法舒地尔治疗老年慢性肺源性心脏病临床疗效及其机制的随机对照研究
2017-02-20 07:23卜丽娜宋爱玲贾卫红杨栋才韩燕燕
中国全科医学 2017年5期
卜丽娜,宋爱玲,贾卫红,杨栋才,韩燕燕
·论著·
法舒地尔治疗老年慢性肺源性心脏病临床疗效及其机制的随机对照研究
卜丽娜*,宋爱玲,贾卫红,杨栋才,韩燕燕
目的 探讨法舒地尔治疗老年慢性肺源性心脏病(CPHD)的临床疗效及其机制。方法 前瞻性选取2014年10月—2015年3月西安市第二医院呼吸内科收治的老年CPHD患者76例为研究对象,采用随机数字表法分为治疗组38例和对照组38例。治疗组在CPHD内科常规药物治疗的基础上给予法舒地尔注射液静脉滴注;对照组在CPHD内科常规药物治疗的基础上给予0.9%氯化钠注射液静脉滴注作为对照,共治疗14 d。治疗前及治疗后测定血压、心率、血气分析〔动脉血氧分压(PaO2)、二氧化碳分压(PaCO2)〕、肺动脉收缩压(sPAP);治疗前及治疗第7、14天检测超敏C反应蛋白(hs-CRP)、N末端脑钠肽前体(NT-proBNP)水平。观察治疗期间不良事件。结果 对照组因心力衰竭死亡1例,脱落率1.3%。治疗前及治疗后,治疗组与对照组患者收缩压、舒张压、心率比较,差异均无统计学意义(P>0.05)。治疗前,治疗组与对照组患者PaO2、PaCO2、sPAP比较,差异均无统计学意义(P>0.05)。治疗后,治疗组较对照组患者PaO2升高,PaCO2、sPAP降低(P<0.05)。hs-CRP、NT-proBNP水平治疗方法与治疗时间存在交互作用(P<0.05),治疗方法主效应显著(P<0.05),治疗时间主效应显著(P<0.05)。治疗前,治疗组与对照组患者hs-CRP、NT-proBNP水平比较,差异均无统计学意义(P>0.05);治疗第7、14天,治疗组患者hs-CRP、NT-proBNP水平较对照组降低(P<0.05)。治疗期间,少数患者出现头昏(治疗组3例,对照组2例)、头痛(治疗组1例,对照组1例)等不适,停药后症状均消失,无其他明显药物不良反应。结论 法舒地尔治疗老年CPHD患者可提高PaO2,降低PaCO2、sPAP、hs-CRP及NT-proBNP水平,不增加不良反应。
肺心病;法舒地尔;C反应蛋白质;利钠肽,脑;随机对照试验
本研究背景:
慢性肺源性心脏病是一种临床上较为常见的心血管疾病,随着我国步入老龄化社会,慢性肺源性心脏病的患病人数日益增多。慢性肺源性心脏病以肺血管阻力进行性升高,血管内膜增生及重构,肺小动脉痉挛、原位微血栓病灶形成等为病理基础。降低肺动脉压是其治疗的重点、难点。但目前降低肺动脉压相关药物治疗老年慢性肺源性心脏病的临床研究却鲜有报道。因此,本研究应用前瞻性、随机对照的方法研究法舒地尔治疗老年慢性肺源性心脏病的安全性及有效性,为老年慢性肺源性心脏病的临床治疗提供科学依据。
肺源性心脏病(pulmonary heart disease,PHD)是指由于支气管、肺组织、肺动脉血管或胸廓等病变导致肺动脉高压,右心室肥大,伴或不伴有右心衰竭的一类心脏病。根据起病缓急和病程长短可分为急性和慢性两类。在我国,慢性肺源性心脏病(chronic pulmonary heart disease,CPHD)占PHD的60%以上,严重影响患者的生活质量。PHD治疗的重点就是降低肺动脉压[1-2]。法舒地尔作为一种Rho激酶抑制剂,国内外多项研究表明该药能有效降低肺动脉压[3-6]。但法舒地尔治疗老年CPHD的临床研究却鲜有报道,我国已步入老龄化社会,老年CPHD患者逐年增多,本研究探讨法舒地尔注射液常规剂量治疗老年CPHD的临床疗效及其机制,为老年CPHD的治疗提供科学依据。
1 资料与方法
1.1 纳入与排除标准 纳入标准:(1)年龄≥60岁;(2)符合1980年第三次全国PHD专业会议制订的PHD诊断标准[7]。排除标准:(1)急性PHD者;(2)合并有严重的脑、肾及血液系统、内分泌系统疾病者;(3)有精神疾病病史,乙醇或者药物滥用史者;(4)因身体健康问题或自身原因不能或不愿配合者。本研究获得了西安市第二医院学术伦理委员会的批准,患者均签署知情同意书。
1.2 一般资料 前瞻性选取2014年10月—2015年3月西安市第二医院呼吸内科收治的老年CPHD患者76例为研究对象,其中男45例,女31例;年龄60~92岁,平均年龄(71±11)岁;身高153~181 cm,平均身高(162±20)cm;体质量48~98 kg,平均体质量(66±33)kg。
1.3 分组 采用随机数字表法分为治疗组38例和对照组38例。两组患者性别、年龄、体质指数(BMI)、吸烟率、病程比较,差异均无统计学意义(P>0.05,见表1)。
表1 对照组与治疗组患者一般资料比较
Table 1 Comparison of general data between control group and treatment group
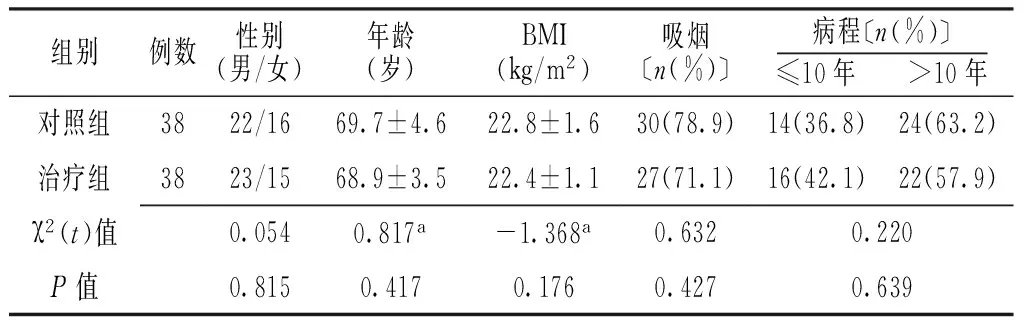
组别例数性别(男/女)年龄(岁)BMI(kg/m2)吸烟〔n(%)〕病程〔n(%)〕≤10年 >10年对照组3822/1669.7±4.622.8±1.630(78.9)14(36.8)24(63.2)治疗组3823/1568.9±3.522.4±1.127(71.1)16(42.1)22(57.9)χ2(t)值0.0540.817a-1.368a0.6320.220P值0.8150.4170.1760.4270.639
注:BMI=体质指数;a为t值
1.4 治疗方法 治疗组给予CPHD内科常规药物治疗(包括吸氧、抗炎、化痰、利尿、强心等),并给予法舒地尔注射液(商品名:川威;天津红日药业股份有限公司生产;批号H20040356;2 ml∶30 mg)30 mg+0.9%氯化钠注射液100 ml静脉滴注60 min,2次/d,治疗14 d。对照组给予CPHD内科常规药物治疗(同治疗组),并给予0.9%氯化钠注射液100 ml作为空白对照静脉滴注60 min,2次/d,治疗14 d。
1.5 观察指标
1.5.1 血压及心率 治疗前及治疗后由专人使用欧姆龙(大连)医用电子血压计HBP-1300测量记录患者的静息血压和心率。
1.5.2 血气分析 治疗前及治疗后使用美国BD公司一次性动脉采血针(REF364314)于桡动脉采血1 ml,美国OPTI CCA-TS便携式血气分析仪检测记录动脉血氧分压(PaO2)、二氧化碳分压(PaCO2)。
1.5.3 超声检查 治疗前及治疗后使用美国Philips iE33型彩色多普勒超声诊断仪检测患者右房室瓣反流压力阶差,估测记录肺动脉收缩压(systolic pulmonary arterial pressure,sPAP),连续测量4个心动周期取平均值。
1.5.4 血液检测 治疗前及治疗第7、14天清晨空腹抽取肘静脉血5 ml,缓慢注入美国BD公司生产的静脉血采集试管(REF366566)中轻轻混匀后,以3 000 r/min离心20 min(离心半径10 cm),分离血浆待测。使用江苏南京Getein1600 全自动荧光免疫定量分析仪检测超敏C反应蛋白(hypersensitive C-reactive protein,hs-CRP)水平。使用美国Biomedica公司的N末端脑钠肽前体(N-terminal pro-brain natriuretic peptide,NT-proBNP)试剂盒,严格按照产品说明书检测NT-proBNP水平。
1.5.5 不良事件 如果两组患者在治疗过程中对药物出现不可耐受的症状、体征时,及时停药,并填写《药物不良反应报告单》上报医院药械科。
2 结果
2.1 血压及心率比较 对照组因心力衰竭死亡1例,脱落率1.3%。共75例患者完成试验:治疗组38例,对照组37例。治疗前及治疗后,治疗组与对照组患者收缩压、舒张压、心率比较,差异均无统计学意义(P>0.05,见表2)。
2.2 PaO2、PaCO2、sPAP比较 治疗前,治疗组与对照组患者PaO2、PaCO2、sPAP比较,差异均无统计学意义(P>0.05)。治疗后,治疗组患者较对照组PaO2升高,PaCO2、sPAP降低,差异均有统计学意义(P<0.05,见表3)。
2.3 hs-CRP、NT-proBNP水平比较 hs-CRP、NT-proBNP治疗方法与治疗时间存在交互作用(P<0.05),治疗方法主效应显著(P<0.05),治疗时间主效应显著(P<0.05)。治疗前,治疗组与对照组患者hs-CRP、NT-proBNP水平比较,差异均无统计学意义(P>0.05);治疗第7、14天,治疗组hs-CRP、NT-proBNP水平较对照组降低,差异均有统计学意义(P<0.05,见表4)。
2.4 不良事件 75例患者试验期间,出现头昏5例(治疗组3例,对照组2例)、头痛2例(治疗组1例,对照组1例)等不适,患者均能耐受,停药后症状均消失。无其他明显药物不良反应。
Table 2 Comparison of blood pressure and heart rate of the patients between control group and treatment group before and after treatment

组别例数收缩压(mmHg)治疗前 治疗后舒张压(mmHg)治疗前 治疗后心率(次/min)治疗前 治疗后对照组37142±11138±1284±781±694±2493±23治疗组38141±13138±1085±584±797±2796±23t值0.5570.0880.8121.7660.4020.605P值0.5790.9300.4190.0820.6890.547

Table 3 Comparison of PaO2,PaCO2and sPAP of the patients between control group and treatment group before and after treatment
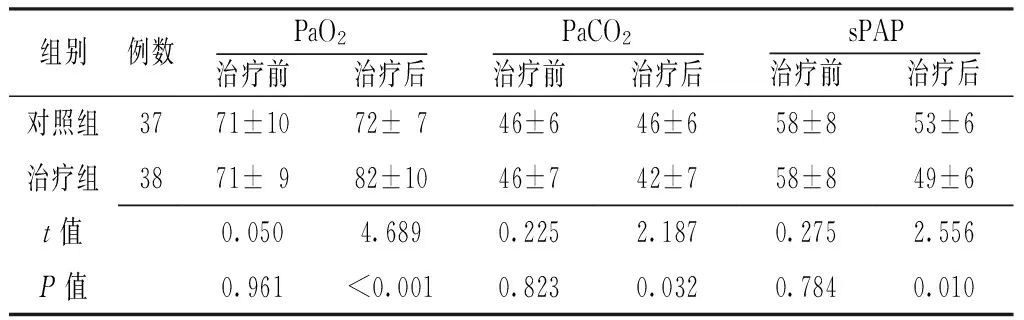
组别例数PaO2治疗前 治疗后PaCO2治疗前 治疗后sPAP治疗前 治疗后对照组3771±1072±746±646±658±853±6治疗组3871±982±1046±742±758±849±6t值0.0504.6890.2252.1870.2752.556P值0.961<0.0010.8230.0320.7840.010
注:PaO2=氧分压,PaCO2=二氧化碳分压,sPAP=肺动脉收缩压
3 讨论
CPHD是一种常见病和多发病,多为各种病因所致的肺动脉高压、右心负荷过重、右心室肥厚,最终引起以右心衰竭为主的一类心脏病。目前以慢性阻塞性肺疾病所致的CPHD最为常见。缺氧、肺动脉血管结构重塑、肺动脉高压形成是CPHD重要的发病机制。随着我国步入老龄社会,CPHD的发病率逐年增高,但CPHD的药物治疗近年来进展缓慢。
表4 对照组与治疗组患者治疗前及治疗后hs-CRP、NT-proBNP水平比较
注:hs-CRP=超敏C反应蛋白,NT-proBNP=N末端脑钠肽前体;与对照组比较,aP<0.05
Rho激酶于1995年被发现[8],属于GTP结合蛋白,主要存在于人体细胞质内,为参与细胞运动的主要激酶。Rho激酶主要作用于肌球蛋白磷酸酶,对其进行磷酸化修饰,提升肌球蛋白轻链磷酸化水平,引起细胞肌动蛋白聚合,对细胞的分裂、收缩、黏附等活动具有重要的调节作用[9-11]。在机体缺血缺氧状态下Rho激酶可被异常激活,减少内皮细胞一氧化氮(NO)合成酶的表达,加速血管痉挛、动脉粥样硬化的进程[12]。Rho激酶可促进心肌细胞异常增长,加速心肌重塑,导致右心室肥厚,这也是CPHD形成的主要原因之一。Rho激酶与缺血性神经元损伤、心肌缺血等病理生理过程密切相关[13]。法舒地尔属于Rho激酶抑制剂,可以增加内皮细胞NO合成酶的表达,促进NO合成,扩张血管;可以降低肌球蛋白轻链磷酸化水平、解除血管痉挛;同时可以减少炎性递质分泌,抗氧自由基,减轻炎性反应等。正是由于这些作用机制,法舒地尔可用于治疗各种血管痉挛、缺血性心脑血管病、肺动脉高压等疾病[14-15]。近年来法舒地尔在冠状动脉痉挛、外周血管痉挛、缺血缺氧性肺动脉高压等疾病中已广泛应用[16-19],但在老年CPHD的研究却鲜有报道。因此,本研究采用前瞻性、随机对照的方法,研究法舒地尔注射液治疗老年CPHD的临床疗效及安全性。
本研究共入选76例老年CPHD患者,其中对照组有1例患者因心力衰竭死亡脱落,最终完成试验75例:治疗组38例,对照组37例。研究结果发现,治疗前及治疗后,治疗组与对照组患者收缩压、舒张压、心率无差异;治疗前,治疗组与对照组患者PaO2、PaCO2、sPAP无差异;治疗后,治疗组患者较对照组PaO2升高,PaCO2、sPAP降低;治疗第7、14天,治疗组较对照组患者hs-CRP、NT-proBNP水平降低。提示法舒地尔注射液常规剂量治疗老年CPHD患者时,可明显改善患者PaO2、PaCO2、sPAP等指标,可提高患者肺部摄氧能力,有效改善患者缺氧,降低肺动脉压,增强肺部呼吸功能,同时该药物的使用对老年患者体循环压力的影响较小。法舒地尔应用7 d后心血管病危险分层指标hs-CRP、NT-proBNP水平降低,可有效减轻炎性反应,降低心血管不良事件的发生,改善预后,且患者耐受性良好,无明显不良反应。提示法舒地尔在治疗老年CPHD患者7 d疗程即可临床获益,其远期临床价值可扩大样本量进一步深入研究。
综上所述,法舒地尔注射液常规剂量治疗老年CPHD临床疗效确切,可一定程度上改善患者缺氧,降低肺动脉压,减轻炎性反应,降低心血管不良事件的发生,安全有效,适合临床推广。
作者贡献:卜丽娜进行研究设计与实施、文章构思、撰写论文、对文章整体负责;宋爱玲进行资料收集;卜丽娜、宋爱玲、韩燕燕进行论文的修订;贾卫红、杨栋才进行质量控制和审校。
本文无利益冲突。
[1]SATOH T,SAJI T,WATANABE H,et al.A phase Ⅲ,multicenter,collaborative,open-label clinical trial of sildenafil in Japanese patients with pulmonary arterial hypertension [J].Circ J,2011,75(3):677-682.
[2]YANAGISAWA R,KATAOKA M,TAGUCHI H,et al.Impact of first-line sildenafil monotreatment for pulmonary arterial hypertension [J].Circ J,2012,76(5):1245-1252.
[3]FUKUMOTO Y,YAMADA N,MATSUBARA H,et al.Double-blind,placebo-controlled clinical trial with a rho-kinase inhibitor in pulmonary arterial hypertension[J].Circ J,2013,77(10):2619-2625.
[4]卢坤琴,陈龙.法舒地尔对COPD合并慢性肺源性心脏病肺动脉高压疗效的临床研究 [J].临床肺科杂志,2012,17 (7):1336-1337.DOI:10.3969/j.issn.1009-6663.2012.07.094. LU K Q,CHEN L.Clinical trial of Rho Kinase Inhibitor Fasudil in COPD patients with chronic pulmonary heart disease and pulmonary artery hypertension [J].Journal of Clinical Pulmonary Medicine,2012,17(7):1336-1337.DOI:10.3969/j.issn.1009-6663.2012.07.094.
[5]唐祖胜,屈红,刘伟.法舒地尔治疗老年舒张性左心衰竭相关性肺动脉高压的有效性及安全性研究[J].中国全科医学,2012,15(17):1988-1990.DOI:10.3969/j.issn.1007-9572.2012.06.068. TANG Z S,QU H,LIU W.Efficacy and safety of fasudil in diastolic left ventricular failure related pulmonary hypertension[J].Chinese General Practice,2012,15(17):1988-1990.DOI:10.3969/j.issn.1007-9572.2012.06.068.
[6]胡燕霞,梅同华,柳毅.法舒地尔治疗慢性阻塞性肺疾病合并肺动脉高压45例[J].中国老年学杂志,2015,35(17):4990-4992.DOI:10.3969/j.issn.1005-9202.2015.17.128. HU Y X,MEI T H,LIU Y.Effects of fasudil on 45 cases in chronic obstructive pulmonary disease complicated with pulmonary arterial hypertension [J].Chinese Journal of Gerontology,2015,35(17):4990-4992.DOI:10.3969/j.issn.1005-9202.2015.17.128.
[7]中华医学会呼吸病学分会.慢性肺源性心脏病临床诊断及疗效判断标准[J].中华结核和呼吸杂志,1980,3(2):23-25. Chinese Thoracic Society.Clinical diagnosis and curative judgment standard of chronic pulmonary heart disease [J].Chinese Journal of Tuberculosis and Respiratory Diseases,1980,3(2):23-25.
[8]LEUNG T,MANSER E,TAN L,et al.A novel serine/threonine kinase binding the Ras-related RhoA GTPase which translocates the kinase to peripheral membranes [J].J Biol Chem,1995,270(49):29051-29054.
[9]ISHIZAKI T,MAEKAWA M,FUJISAWA K,et al.The small GTP-binding protein Rho binds to and activates a 160 kDa Ser/Thr protein kinase homologous to myotonic dystrophy kinase [J].EMBO J,1996,15(8):1885-1893.
[10]BOKU S,NAKAGAWA S,TODA H,et al.ROCK2 regulates bFGF-induced proliferation of SH-SY5Y cells through GSK-3beta and beta-catenin pathway [J].Brain Res,2013,1492:7-17.
[11]SHI J,SURMA M,ZHANG L,et al.Dissecting the roles of ROCK isoforms in stress-induced cell detachment [J].Cell Cycle,2013,12(10):1492-1500.
[12]LI H,PENG W,JIAN W,et al.ROCK inhibitor fasudil attenuated high glucose-induced MCP-1 and VCAM-1 expression and monocyte-endothelial cell adhesion [J].Cardiovasc Diabetol,2012,11:65.
[13]OKAMOTO R,LI Y,NOMA K,et al.FHL2 prevents cardiac hypertrophy in mice with cardiac-specific deletion of ROCK2 [J].FASEB J,2013,27(4):1439-1449.
[14] 佟淑平,杜闻博,哈申高娃.盐酸法舒地尔治疗肺动脉高压的临床疗效观察[J].实用心脑肺血管病杂志,2015,23(2):71-73.DOI:10.3969/j.issn.1008-5971.2015.02.023. TONG S P,DU W B,HA S G W.Clinical effect of fasudil hydrochloride on pulmonary arterial hypertension[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2015,23(2):71-73.DOI:10.3969/j.issn.1008-5971.2015.02.023.
[15]李志伟,薛辉,刘军,等.盐酸法舒地尔对脑血管造影术患者脑血管痉挛及血浆内皮素-1的影响[J].脑与神经疾病杂志,2016,24(1):4-7. LI Z W,XUE H,LIU J,et al.Effect of fasudil on cerebral vscular spasm and plasma endothelin-1 of cerebral angiography subjects[J].Journal of Brain and Nervous Diseases,2016,24(1):4-7.
[16] DONG M,YAN B P,LIAO J K,et al.Rho-kinase inhibition:a novel therapeutic target for the treatment of cardiovascular diseases [J].Drug Discov Today,2010,15(15/16):622-629.
[17]WANG Q M,LIAO J K.ROCKs as immunomodulators of stroke [J].Expert Opin Ther Targets,2012,16(10):1013-1025.
[18]COLLIGRIS B,CROOKE A,HUETE F,et al.Potential role of Rho-associated protein kinase inhibitors for glaucoma treatment[J].Recent Pat Endocr Metab Immune Drug Discov,2012,6(2):89-98.
[19] LIU P,ZHANG H,TANG Y J,et al.Influence of Rho kinase inhibitor Fasudil on late endothelial progenitor cells in peripheral blood of COPD patients with pulmonary artery hypertension[J].Bosn J Basic Med Sci,2014,14(1):40-44.
(本文编辑:陈素芳)
Efficacy and Mechanism of Action of Fasudil in the Treatment of Elderly Patients with Chronic Pulmonary Heart Disease:A Randomized Controlled Study
BULi-na*,SONGAi-ling,JIAWei-hong,YANGDong-cai,HANYan-yan
DepartmentofRespiratoryMedicine,SecondHospitalofXi′an,Xi′an710003,China
Objective To evaluate the efficacy and mechanism of action of fasudil in the treatment of elderly patients with chronic pulmonary heart disease (CPHD).Methods The subjects enrolled in this study were 76 elderly patients with CPHD admitted to Department of Respiratory Medicine,Second Hospital of Xi′an from October 2014 to March 2015 by a prospective method.And they were divided into the treatment group(n=38) and the control group(n=38) by random number table method.Based on the conventional medical therapy,the treatment group additionally received intravenous drip of fasudil injection,and the control group received intravenous drip of 0.9% sodium chloride injection.And the treatment for both groups lasted for 14 days.Blood pressure,heart rate(HR),blood gas analysis〔partial pressure of oxygen(PaO2),partial pressure of carbon dioxide(PaCO2)〕,systolic pulmonary arterial pressure(sPAP) were measured before and after treatment.Levels of hypersensitive C-reactive protein(hs-CRP) and N-terminal pro-brain natriuretic peptide (NT-proBNP) were measured before,at the 7th and 14th days after treatment,respectively.And adverse events occurred during treatment were observed.Results Of the patients in the control group,1 died of heart failure,and 1.3% dropped out of the study.No significantly statistical differences were found in terms of systolic and diastolic blood pressure and HR between the two groups before and after treatment (P>0.05).Before treatment,no significant differences were observed in PaO2,PaCO2and sPAP between the two groups(P>0.05),but after treatment,PaO2was elevated and PaCO2and sPAP were decreased in the treatment group(P<0.05).Treatment method and time exerted interaction effect on levels of hs-CRP and NT-proBNP (P<0.05).Treatment method led to remarkable main effect on levels of hs-CRP and NT-proBNP (P<0.05).Treatment time also had significant main effect on levels of hs-CRP and NT-proBNP(P<0.05).Before treatment,levels of hs-CRP and NT-proBNP in the treatment group did not differ from those in the control group significantly(P>0.05),but at the 7th and 14th days after treatment,levels of hs-CRP and NT-proBNP in the treatment group were lowered (P<0.05).During the treatment,only a few patients had some side effects such as dizziness(3 in treatment group and 2 in control group) and headache(1 in treatment group and 1 in control group),but the symptoms disappeared when the medicine was stopped.Conclusion The treatment of fasudil in regular doses can effectively improve the PaO2,reduce PaCO2,sPAP,levels of hs-CRP and NT-proBNP in elderly patients with CPHD,do not increase adverse reactions.
Pulmonary heart disease;Fasudil;C-reactive protein;Natriuretic peptide,brain;Randomized controlled trial
西安市卫生局科研项目(2012004,J2014009)
R 541.5
A
10.3969/j.issn.1007-9572.2017.05.007
2016-06-21;
2016-12-08)
710003陕西省西安市第二医院呼吸内科
*通信作者:卜丽娜,副主任医师;E-mail:2479140923@qq.com
卜丽娜,宋爱玲,贾卫红,等.法舒地尔治疗老年慢性肺源性心脏病临床疗效及其机制的随机对照研究[J].中国全科医学,2017,20(5):538-542.[www.chinagp.net]
BU L N,SONG A L,JIA W H,et al.Efficacy and mechanism of action of fasudil in the treatment of elderly patients with chronic pulmonary heart disease:a randomized controlled study[J].Chinese General Practice,2017,20(5):538-542.
*Correspondingauthor:BULi-na,Associatechiefphysician;E-mail:2479140923@qq.com
猜你喜欢
基层中医药(2022年5期)2022-10-24
中国典型病例大全(2022年11期)2022-05-13
天津医科大学学报(2021年3期)2021-07-21
世界最新医学信息文摘(2021年12期)2021-06-09
世界科学技术-中医药现代化(2021年12期)2021-04-19
山西中医药大学学报(2020年1期)2020-05-10
中国老年学杂志(2017年18期)2017-09-27
中西医结合心血管病电子杂志(2014年10期)2015-07-20
医学研究杂志(2015年9期)2015-07-01