,取肘静脉血3 ml,检测H-FABP、NT-proBNP、肌钙蛋白I(cTnI)、肌酸激酶同工酶(CK-MB)和肌酸激酶(CK)水平,同时记录急性生理学和慢性健康状况(APACHE)Ⅱ评分。结果 入院1 h,脓毒性休克组H-FABP、NT-proBNP水平和APACHEⅡ评分高于严重脓毒症组(P<0.05);入院6 h,脓毒性休克组H-FABP、NT-proBNP、cTnI水平和APACHEⅡ评分高于严重脓毒症组(P<0.05);入院24 h,脓毒性休克组NT-proBNP、cTnI水平和APACHEⅡ评分高于严重脓毒症组(P<0.05);严重脓毒症组与脓毒性休克组H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分组内入院6 h与入院1 h比较,入院24 h与入院6 h比较,差异均有统计学意义(P<0.05)。入院1 h心肌损伤组H-FABP、NT-proBNP水平和APACHEⅡ评分与非心肌损伤组比较,差异均有统计学意义(P<0.05);入院6 h心肌损伤组H-FABP、NT-proBNP、cTnI、CK-MB、CK水平和APACHEⅡ评分与非心肌损伤组比较,差异均有统计学意义(P<0.05);入院24 h 心肌损伤组NT-proBNP、cTnI、CK-MB、CK水平和APACHEⅡ评分与非心肌损伤组比较,差异均有统计学意义(P<0.05);心肌损伤组H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分入院6 h与入院1 h比较,入院24 h与入院6 h比较,差异均有统计学意义(P<0.05);非心肌损伤组APACHEⅡ评分入院6 h低于入院1 h,入院24 h低于入院6 h(P<0.05)。脓毒症患者H-FABP、NT-proBNP水平与APACHEⅡ评分呈正相关(H-FABP:r1 h=0.353,P1 h<0.001;r6 h=0.256,P6 h=0.011;NT-proBNP:r1 h=0.254,P1 h=0.011;r6 h=0.263,P6 h=0.009)。结论 H-FABP和NT-proBNP对脓毒症心肌损伤的早期诊断、指导临床合理用药具有重要意义。
脓毒症;休克,脓毒性;心肌损伤;脂肪酸结合蛋白质类;N-末端脑钠肽前体
齐洪娜,张建军,何佳起,等.心型脂肪酸结合蛋白和N-末端脑钠肽前体在脓毒症心肌损伤中的临床研究[J].中国全科医学,2017,20(9):1042-1048.[www.chinagp.net]
QI H N,ZHANG J J,HE J Q,et al.Roles for heart-type fatty acid-binding protein and N-terminal probrain natriuretic peptide in myocardium injury in sepsis[J].Chinese General Practice,2017,20(9):1042-1048.
脓毒症是常见的急危重症之一,可引起全身多器官损伤,其中心脏损害最常见,如心律失常和心力衰竭,在严重脓毒症及脓毒性休克死亡患者中,30%~80%归因于心血管系统受损[1]。肌钙蛋白I(cTnI)是目前早期心肌损伤的特异性标志物,其水平在心肌损伤后4~6 h升高。心型脂肪酸结合蛋白(H-FABP)是诊断心肌损伤的早期敏感标志物[2],其水平在心肌缺血后1~3 h升高,有利于心肌缺血损伤的早诊断、早治疗。目前认为心肌损伤、抑制及心功能不全是脓毒症患者N-末端脑钠肽前体(NT-proBNP)水平升高的主要原因[3]。本研究旨在通过分析严重脓毒症和脓毒性休克患者血清H-FABP、NT-proBNP水平变化,观察其在脓毒症患者心肌损伤的早期诊断及预后评估中的价值。
本研究创新点:
(1)心型脂肪酸结合蛋白(H-FABP)和N-末端脑钠肽前体(NT-proBNP)联合检测可为脓毒症合并心肌损伤早期诊断及判断预后提供参考依据,在治疗过程中持续监测其动态变化,可提示患者病情变化。(2)H-FABP水平在脓毒症心肌损伤后1~3 h开始升高,6~8 h达到峰值,12~24 h恢复正常,早于肌钙蛋白I、肌酸激酶同工酶和肌酸激酶,对脓毒症心肌损伤的早期诊断有指导意义。
1 资料与方法
1.1 脓毒症患者纳入标准 符合《2012国际严重脓毒症及脓毒性休克诊疗指南》中的诊断标准[4],且符合下列任何一项的患者:(1)收缩压<90 mm Hg(1 mm Hg=0.133 kPa),或平均动脉压(MAP)<70 mm Hg,或存在需液体复苏或血管活性药物治疗的低血压;(2)存在意识改变;(3)急性少尿(尿量<0.5 ml·kg-1·h-1);(4)存在代谢性酸中毒(pH值<7.35,HCO3-<20 mmol/L),并住院治疗;(5)于发病3 h内入院。
1.2 脓毒症患者排除标准 原有心功能不全、急性或慢性肺心病、急性冠脉综合征、瓣膜性心脏病、糖尿病、慢性肾衰竭等;肿瘤晚期、妊娠、创伤、免疫缺陷病及近3个月内使用过激素或免疫抑制剂者;住院期间诊断不明确且24 h内死亡或放弃治疗者。
1.3 一般资料 选择2014年6月—2016年3月河北医科大学附属哈励逊国际和平医院急诊重症监护病房(EICU)和重症医学科收住院的严重脓毒症、脓毒性休克患者98例为研究对象,均符合纳入标准。严重脓毒症组患者50例,其中肺部感染20例,腹腔感染12例,泌尿系感染8例,其他感染10例。脓毒性休克组患者48例,其中肺部感染22例,腹腔感染10例,泌尿系感染8例,其他感染8例。选取同时期门诊体检健康者50例作为对照组。
同时,根据超声心动图结果,以左心室射血分数(LVEF)≤50%提示合并心肌损伤[5-6],将患者分为心肌损伤组62例,其中男28例、女34例,平均年龄(67.6±5.5)岁,其中肺部感染26例、腹腔感染14例、泌尿系感染10例、其他感染12例;非心肌损伤组36例,其中男16例、女20例,平均年龄(66.9±5.3)岁,其中肺部感染16例、腹腔感染8例、泌尿系感染6例、其他感染6例。心肌损伤组与非心肌损伤组的性别、年龄、感染部位比较,差异均无统计学意义(χ2=0.005,t=0.616,χ2=0.030;P0.05)。
本研究符合医学伦理学标准,经医院伦理委员会批准,并取得所有研究对象的知情同意。
1.4 方法 (1)体检健康者于体检时,患者于入院1、6 、24 h采肘静脉血3 ml,3 000 r/min离心10 min,离心半径16 cm,分离提取血清后置于-80 ℃冰箱备用,应用日立公司生产的7600全自动生化分析仪,检测cTnI、肌酸激酶同工酶(CK-MB)、肌酸激酶(CK)水平;血清H-FABP、NT-proBNP水平采用美国ReLIA生物科技公司SSJ-2型多功能免疫检测仪进行检测,试剂盒选择配套产品,检测范围分别为2~60 μg/L和200~15 000 ng/L,严格按照试剂盒说明书操作。(2)在入院时采用美国GE公司VIVID7型全数字心脏彩色多普勒超声诊断仪检测患者的左心室舒张末期内径(LVEDD)和LVEF,并在入院1、6、24 h行全导心电图检查,明确患者有无心肌缺血改变,同时,连续3次记录急性生理学和慢性健康状况(APACHE)Ⅱ评分情况(如患者死亡则评分终止);体检健康者于体检时记录APACHEⅡ评分。
2 结果
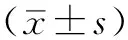
2.1 对照组、严重脓毒症组、脓毒性休克组临床资料比较 对照组、严重脓毒症组、脓毒性休克组的年龄、性别构成、体质指数比较,差异无统计学意义(P0.05);3组收缩压、舒张压比较,差异有统计学意义(P<0.05,见表1)。
表1 对照组、严重脓毒症组、脓毒性休克组临床资料比较
Table 1 Comparison of baseline characteristics in control,severe sepsis and septic shock groups
组别例数年龄(岁)性别(男/女)体质指数(kg/m2)收缩压(mmHg)舒张压(mmHg)对照组5068.5±5.328/2224.9±2.3116±1974±16严重脓毒症组5067.1±5.227/2324.2±2.6 98±20 62±13脓毒性休克组4867.3±5.626/2225.0±2.9 90±18 60±11F(χ2)值1.9630.049a0.94355.17520.592P值0.1670.9760.518<0.001<0.001
注:a为χ2值
2.2 对照组、严重脓毒症组、脓毒性休克组观察指标比较 组别与时间在H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分上均有交互作用(P<0.05);组别在H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分上主效应显著(P<0.05);时间在H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分上主效应显著(P<0.05)。其中,入院1 h,脓毒性休克组H-FABP、NT-proBNP水平和APACHEⅡ评分高于严重脓毒症组,差异有统计学意义(P<0.05);入院6 h,脓毒性休克组H-FABP、NT-proBNP、cTnI水平和APACHEⅡ评分高于严重脓毒症组,差异有统计学意义(P<0.05);入院24 h,脓毒性休克组NT-proBNP、cTnI水平和APACHEⅡ评分高于严重脓毒症组,差异有统计学意义(P<0.05);严重脓毒症组与脓毒性休克组H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分组内入院6 h与入院1 h比较,入院24 h与入院6 h比较,差异均有统计学意义(P<0.05,见表2)。
2.3 心肌损伤组与非心肌损伤组观察指标比较 组别与时间在H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分上均有交互作用(P<0.05);组别在H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分上主效应显著(P<0.05);时间在H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分上主效应显著(P<0.05)。其中,入院1 h心肌损伤组H-FABP、NT-proBNP水平和APACHEⅡ评分与非心肌损伤组比较,差异均有统计学意义(P<0.05);入院6 h心肌损伤组H-FABP、NT-proBNP、cTnI、CK-MB、CK水平和APACHEⅡ评分与非心肌损伤组比较,差异均有统计学意义(P<0.05);入院24 h心肌损伤组NT-proBNP、cTnI、CK-MB、CK水平和APACHEⅡ评分与非心肌损伤组比较,差异均有统计学意义(P<0.05);心肌损伤组H-FABP、NT-proBNP、cTnI、CK-MB、CK水平及APACHEⅡ评分入院6 h与入院1 h比较,入院24 h与入院6 h比较,差异均有统计学意义(P<0.05);非心肌损伤组APACHEⅡ评分入院6 h低于入院1 h,入院24 h低于入院6 h,差异均有统计学意义(P<0.05,见表3)。
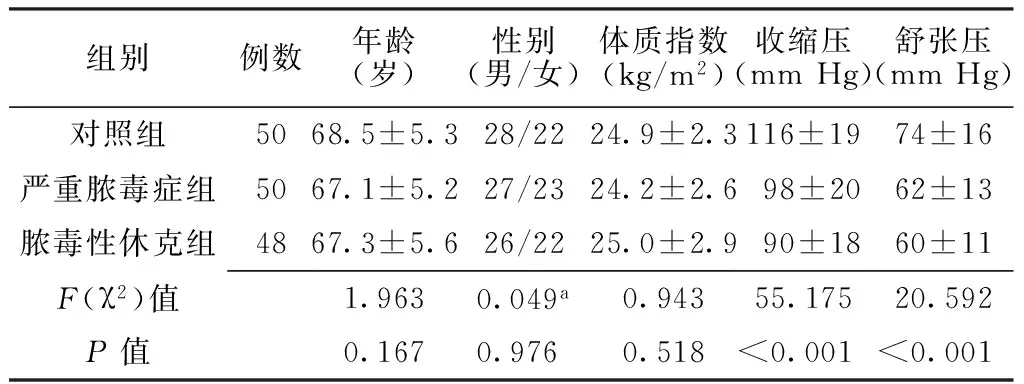
2.4 脓毒症患者H-FABP、NT-proBNP水平与APACHEⅡ评分的相关性 脓毒症患者入院1、6 h H-FABP、NT-proBNP水平与APACHEⅡ评分均呈正相关(H-FABP:r1 h=0.353,P1 h<0.001;r6 h=0.256,P6 h=0.011;NT-proBNP:r1 h=0.254,P1 h=0.011;r6 h=0.263,P6 h=0.009,见图1~4)。
3 讨论
脓毒症是由感染所致的全身炎症反应综合征,病情发展迅速,治疗困难,被认为是急危重症患者的第一位死亡原因[7]。部分脓毒症患者在得到积极有效的治疗后仍难免死亡,其原因在于心律失常、心力衰竭等心肌损伤参与了其病理生理过程,加速了病情的进展,因此,脓毒症合并心肌损伤是导致脓毒症病死率增加的重要原因,而目前对其早期的诊断及严重程度的判断尚无系统指标。

Table 2 Comparion of levels of H-FABP,NT-proBNP,cTnI,CK-MB and CK and APACHEⅡscores in control,severe sepsis and septic shock groups measured at 1 h,6 h and 24 h after admission

组别例数H-FABP(μg/L)1h 6h 24hNT-proBNP(ng/L)1h 6h 24h对照组d504.5±1.04.5±1.04.5±1.0346.8±81.6346.8± 81.6346.8± 81.6严重脓毒症组5024.3±2.735.8±6.2b5.5±0.3c1344.0±518.42244.6± 984.0b2821.4±1063.6c脓毒性休克组4832.4±6.3a45.3±8.1ab5.7±0.9c2165.0±681.2a2892.4±1279.8ab3401.1±1221.1acF值F组间=109.86,F时间=1215.83,F交互=24.11F组间=38.42,F时间=144.06,F交互=9.36P值P组间<0.001,P时间<0.001,P交互<0.001P组间<0.001,P时间<0.001,P交互<0.001组别cTnI(μg/L)1h 6h 24hCK-MB(U/L)1h 6h 24h对照组d0.002±0.0040.002±0.0040.002±0.00414.8±3.114.8±3.114.8±3.1严重脓毒症0.004±0.0050.760±0.370b1.590±0.510c15.6±3.027.5±5.9b40.9±8.4bc脓毒性休克0.003±0.0041.080±0.310ab2.190±0.610ac15.3±5.829.1±6.2b44.1±8.9bcF值F组间=44.01,F时间=719.28,F交互=18.70F组间=4.21,F时间=399.29,F交互=21.64P值P组间<0.001,P时间<0.001,P交互<0.001P组间=0.043,P时间<0.001,P交互=0.028组别CK(U/L)1h 6h 24hAPACHEⅡ评分(分)1h 6h 24h对照组d59.2±13.459.2±13.459.2±13.47.7±0.97.7±0.97.7±0.9严重脓毒症61.2±14.2208.7±65.6b571.7±116.1c23.9±3.319.1±5.0b17.8±4.6c脓毒性休克64.8±16.7225.7±70.4b591.6±110.9c28.4±6.2a25.8±6.6ab22.7±7.8acF值F组间=112.25,F时间=1175.93,F交互=20.31F组间=65.82,F时间=125.81,F交互=10.96P值P组间=0.041,P时间<0.001,P交互=0.032P组间<0.001,P时间<0.001,P交互=0.005
注:H-FABP=心型脂肪酸结合蛋白,NT-proBNP=N-末端脑钠肽前体,cTnI=肌钙蛋白I,CK-MB=肌酸激酶同工酶,CK=肌酸激酶,APACHEⅡ评分=急性生理学和慢性健康状况Ⅱ评分;与严重脓毒症组比较,aP<0.05;与入院1 h比较,bP<0.05;与入院6 h比较,cP<0.05;d表示对照组均为体检时检测所得数据
Table 3 Comparsion of levels of H-FABP,NT-proBNP,cTnI,CK-MB and CK and APACHEⅡscores in myocardium injury and non-myocardium injury groups measured at 1 h,6 h and 24 h after admission

组别例数H-FABP(μg/L)1h 6h 24hNT-proBNP(ng/L)1h 6h 24h心肌损伤组6230.7±6.442.8±8.9b5.7±0.8c1954.7±750.32838.0±923.9b3354.4±1183.2c非心肌损伤组365.5±1.0a5.2±1.1a5.4±1.3356.1±78.6a361.8±80.8a364.1± 70.2aF值F组间=1365.39,F时间=546.64,F交互=535.81F组间=487.72,F时间=14.51,F交互=14.18P值P组间<0.001,P时间<0.001,P交互<0.001P组间<0.001,P时间<0.001,P交互<0.001组别cTnI(μg/L)1h 6h 24hCK-MB(U/L)1h 6h 24h心肌损伤组0.004±0.0061.040±0.350b2.040±0.620c15.3±5.329.2±6.4b43.5±9.5c非心肌损伤组0.002±0.0050.002±0.004a0.003±0.001a15.6±2.915.3±2.7a15.1±2.6aF值F组间=518.05,F时间=254.76,F交互=254.62F组间=375.52,F时间=117.98,F交互=126.73P值P组间<0.001,P时间<0.001,P交互<0.001P组间<0.001,P时间<0.001,P交互<0.001组别CK(U/L)1h 6h 24hAPACHEⅡ评分(分)1h 6h 24h心肌损伤组65.1±15.7226.2±69.4b588.0±111.8c27.3±6.224.3±6.6b21.8±7.2c非心肌损伤组59.6±14.761.0±12.4a59.0± 9.9a24.1±2.8a19.1±5.5ab17.5±5.0acF值F组间=10006.90,F时间=425.81,F交互=428.90F组间=29.91,F时间=225.48,F交互=11.64P值P组间<0.001,P时间<0.001,P交互<0.001P组间<0.001,P时间<0.001,P交互<0.001
注:与心肌损伤组比较,aP<0.05;与入院1 h比较,bP<0.05;与入院6 h比较,cP<0.05
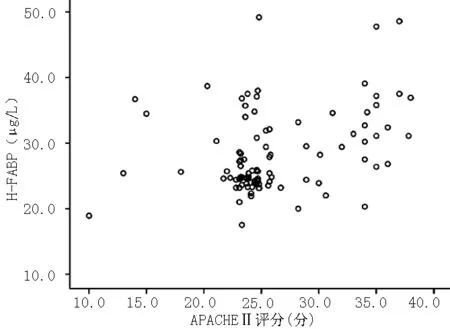
图1 脓毒症患者入院1 h H-FABP水平与APACHEⅡ评分关系的散点图
Figure 1 Scatter plot of correlation between H-FABP and APACHE Ⅱ score in sepsis patients measured at 1 h after admission
注:H-FABP=心型脂肪酸结合蛋白,APACHEⅡ评分=急性生理学和慢性健康状况Ⅱ评分
脓毒症早期就已经存在心肌器质性损伤,易伴发低血压、心力衰竭和心律失常,WITTHAUT等[8]研究发现,约有25%的脓毒症和50%的脓毒症休克患者LVEF降低,1/6有严重的心肌运动功能障碍,因此早期诊断脓毒性心肌损伤及其合并症,并采取积极的防治策略有助于降低脓毒症患者的病死率。目前认为脓毒症患者心肌损伤的原因可能与下列因素相关[9]:(1)心肌抑制因子可影响心肌细胞的兴奋-收缩耦联,同时降低β肾上腺素能受体反应性及心肌收缩力,从而影响心脏功能;(2)线粒体功能障碍,进而使心脏功能受损,严重时可导致心脏衰竭;(3)血液循环与微循环功能障碍,引起心脏充盈不足导致心排血量减少,进而导致心肌组织的氧供失衡,心肌间质水肿降低心脏的顺应性和收缩功能;(4)心肌细胞内钙稳态失衡,引起心肌收缩、舒张功能障碍。cTnI是心肌特有的调节蛋白,是目前诊断心肌损伤的标志物,在心肌损伤后4~6 h才可检测出,18~24 h达高峰,因此,在心肌损伤早期寻找敏感标志物尤为重要。研究发现,脓毒症患者cTnI的检测有助于临床早期诊断是否合并心肌损伤,且cTnI水平升高程度与病变严重程度密切相关[10]。本研究显示,严重脓毒症组及脓毒性休克组患者血清CK-MB水平在入院6、24 h均较入院1 h有不同程度升高,且心肌损伤组高于非心肌损伤组,但CK-MB作为心肌损伤的指标,其特异性较差,对心肌微小损伤不敏感。

图2 脓毒症患者入院6 h H-FABP水平与APACHEⅡ评分关系的散点图
Figure 2 Scatter plot of correlation between H-FABP and APACHE Ⅱ score in sepsis patients measured at 6 h after admission

注:NT-proBNP=N-末端脑钠肽前体
图3 脓毒症患者入院1 h NT-proBNP水平与APACHEⅡ评分关系的散点图
Figure 3 Scatter plot of relationship between NT-proBNP and APACHE Ⅱ score in sepsis patients measured at 1 h after admission

图4 脓毒症患者入院6 h NT-proBNP水平与APACHEⅡ评分关系的散点图
Figure 4 Scatter plot of relationship between NT-proBNP and APACHE Ⅱ score in sepsis patients measured at 6 h after admission
H-FABP是心肌固有的小分子量细胞质蛋白,主要存在于心室肌中。当心肌细胞缺血、缺氧时,机体动员脂肪酸供能,心肌细胞内H-FABP水平升高[11],迅速释放入血,其血清水平升高时间较cTnT、CK-MB更早,急性心肌梗死(AMI)发病后1~3 h开始升高,6~8 h达到峰值,12~24 h恢复正常[12]。在AMI早期诊断及预后评估心肌梗死范围及心肌早期微损伤、评价心肌再灌注等方面,H-FABP具有较高的灵敏度和特异度[13-14]。本研究显示,入院6 h,严重脓毒症组与脓毒性休克组H-FABP、NT-proBNP、cTnI水平较入院1 h有不同程度的升高,且脓毒性休克组患者高于严重脓毒症患者,说明不同程度的脓毒症患者存在不同程度的心肌损伤。入院24 h,严重脓毒症组与脓毒性休克组H-FABP水平较入院6 h下降。
有研究显示,血浆脑钠肽(BNP)、NT-proBNP水平与左心室的收缩和舒张功能障碍、左心室扩张或肥厚、肺动脉高压及瓣膜性心脏病密切相关[15]。脓毒症尽管存在心肌损伤,但NT-proBNP在脓毒症中的作用目前尚未明确,本研究选择NT-proBNP作为观察指标,主要是因为与BNP相比,NT-proBNP具有t1/2长、个体差异较小和体外稳定性好等优点,其作为早期心肌损伤的标记物更为敏感。然而,NT-proBNP对心肌损伤没有呈现出高度的组织或临床特异性,在非心源性心肌损伤时也升高,因此,本研究将H-FABP和NT-proBNP两者联合检测心肌损伤。刘娟等[16]对480例重症监护病房危重患者的临床资料进行分析,认为NT-proBNP水平是危重病患者发生死亡事件的独立危险因素。本研究显示,无论是重症脓毒症还是脓毒性休克患者,心肌损伤组的H-FABP、NT-proBNP水平均高于非心肌损伤组,说明对于脓毒症患者早期检测H-FABP和NT-proBNP是很有意义的,在一定程度上可以反映有无心肌损伤及心肌损伤的程度。APACHEⅡ评分系统是目前国际上应用最广泛的反映危重症病情严重程度的良好指标之一,与患者预后和实际病死率呈正相关[17]。APACHEⅡ评分常取24 h内最差值,但KATAN等[18]认为,如果早期评估则意义更大,因为可以最大限度清除治疗对评价结果的影响或干扰,目前进行动态评分来预测病死率。本研究结果显示,心肌损伤组APACHEⅡ评分明显高于非心肌损伤组。
本研究通过检测H-FABP和NT-proBNP这两种生物标志物发现,心肌损伤组H-FABP、NT-proBNP水平均高于非心肌损伤组,脓毒性休克患者较严重脓毒症患者H-FABP和NT-proBNP水平增加明显,且H-FABP、NT-proBNP水平升高早于cTnI、CK-MB和CK,对早期诊断及治疗有指导意义。随着脓毒症病情程度的增加,早期H-FABP、NT-proBNP水平逐渐升高,二者水平与APACHEⅡ评分呈正相关。本研究结果在一定程度上提示H-FABP、NT-proBNP水平可反映脓毒性心肌损伤程度并能评估预后转归情况。
综上所述,H-FABP和NT-proBNP可作为脓毒症合并心肌损伤早期诊断的指标并为预后判断提供参考依据,在患者治疗过程中持续监测其动态变化,以提示病情变化,及时对治疗方案进行调整,对指导临床用药有重要意义。相对于其他脏器,脓毒性心肌损伤的研究尚不深入,尚需进一步的临床研究来阐明其发生机制,进而探索预防及保护措施,对降低脓毒症病死率提供临床指导。
作者贡献:齐洪娜进行试验设计及实施、撰写论文并对文章负责;张建军、何佳起、李雅琴进行试验实施、评估及资料搜集;王维展进行质量控制及审校。
本文无利益冲突。
[1]WERDAN K,SCHMIDT H,EBELT H,et al.Impaired regulation of cardiac sepsis,SIRS,and MODS[J].Can J Physiol Pharmacol,2009,87(4):266-274.
[2]MCMAHON C G,LAMONT J V,CURTIN E,et al.Diagnostic accuracy of heart-type fatty acid-binding protein for the early diagnosis of acute myocardial infarction[J].Am J Emerg Med,2012,30(2):267-274.
[3]刘娟.N端B型脑钠肽在脓毒症中的研究进展[J].中国医师杂志,2013,15(6):861-864. LIU J.Research progress of N type B brain natriuretic peptide in sepsis[J].Journal of Chinese Physician,2013,15(6):861-864.
[4]高戈,冯喆,常志刚,等.2012国际严重脓毒症及脓毒性休克诊疗指南[J].中华危重病急救医学,2013,25(8):501-505. GAO G,FENG Z,CHANG Z G,et al.2012 international guidelines for the diagnosis and treatment of severe sepsis and septic shock[J].Chin Crit Care Med,2013,25(8):501-505.
[5]高雪花,曹雯,关银,等.艾司洛尔对脓毒症患者心肌损伤的保护作用[J].中国急救医学,2015,35(8):678-682. GAO X H,CAO W,GUAN Y,et al.Protective effect of esmolol on myocardial injury in septic patients[J].Clin J Crit Care Med,2015,35(8):678-682.
[6]POST F,WEILEMANN L S,MESSOW C M,et al.B-type natriuretic peptide as a marker for sepsis-induced myocardial depression in intensive care patients[J].Crit Care Med,2008,36(11):3030- 3037.DOI:10.1097/CCM.0b013e31818b9153.
[7]李振华,董磊,王国兴,等.脑利钠肽、肌钙蛋白T和I监测对重症脓毒症和脓毒症休克预后的意义[J].中华急诊医学杂志,2012,21(9):1016-1021. LI Z H,DONG L,WANG G X,et al.Prognostic value of monitoring B-type natriuretic peptide,cardiac troponin T and troponin I in severe sepsis and septic shock[J].Chin J Emerg Med,2012,21(9):1016-1021.
[8]WITTHAUT R,BUSCH C,FRAUNBERGER P,et al.Plasma atrial natriuretic peptide and brain natriuretic peptide are increased in septic shock:impact of interleukin-6 and sepsis-associated left ventricular dysfunction[J].Intensive Care Med,2003,29(10):1696-1702.DOI:10.1007/s00134-003-1910-0.
[9]闫丽梅.脓毒症休克患者心肌损伤程度及预后判断的研究[J].中国医师进修杂志,2014,37(10):36-39. YAN L M.Clinical study on evaluation of severity of sepsis shock patients with myocardium injury[J].Chin J Postgrad Med,2014,37(10):36-39.
[10]郭俊,王夜明.脓毒症患者血清降钙素原与心肌肌钙蛋白I水平的相关性研究[J].中国中西医结合急救杂志,2015,22(5):527-530. GUO J,WANG Y M.Correlation between serum procalcitonin and cardiac troponin I in patients with sepsis[J].Chin J TCM WM Crit Care,2015,22(5):527-530.
[11]KOSSAIFY A,GARCIA A,SUCCAR S,et al.Perspectives on the value of biomarkers in acute cardiac care and implications for strategic management[J].Biomark Insights,2013,8:115-126.DOI:10.4137/BMI.S12703.
[12]AZZAZY H M,PELSERS M M,CHRISTENSON R H.Unbound free fatty acids and heart-type fattty acid-binding protein:diagnostic assays and clinical applications[J].Clin Chem,2006,52(1):19-29.
[13]CAPPELLINI F,DA MOLIN S,SIGNORINI S,et al.Heart-type fatty acid-binding protein may exclude acute myocardial infarction on admission to emergency department for chest pain[J].Acute Card Care,2013,15(4):83-87.DOI:10.3109/17482941.2013.8 41947.
[14]REITER M,TWERENBOLD R,REICHLIN T,et al.Heart-type fatty acid-binding protein in the early diagnosis of acute myocardial infraction[J].Heart,2013,99(10):708-714.DOI:10.1136/heartjnl-2012-303325.
[15]BHALLA V,ISAKSON S,BHALLA M A,et al.Diagnostic ability of B-type natriuretic peptide and impedance cardiography:testing to identify left ventricular dysfunction in hypertensive patients[J].AM J Hypertens,2005,18(2 Pt 2):73S-81.DOI:10.1016/j.amjhyper.2004.11.044.
[16]刘娟,张熙春,刘运东,等.重症监护病房患者血清N末端B型利钠肽水平对预后评估的意义[J].中华危重病急救医学,2014,26(7):489-492. LIU J,ZHANG X C,LIU Y D,et al.The significance of serum N-terminal pro-brain natriuretic peptide levels for prognosis of patients in intensive care unit[J].Chin Crit Care Med,2014,26(7):489-492.
[17]NAVED S A,SIDDIGUI S,KHAN F H.APACHE-Ⅱ score correlation with mortality and length of stay in an intensive care unit[J].J Coll Physicians Surg Pak,2011,21(1):4-8.DOI:01.2011/JCPSP.0408.
[18]KATAN M,MORGENTHALER N,WIDMER I,et al.Copeptin,a stable peptide derived from the vasopressin precursor,correlates with the individual stress level[J].Neuro Endocrinol Lett,2008,29(3):341-346.
(本文编辑:赵跃翠)
Roles for Heart-type Fatty Acid-binding Protein and N-terminal Probrain Natriuretic Peptide in Myocardium Injury in Sepsis
QIHong-na1*,ZHANGJian-jun2,HEJia-qi1,WANGWei-zhan1,LIYa-qin1
1.DepartmentofEmergency,HarrisonInternationalPeaceHospitalAffiliatedtoHebeiMedicalUniversity,Hengshui053000,China2.DepartmentofIntensiveCareUnit,HarrisonInternationalPeaceHospitalAffiliatedtoHebeiMedicalUniversity,Hengshui053000,China
*Correspondingauthor:QIHong-na,Attendingphysician;E-mail:894582067@qq.com
Objective To investigate the expressions and clinical values of heart-type fatty acid-binding protein (H-FABP) and N-terminal probrain natriuretic peptide (NT-proBNP) in myocardium injury in sepsis.Methods The subjects enrolled in this study were 98 sepsis patients(50 diagnosed with severe sepsis,and 48 with septic shock on admission) who were treated in Emergency Intensive Care Unit(EICU) and Intensive Care Unit of Harrison International Peace Hospital Affiliated to Hebei Medical University from June 2014 to March 2016 and 50 controls underwent physical examination in this hospital during the same period.The 98 sepsis patients were divided into myocardium injury group(62 with value of LVEF≤50%) and non-myocardium injury group(36 with value of LVEF50%) based on the value of left ventricular ejection fraction (LVEF) obtained from the ultrasound cardiogram(UCG) performed on admission.The measurement of H-FABP,NT-proBNP,troponin I(cTnI),creatine kinase isoenzyme (CK-MB) and creatine kinase(CK) in venous blood samples of 3 ml was performed in sepsis patients at 1 h,6 h and 24 h after admission,and in the controls during the physical examination,respectively.And changes in scores of Acute Physiology and Chronic Health Evaluation Ⅱ(APACHE Ⅱ) of all groups were recorded.Results At 1 h after admission,the levels of H-FABP,NT-proBNP and APACHEⅡscore in septic shock group were significantly higher than those in severe sepsis group (P<0.05).At 6 h after admission,the levels of H-FABP,NT-proBNP,cTnI and APACHEⅡscore were higher in septic shock group than in severe sepsis group (P<0.05).At 24 h after admission,septic shock group had higher levels of NT-proBNP,cTnI and APACHEⅡscore than severe sepsis group(P<0.05).In both severe sepsis and sepsis shock groups,the levels of H-FABP,NT-proBNP,cTnI,CK-MB,CK and APACHE Ⅱ scores measured at 1 h after admission differed significantly from those measured at 6 h after admission(P<0.05),and those measured at 6 h after admission also differed remarkably from those measured at 24 h after admission (P<0.05).At 1 h after admission,there were significant differences in the levels of H-FABP,NT-proBNP and APACHEⅡscore between myocardium injury group and non-myocardium injury group (P<0.05).At 6 h after admission,significant differences in the levels of H-FABP,NT-proBNP,cTnI,CK-MB,CK and APACHEⅡscore were observed between myocardium injury group and non-myocardium injury group (P<0.05).At 24 h after admission,the levels of NT-proBNP,cTnI,CK-MB,CK and APACHE Ⅱ score in myocardium injury group differed significantly from those in non-myocardium injury group (P<0.05).In myocardium injury group,there were significant differences in the levels of H-FABP,NT-proBNP,cTnI,CK-MB,CK and APACHE Ⅱ score between 6 h and 1 h after admission(P<0.05),and between at 24 h and 6 h after admission(P<0.05).In non-myocardium injury group,APACHE Ⅱ score measured at 6 h after admission was lower than that measured at 1 h after admission (P<0.05),and that measured at 24 h after admission was lower than that measured at 6 h after admission (P<0.05).In sepsis patients,positive correlations were found between level of H-FABP and APACHE Ⅱ score measured both at 1 h and 6 h after admission (r1 h=0.353,P1 h<0.001;r6 h=0.256,P6 h=0.011);and positive relationship existed between level of NT-proBNP and APACHE Ⅱ score measured both at 1 h and 6 h after admission (r1 h=0.254,P1 h=0.011;r6 h=0.263,P6 h=0.009).Conclusion Values of H-FABPand NT-proBNP are of important reference significance in the early diagnosis and reasonable prescription for myocardium injury in sepsis.
Sepsis;Shock,septic;Myocardium injury;Fatty acid-binding proteins;N-terminal probrain natriuretic peptide
衡水市科学技术研究与发展计划项目(15019)
R 163
A
10.3969/j.issn.1007-9572.2017.09.005
2016-10-10;
2017-01-10)
1.053000河北省衡水市,河北医科大学附属哈励逊国际和平医院急救医学部
2.053000河北省衡水市,河北医科大学附属哈励逊国际和平医院重症医学科
*通信作者:齐洪娜,主治医师;E-mail:894582067@qq.com
猜你喜欢
健康护理(2022年3期)2022-05-26
健康体检与管理(2022年4期)2022-05-13
中国药学药品知识仓库(2022年7期)2022-05-10
现代临床医学(2022年2期)2022-04-19
天津医科大学学报(2021年4期)2021-08-21
中华养生保健(2020年10期)2021-01-18
中华养生保健(2020年4期)2020-11-16
天津医科大学学报(2019年3期)2019-08-13
中国中医急症(2019年10期)2019-05-21
医药前沿(2018年27期)2018-01-16
