尿酸与冠心病及血脂指标的关系研究
2016-10-09 04:58宋艳斌蔡高军薛社亮翁伟进
实用心脑肺血管病杂志 2016年8期
宋艳斌,蔡高军,薛社亮,翁伟进
尿酸与冠心病及血脂指标的关系研究
宋艳斌,蔡高军,薛社亮,翁伟进
目的分析尿酸(UA)与冠心病及血脂指标的关系。方法选取2012年12月—2014年12月因“胸闷、胸痛、晕厥症状”于江苏大学附属武进医院心内科就诊的冠心病患者841例作为冠心病组;另选取同期因“胸闷、胸痛、晕厥症状”于江苏大学附属武进医院心内科就诊的健康人129例作为健康对照组。收集并比较两组受试者临床资料,分析冠心病危险因素,比较两组不同性别受试者UA水平及不同UA水平冠心病患者的血脂指标。结果两组受试者总胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)水平比较,差异无统计学意义(P>0.05);冠心病组患者年龄、男性比例、吸烟史阳性率、高血压发生率、糖尿病发生率、UA水平高于健康对照组,高密度脂蛋白胆固醇(HDL-C)水平低于健康对照组(P<0.05)。多因素logistic回归分析结果显示,年龄〔OR=1.076,95%CI(1.054,1.098)〕、吸烟史〔OR=2.168,95%CI(1.283,3.662)〕、高血压〔OR=2.007,95%CI(1.313,3.068)〕、糖尿病〔OR=3.091,95%CI(1.715,5.571)〕是冠心病的危险因素,HDL-C〔OR=0.222,95%CI(0.116,0.426)〕是冠心病的保护因素(P<0.05)。两组男性受试者UA水平比较,差异无统计学意义(P>0.05);冠心病组女性患者UA水平高于健康对照组女性(P<0.05)。冠心病患者UA水平>419 μmol/L者TC、TG、LDL-C水平高于UA水平<288 μmol/L者,HDL-C水平低于UA水平<288 μmol/L者(P<0.05);UA水平>419 μmol/L者TC、TG水平高于UA水平为288~346 μmol/L者,HDL-C水平低于UA水平为288~346 μmol/L者(P<0.05);UA水平为347~419 μmol/L者TC、LDL-C水平高于UA水平<288 μmol/L者(P<0.05);UA水平为347~419 μmol/L者LDL-C水平高于UA水平为288~346 μmol/L者(P<0.05)。结论冠心病患者UA水平较高,且与冠心病的发生、发展及血脂异常有关,但UA不是冠心病的危险因素,而其对冠心病的影响存在性别差异。
冠心病;尿酸;危险因素
宋艳斌,蔡高军,薛社亮,等.尿酸与冠心病及血脂指标的关系研究[J].实用心脑肺血管病杂志,2016,24(8):16-19.[www.syxnf.net]
SONG Y B,CAI G J,XUE S L,et al.Relationship between uric acid and coronary heart disease,blood lipids index[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2016,24(8):16-19.
冠心病是危害人类健康的重大疾病,冠心病的发生与患者性别、高血压、糖尿病、高脂血症、吸烟及遗传因素等有关,其发病机制复杂。尿酸(UA)是机体内核酸嘌呤碱基的代谢产物,其也是男性的抗氧化剂,但UA水平较高会损伤血管内皮功能,并参与炎性反应及血脂过氧化过程。有研究表明,UA与冠心病的发生及严重程度有关,其也是心血管事件的预测因子[1-2]。但也有研究表明,UA与冠心病发生、发展的关系并不确定,其并不是冠心病的独立危险因素[3-4]。目前,UA与冠心病的关系仍存在争议。本研究旨在分析UA与冠心病及血脂指标的关系,现报道如下。
1 资料与方法
1.1一般资料选取2012年12月—2014年12月因“胸闷、胸痛、晕厥症状”于江苏大学附属武进医院心内科就诊的冠心病患者841例作为冠心病组,患者经桡动脉途径6个投射体位冠状动脉造影检查示主要冠状动脉血管狭窄率≥50%,存在急性心肌梗死;另选取同期因“胸闷、胸痛、晕厥症状”于江苏大学附属武进医院心内科就诊的健康者129例作为健康对照组,经冠状动脉造影检查排除冠心病或冠状动脉粥样硬化。排除标准:合并严重感染、肝肾功能不全、恶性肿瘤、营养不良、严重贫血等患者。冠心病组中男564例(67.1%),女277例(32.9%);平均年龄(65.3±11.1)岁。健康对照组中男74例(57.4%),女55例(42.6%);平均年龄(58.4±9.5)岁。
1.2资料收集方法
1.2.1临床资料收集所有受试者的临床资料,包括性别、年龄、吸烟史、高血压及糖尿病发生情况。高血压:采用1999年世界卫生组织(WHO)高血压诊断标准:在未使用抗高血压药物的情况下,非同日测量3次血压,收缩压≥140 mm Hg(1 mm Hg=0.133 kPa)。糖尿病:采用1999年WHO糖尿病专家委员会推荐的诊断标准:(1)具有糖尿病症状(多饮、烦渴多尿、难以解释的体质量减轻),任意时间血糖≥11.1 mmol/L;(2)空腹血糖≥7.0 mmol/L;(3)葡萄糖耐量试验,餐后2 h血糖≥11.1 mmol/L。吸烟史:每天至少1支,连续吸烟1年以上,长期吸烟或戒烟时间短于半年患者。
1.2.2实验室检查指标采集受试者空腹静脉血5 ml,采用日立7060C全自动生化分析仪检测UA水平、血脂指标〔总胆固醇(TC)、三酰甘油(TG)、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)〕。

2 结果
2.1两组受试者一般资料比较两组受试者TC、TG、LDL-C水平比较,差异无统计学意义(P>0.05);冠心病组患者年龄、男性比例、吸烟史阳性率、高血压发生率、糖尿病发生率、UA水平高于健康对照组,HDL-C水平低于健康对照组,差异有统计学意义(P<0.05,见表1)。
2.2冠心病影响因素的多因素logistic回归分析以年龄(赋值:实测值)、男性(赋值:是=1,否=0)、吸烟史(赋值:有=1,无=0)、高血压(赋值:有=1,无=0)、糖尿病(赋值:有=1,无=0)、UA(赋值:实测值)、HDL-C(赋值:实测值)为自变量,以冠心病(赋值:无=0,有=1)为因变量,结果显示,年龄、吸烟史、高血压、糖尿病是冠心病的危险因素,HDL-C是冠心病的保护因素(P<0.05,见表2)。

表1 两组受试者一般资料比较
注:a为t值;UA= 尿酸,TC=总胆固醇,TG=三酰甘油,HDL-C=高密度脂蛋白胆固醇,LDL-C低密度脂蛋白胆固醇
表2冠心病影响因素的多因素logistic回归分析
Table 2Multivariate logistic regression analysis on influencing factors of coronary heart disease

自变量βSEWaldχ2值dfOR(95%CI)P值年龄0.0730.01050.90111.076(1.054,1.098)<0.001性别0.4750.2613.31311.609(0.964,2.685)0.069吸烟史0.7740.2688.36312.168(1.283,3.662)0.004高血压0.6970.21710.34112.007(1.313,3.068)0.001糖尿病1.1290.30114.09813.091(1.715,5.571)<0.001UA0.0000.0010.07111.000(0.998,1.003)0.790HDL-C-1.5060.33220.52110.222(0.116,0.426)<0.001
2.3两组不同性别受试者UA水平比较两组男性受试者UA水平比较,差异无统计学意义(P>0.05);冠心病组女性患者UA水平高于健康对照组女性,差异有统计学意义(P<0.05,见表3)。

Table3ComparisonofUAlevelinmaleandinfemalebetweenthetwogroups
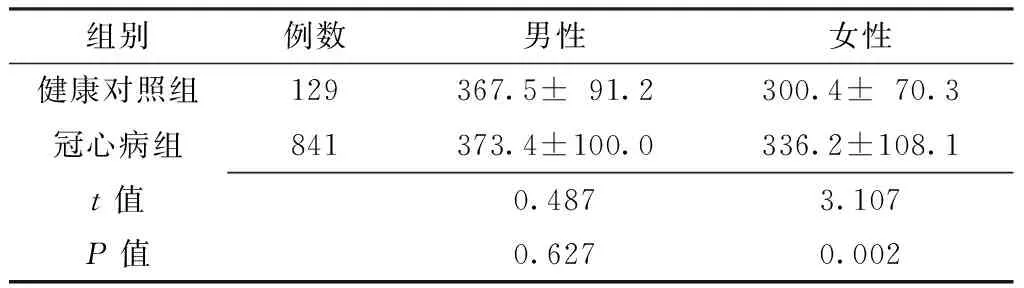
组别例数男性女性健康对照组129367.5±91.2300.4±70.3冠心病组841373.4±100.0336.2±108.1t值0.4873.107P值0.6270.002
2.4不同UA水平冠心病患者血脂指标比较不同UA水平冠心病患者TC、TG、HDL-C、LDL-C水平比较,差异有统计学意义(P<0.05);UA水平>419 μmol/L患者TC、TG、LDL-C水平高于UA水平<288 μmol/L者,HDL-C水平低于UA水平<288 μmol/L者,差异有统计学意义(P<0.05);UA水平>419 μmol/L患者TC、TG水平高于UA水平288~346 μmol/L者,HDL-C水平低于UA水平288~346 μmol/L者,差异有统计学意义(P<0.05);UA水平347~419 μmol/L患者TC、LDL-C水平高于UA水平<288 μmol/L者,差异有统计学意义(P<0.05);UA水平347~419 μmol/L患者LDL-C水平高于UA水平288~346 μmol/L者,差异有统计学意义(P<0.05,见表4)。

Table4ComparisonofbloodlipidsindexincoronaryheartdiseasepatientswithdifferentUAlevels

UA水平(μmol/L)例数TCTGHDL-CLDL-C<2882454.40±0.951.52±1.051.14±0.312.63±0.80288~3462404.47±1.021.62±1.131.14±0.272.73±0.95347~4192424.74±1.18a1.86±1.331.10±0.322.94±1.03ab>4192434.65±1.10ab2.53±0.60ab1.05±0.25abc2.88±0.97aF值5.21444.6305.8085.813P值0.0020.0000.0010.001
注:与<288 μmol/L比较,aP<0.05,与288~346 μmol/L比较,bP<0.05,与347~419 μmol/L比较,cP<0.05
3 讨论
冠状动脉粥样硬化是冠心病发生、发展的病理学基础,其与血管内皮功能紊乱、慢性炎性反应、脂质过氧化、血小板活化等有关。有研究表明,UA可诱导血小板聚集、活化,提高C反应蛋白水平,促进氧化应激及炎性细胞迁移、黏附,加重血管粥样斑块进展,造成斑块不稳定性增加,导致心血管事件的发生[5-6]。雷刚等[7]研究表明,急性心肌梗死患者UA水平高于对照组,多因素分析结果显示,UA是急性心肌梗死的危险因素。沈详聪等[8]分析年轻女性冠心病患者危险因素发现,UA不是冠心病的危险因素。目前,UA是否为冠心病的危险因素尚无定论。BARBIERI等[9]分析性别亚组时发现,UA〔OR=1.29,95%CI(1.03,1.62)〕是女性冠心病患者的危险因素(P=0.03)。有研究通过血管内超声(IVUS)观察患者的冠状动脉病变发现,UA水平与动脉粥样斑块严重程度有关,但无统计学意义[10]。有研究表明,女性亚组中UA水平与冠状动脉内皮功能紊乱有关,而血管内皮功能紊乱与斑块形成有关,其可能是造成性别差异的原因之一[11]。
本研究结果显示,两组受试者TC、TG、LDL-C水平间无差异,冠心病组患者年龄、男性比例、吸烟史阳性率、高血压发生率、糖尿病发生率、UA水平高于健康对照组,HDL-C水平低于健康对照组,与国外相关研究结果一致[12-13],提示UA水平与冠心病有关。本研究多因素logistic回归分析结果显示,年龄、吸烟史、高血压、糖尿病是冠心病的危险因素,HDL-C是冠心病的保护因素,与相关研究结果一致[9,14],提示UA可能通过其他因素影响冠心病的发生、发展。DAI等[15]认为,高尿酸血症与冠心病的发生密切相关,其可能与LDL-C水平较高、HDL-C水平较低有关。本研究结果显示,两组男性受试者UA水平间无差异,冠心病组女性患者UA水平高于健康对照组女性;不同UA水平冠心病患者TC、TG、HDL-C、LDL-C水平间有差异。提示UA水平在冠心病患者中存在性别差异,UA水平较高可使冠状动脉病变进展,且其与LDL-C水平升高、HLD-C水平降低有关。有研究表明,冠状动脉斑块进展过程中UA水平与同型半胱氨酸可能具有协同作用[16],其可抑制NO释放,导致冠状动脉血管内皮细胞损伤[17]。UA水平较高可引起阿司匹林抵抗,导致支架术后再狭窄。目前,UA影响冠心病发生、发展的机制尚不明确,需从分子生物学及遗传学等多角度进行研究。
综上所述,冠心病患者UA水平较高,且与冠心病的发生、发展及血脂异常有关,但UA不是冠心病的危险因素,而其对冠心病的影响存在性别差异。但本研究观察指标不够系统全面,可能存在一定局限性及混杂偏倚,所得结果及结论尚需进一步验证。
作者贡献:宋艳斌进行资料收集整理、撰写论文、成文并对文章负责;蔡高军,薛社亮修改论文;翁伟进进行质量控制及审校。
本文无利益冲突。
[1]SUN Y,YU X,ZHI Y,et al.A cross-sectional analysis of the relationship between uric acid and coronary atherosclerosis in patients with suspected coronary artery disease in China[J].BMC Cardiovasc Disord,2014(14):101.
[2]ZHANG J W,HE L J,CAO S J,et al.Association of serum uric acid and coronary artery disease in premenopausal women[J].PLoS One,2014,9(9):e106130.
[3]ZAND S,SHAFIEE A,BOROUMAND M,et al.Serum uric Acid is not an independent risk factor for premature coronary artery disease.[J].Cardiorenal Medicine,2013,3(4):246-253.
[4]AKIN F,AYÇA B,ÇELIK Ö,et al.Predictors of poor coronary collateral development in patients with stable coronary artery disease:neutrophIL-to-lymphocyte ratio and platelets[J].Anatol J Cardiol,2015,15(3):218-223.
[5]KAWAMOTO R,TOMITA H,OKA Y,et al.Relationship between serum uric acid concentration,metabolic syndrome and carotid atherosclerosis[J].Intern Med,2006,45(9):605-614.
[6]KLEBER M E,DELGADO G,GRAMMER T B,et al.Uric Acid and Cardiovascular Events:A Mendelian Randomization Study[J].J Am Soc Nephrol,2015,26(11):2831-2838.
[7]雷刚,邱健,肖华,等.急性心肌梗死患者血浆致动脉硬化指数、血尿酸水平的变化及临床意义[J].临床军医杂志,2013,41(4):334-337.
[8]沈祥聪,刘恒道,李红军,等.年轻女性冠心病患者相关危险因素及冠状动脉造影特点分析[J].中华临床医师杂志(电子版),2015,9(22):6-11.
[9]BARBIERI L,VERDOIA M,SCHAFFER A,et al.Impact of sex on uric acid levels and its relationship with the extent of coronary artery disease:A single-centre study [J].Atherosclerosis,2015,241(1):241-248.
[10]ANDO K,TAKAHASHI H,WATANABE T,et al.Impact of Serum Uric Acid Levels on Coronary Plaque Stability Evaluated Using Integrated Backscatter Intravascular Ultrasound in Patients with Coronary Artery Disease[J].J Atheroscler Thromb,2016.
[11]KUWAHATA S,HAMASAKI S,ISHIDA S,et al.Effect of uric acid on coronary microvascular endothelial function in women:association with eGFR and ADMA[J].J Atheroscler Thromb,2010,17(3):259-269.
[12]BOZCALI E,POLAT V,ACIKSARI G,et al.Serum concentrations of galectin-3 in patients with cardiac syndrome X[J].Atherosclerosis,2014,237(1):259-263.
[13]YALCIN M,KARDESOGLU E,ISILAK Z,et al.The association between plasma uric acid level and cardiovascular events in patients with stable coronary artery disease:a short-term follow-up study[J].Med Glas (Zenica),2013,10(2):239-243.
[14]DE LUCA G,SECCO G G,SANTAGOSTINO M,et al.Uric acid does not affect the prevalence and extent of coronary artery disease.Results from a prospective study[J].Nutr Metab Cardiovasc Dis,2012,22(5):426-433.
[15]DAI X M,WEI L,MA L L,et al.Serum uric acid and its relationship with cardiovascular risk profile in Chinese patients with early-onset coronary artery disease[J].Clin Rheumatol,2015,34(9):1605-1611.
[16]COHEN E,LEVI A,VECHT-LIFSHITZ S E,et al.Assessment of a possible link between hyperhomocysteinemia and hyperuricemia[J].J Investig Med,2015,63(3):534-538.
(本文编辑:李洁晨)
Relationship between Uric Acid and Coronary Heart Disease,Blood Lipids Index
SONGYan-bin,CAIGao-jun,XUEShe-liang,WENGWei-jin.
DepartmentofCardiology,WujinHospitalAffiliatedtoJiangsuUniversity,Changzhou213017,China
ObjectiveTo analyze the relationship between uric acid and coronary heart disease,blood lipids index.MethodsFrom December 2012 to December 2014,a total of 841 coronary heart disease patients performed as chest distress,chest pain and syncope were selected as case group in the Department of Cardiology,Wujin Hospital Affiliated to Jiangsu University,and a total of 129 healthy people performed as chest distress,chest pain and syncope were selected as control group at the same time.Clinical data of the two groups were collected and compared,and risk factors of coronary heart disease were analyzed;uric acid levels were compared in male and in female between the two groups,and blood lipids index were compared in coronary heart disease patients with different uric acid levels.ResultsNo statistically significant differences of TC,TG or LDL-C was found between the two groups(P>0.05);age,the proportion of male,positive rate of smoking history,incidence of hypertension and diabetes,and uric acid level of case group were statistically significantly higher than those of control group,while HDL-C of case group was statistically significantly lower than that of control group(P<0.05).Multivariate logistic regression analysis showed that,age〔OR=1.076,95%CI(1.054,1.098)〕,smoking history〔OR=2.168,95%CI(1.283,3.662)〕,hypertension〔OR=2.007,95%CI(1.313,3.068)〕and diabetes〔OR=3.091,95%CI(1.715,5.571)〕were risk factors of coronary heart disease,while HDL-C〔OR=0.222,95%CI(0.116,0.426)〕was the protective factor(P<0.05).No statistically significant differences of uric acid level was found in male between the two groups(P>0.05),while uric acid level of case group was statistically significantly higher than that of control group in female(P<0.05).TC,TG and LDL-C of coronary heart disease patients with uric acid level over 419 μmol/L were statistically significantly higher than patients with uric acid level less than 288 μmol/L,while HDL-C was statistically significantly lower than patients with uric acid level less than 288 μmol/L(P<0.05);TC and TG of patients with uric acid level over 419 μmol/L were statistically significantly higher than patients with uric acid level between 288 and 346 μmol/L,while HDL-C was statistically significantly lower than patients with uric acid level between 288 and 346 μmol/L(P<0.05);TC and LDL-C of patients with uric acid level between 347 and 419 μmol/L were statistically significantly higher than patients with uric acid level less than 288 μmol/L(P<0.05);LDL-C of patients with uric acid level between 347 and 419 μmol/L was statistically significantly higher than patients with uric acid level between 288 and 346 μmol/L(P<0.05).ConclusionUric acid level of patients with coronary heart disease is relatively high,and it plays an important role in the occurrence and development of coronary heart disease and dyslipidemia,but it is not one of risk factors of coronary heart disease,while its impact on coronary heart disease exists some gender difference.
Coronary disease;Uric acid;Risk factors
213017江苏省常州市,江苏大学附属武进医院心内科
R 541.4
A
10.3969/j.issn.1008-5971.2016.08.004
2016-03-22;
2016-07-19)
猜你喜欢
中国心血管杂志(2022年2期)2022-11-25
中国心血管杂志(2022年4期)2022-11-25
保健医苑(2021年7期)2021-08-13
中国医学创新(2021年6期)2021-05-10
抗癌(2020年3期)2021-01-16
中国心血管杂志(2021年6期)2021-01-02
中国生殖健康(2019年3期)2019-02-01
中国心血管杂志(2019年3期)2019-01-04
健康大视野(2018年13期)2018-10-31
中西医结合心脑血管病杂志(2016年9期)2016-06-04