
氯吡格雷对急性心肌梗死并心力衰竭患者血清炎性因子水平的影响
2016-06-28 08:38闫巧焕
实用心脑肺血管病杂志 2016年5期
闫巧焕
·药物与临床·
氯吡格雷对急性心肌梗死并心力衰竭患者血清炎性因子水平的影响
闫巧焕
056002河北省邯郸市第一医院老年病一科
【摘要】目的探讨氯吡格雷对急性心肌梗死并心力衰竭患者血清炎性因子水平的影响。方法选取2012年5月—2015年5月邯郸市第一医院收治的急性心肌梗死并心力衰竭患者63例,按照随机数字表法分为观察组32例和对照组31例。对照组患者给予常规治疗,观察组患者在常规治疗基础上给予氯吡格雷治疗,14 d为1个疗程。比较两组患者治疗前及治疗7、14 d血清炎性因子〔肿瘤坏死因子α(TNF-α)、C反应蛋白(CRP)、白介素6(IL-6)及可溶性血管细胞黏附分子1(sVCAM-1)〕水平;并观察治疗期间两组患者不良反应发生情况。结果治疗前两组患者血清TNF-α、CRP、IL-6及sVCAM-1水平比较,差异无统计学意义(P>0.05);治疗7 d、14 d观察组患者血清TNF-α、CRP、IL-6及sVCAM-1水平均低于对照组(P<0.05)。治疗期间两组患者严重出血、轻微出血及中性粒细胞减少发生率比较,差异均无统计学意义(P>0.05)。结论氯吡格雷能有效降低急性心肌梗死并心力衰竭患者血清炎性因子水平,可有效减轻炎性反应,且安全性较高。
【关键词】心肌梗死;心力衰竭;氯吡格雷;炎性因子
闫巧焕.氯吡格雷对急性心肌梗死并心力衰竭患者血清炎性因子水平的影响[J].实用心脑肺血管病杂志,2016,24(5):106-108.[www.syxnf.net]
Yan QH.Influence of clopidogrel on serum inflammatory cytokines levels of acute myocardial infarction patients complicated with heart failure[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2016,24(5):106-108.
急性心肌梗死并心力衰竭是一种心血管急危重症,具有起病急、进展快、病死率高及预后差等特点。临床研究证实,炎症参与了斑块的形成、进展及破溃过程,且炎性细胞聚集贯穿疾病发展过程,因此炎性反应一直是急性心肌梗死并心力衰竭发生机制的研究热点。有研究显示,血流中断和再灌注可使白细胞在心肌内浸润,启动炎症级联反应而释放炎性递质,促进血小板激活,进一步加重心肌损伤[1]。氯吡格雷具有抑制血小板聚集的作用[2],可通过选择性、不可逆地拮抗血小板二磷酸腺苷(ADP)受体而发挥作用。本研究通过观察氯吡格雷对急性心肌梗死并心力衰竭患者血清炎性因子水平的影响,旨在探讨氯吡格雷的抗炎作用。
1资料与方法
1.1纳入与排除标准纳入标准:(1)明确诊断为急性心肌梗死,且伴有不同程度心力衰竭(Killip分级Ⅰ~Ⅳ级);(2)无氯吡格雷过敏史;(3)患者及其家属知情同意,并签署知情同意书;(4)符合医学伦理学要求。排除标准:(1)妊娠期、哺乳期妇女;(2)合并严重肝、肾功能障碍者;(3)合并急慢性炎性疾病、扩张型心肌病、肥厚型心肌病、恶性肿瘤及自身免疫性疾病者。
1.2一般资料选取2012年5月—2015年5月邯郸市第一医院收治的急性心肌梗死并心力衰竭患者63例,按照随机数字表法分为观察组32例和对照组31例,两组患者性别、年龄、合并疾病、梗死部位及Killip分级比较,差异均无统计学意义(P>0.05,见表1),具有可比性。
1.3治疗方法对照组患者给予常规治疗,包括阿司匹林、硝酸甘油及利尿剂等;观察组患者在对照组治疗基础上给予氯吡格雷(赛诺菲安万特制药有限公司生产,生产批号:0080090)治疗,第1天嚼服300 mg,第2天开始口服,75 mg/d,14 d为1个疗程。
1.4观察指标(1)比较两组患者治疗前及治疗7、14 d血清炎性因子〔肿瘤坏死因子α(TNF-α)、C反应蛋白(CRP)、白介素6(IL-6)及可溶性血管细胞黏附分子1(sVCAM-1)〕水平。清晨抽取两组患者空腹肘静脉血6 ml,以3 000 r/min的速度离心10 min,留取上清液并将其置于-80 ℃环境下保存待测,采用放射免疫法检测血清TNF-α水平,采用酶联免疫吸附试验检测血清CRP、IL-6及sVCAM-1水平,所有试剂盒由深圳晶美公司提供,严格按照试剂盒说明书进行操作。(2)观察治疗期间两组患者不良反应发生情况。常见的不良反应包括严重出血(颅内出血、眼底出血及导致血红蛋白水平下降>30 g/L的出血)、轻微出血(不引起血红蛋白水平下降的出血,包括少量牙龈出血、小量皮下瘀血等)、中性粒细胞减少及血小板减少。

2结果
2.1两组患者治疗前后血清炎性因子水平比较治疗前两组患者血清TNF-α、CRP、IL-6及sVCAM-1水平比较,差异无统计学意义(P>0.05);治疗7 d、14 d观察组患者血清TNF-α、CRP、IL-6及sVCAM-1水平均低于对照组,差异有统计学意义(P<0.05,见表2)。
2.2不良反应治疗期间共5例患者发生严重出血,其中3例为脑出血、2例为消化道大出血;7例患者发生轻微出血,均为皮肤黏膜出血。两组患者严重出血、轻微出血及中性粒细胞减少发生率比较,差异均无统计学意义(P>0.05,见表3)。
表3两组患者不良反应发生率比较〔n(%)〕
Table 3Comparison of incidence of adverse reactions between the two groups
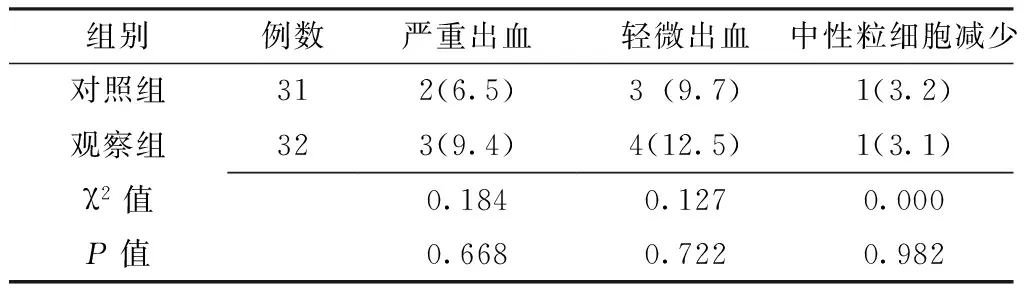
组别例数严重出血轻微出血中性粒细胞减少对照组312(6.5)3(9.7)1(3.2)观察组323(9.4)4(12.5)1(3.1)χ2值0.1840.1270.000P值0.6680.7220.982

表1 两组患者一般资料比较
注:a为t值

表2 两组患者治疗前后血清炎性因子水平比较±s)
注:TNF-α=肿瘤坏死因子α,CRP=C反应蛋白,IL-6=白介素6,sVCAM-1=可溶性血管细胞黏附分子1
3讨论
急性心肌梗死是临床常见的危重疾病,心力衰竭作为冠心病发展的终末阶段,是急性心肌梗死的常见并发症[3]。急性心肌梗死并心力衰竭的主要发病机制为心室重塑,而炎性反应在心室重塑过程中发挥着重要作用[4]。急性心肌梗死发生后坏死的心肌细胞内容物被释放,诱发炎性反应及局部炎性细胞浸润,并分泌大量炎性因子,炎性因子可通过心肌细胞的坏死或凋亡而导致心肌纤维化,继而参与心力衰竭的发生发展过程[5-6]。因此,寻找一种有效的治疗措施控制炎性反应可减缓急性心肌梗死并心力衰竭患者的心室重构,进而缓解患者病情。
氯吡格雷作为ADP受体阻滞剂,可通过与血小板膜表面的ADP受体结合而阻止纤维蛋白原与糖蛋白GPⅡb/Ⅲa受体结合,从而抑制血小板聚集[7-8]。但氯吡格雷是否同时具有抑制炎性反应及炎性因子释放的作用,目前相关研究报道较少。本研究在常规治疗的基础上联合氯吡格雷治疗急性心肌梗死并心力衰竭,旨在探讨氯吡格雷对患者血清炎性因子水平的影响及其抗炎作用。
临床研究显示,CRP是预测心血管事件最有力的炎性标志物,其可启动血凝过程、刺激组织因子生成,还可以激活补体产生免疫反应,促进动脉粥样硬化的发生发展。有研究发现,心肌梗死患者CRP水平明显升高,提示CRP可能是急性心肌梗死的重要敏感指标[9]。CRP可刺激单核细胞释放炎性递质如IL-6、TNF-α,TNF-α,还能促进T细胞产生各种炎性因子,进而促进炎性反应的发生[10]。IL-6是由活化的巨噬细胞分泌的细胞因子,可导致平滑肌细胞增殖及诱导其他炎性因子释放,研究证实其与TNF-α相互诱导而共同发挥促炎性作用[11]。sVCAM-1可通过介导血管内皮细胞与单核细胞黏附而在炎性反应的发生及发展过程中发挥作用[12]。故本研究以TNF-α、CRP、IL-6及sVCAM-1作为观察指标,结果显示,治疗7 d、14 d观察组患者血清TNF-α、CRP、IL-6及sVCAM-1水平均低于对照组,提示氯吡格雷可能通过抑制血清炎性因子水平而抑制炎性反应的发生;加上氯吡格雷具有强大的抗血小板聚集作用,因此可作为临床治疗急性心肌梗死并心力衰竭的首选药物。本研究进一步观察药物不良反应发现,两组患者严重出血、轻微出血及中性粒细胞减少发生率间无差异。
综上所述,氯吡格雷可能通过降低急性心肌梗死并心力衰竭患者血清炎性因子水平而发挥抗炎作用,且安全性较高。但本研究样本量小、随访时间短,可能影响研究结果,需要大样本量、随访时间长的研究进一步证实。
参考文献
[1]Pawlak A,Przybylski M,Frontczak-Baniewicz M,et al.Enterovirus Causing Progression of Heart Failure in a Patient with a History of Myocardial Infarction[J].Hellenic J Cardiol,2015,56(4):332-337.
[2]Brener SJ,Oldroyd KG,Maehara A,et al.Outcomes in patients with ST-segment elevation acute myocardial infarction treated withclopidogrel versus prasugrel (from the INFUSE-AMI trial)[J].Am J Cardiol,2014,113(9):1457-1460.
[3]Seneviratna A,Lim GH,Devi A,et al.Circadian Dependence of Infarct Size and Acute Heart Failure in ST Elevation Myocardial Infarction[J].PLoS One,2015,10(6):e0128526.
[4]张晓华,潘俊霞,秦利强,等.心脉隆注射液对急性心肌梗死后心力衰竭患者炎症因子的影响[J].中西医结合心脑血管病杂志,2013,11(6):667-668.
[5]Cinq-Mars A,Veilleux SP,Voisine P,et al.The novel use of heart transplantation for the management of a case with multiple complications after acute myocardial infarction[J].Can J Cardiol,2015,31(6):816-818.
[6]Waks JW,Sabatine MS,Cannon CP,et al.Clinical implications and correlates of Q waves in patients with ST-elevation myocardial infarctiontreated with fibrinolysis: observations from the CLARITY-TIMI 28 trial[J].Clin Cardiol,2014,37(3):160-166.
[7]Guimaraes PO, Tricoci P.Ticagrelor, prasugrel, or clopidogrel in ST-segment elevation myocardial infarction: which one tochoose[J].Expert Opin Pharmacother,2015,16(13):1983-1995.
[8]Varenhorst C,Koul S,Erlinge D,et al.Relationship between clopidogrel-induced platelet P2Y12 inhibition and stent thrombosis ormyocardial infarction after percutaneous coronary intervention——a case-control study[J].Am Heart J,2011,162(2):363-371.
[9]Wang J,Tang B,Liu X,et al.Increased monomeric CRP levels in acute myocardial infarction: a possible new and specific biomarker for diagnosis and severity assessment of disease[J].Atherosclerosis,2015,239(2):343-349.
[10]Yong H,Wang X,Mi L,et al.Effects of atorvastatin loading prior to primary percutaneous coronary intervention on endothelial function and inflammatory factors in patients with ST-segment elevation myocardial infarction[J].Exp Ther Med,2014,7(2):316-322.
[11]Groot HE,Hartman MH,Gu YL,et al.Soluble interleukin 6 receptor levels are associated with reduced myocardial reperfusion after percutaneous coronary intervention for acute myocardial infarction[J].Cytokine,2015,73(2):207-212.
[12]Lisowska A,Siergiejko E,Tycińska A,et al.sVCAM-1 concentration and carotid IMT values in patients with acute myocardial infarction——Atherosclerotic markers of the presence, progress and prognosis[J].Adv Med Sci,2015,60(1):101-106.
(本文编辑:谢武英)
Influence of Clopidogrel on Serum Inflammatory Cytokines Levels of Acute Myocardial Infarction Patients Complicated With Heart Failure
YANQiao-huan.
TheFirstDepartmentofGeriatrics,theFirstHospitalofHandan,Handan056002,China
【Abstract】ObjectiveTo investigate the influence of clopidogrel on serum inflammatory cytokines levels of acute myocardial infarction patients complicated with heart failure.MethodsA total of 63 acute myocardial infarction patients complicated with heart failure were selected in the First Hospital of Handan from May 2012 to May 2015,and they were divided into control group(n=31)and observation group(n=32)according to random number table.Patients of control group received conventional treatment,while patients of observation group received extra clopidogrel for 14 days based on conventional treatment.Serum levels of TNF-α,CRP,IL-6 and sVCAM-1 were compared between the two groups before treatment,after 7 days and 14 days of treatment,and incidence of adverse reactions during treatment was observed.ResultsNo statistically significant differences of serum level of TNF-α,CRP,IL-6 or sVCAM-1 was found between the two groups before treatment(P>0.05);after 7 days and 14 days of treatment,serum levels of TNF-α,CRP,IL-6 and sVCAM-1 of observation group were statistically significantly lower than those of control group(P<0.05).No statistically significant differences of incidence of severe hemorrhage,slight hemorrhage or neutropenia was found between the two groups during the treatment(P>0.05).ConclusionClopidogrel can effectively reduce the serum inflammatory cytokines levels of acute myocardial infarction patients complicated with heart failure,can effectively relive the inflammatory reaction,and is safe.
【Key words】Myocardial infarction;Heart failure;Clopidogrel;Inflammatory factor
【中图分类号】R 542.22R 541.6
【文献标识码】B
doi:10.3969/j.issn.1008-5971.2016.05.029
(收稿日期:2016-02-16;修回日期:2016-05-17)
猜你喜欢
中国实用医药(2016年27期)2016-11-30
云南中医中药杂志(2016年9期)2016-11-29
中国现代医生(2016年23期)2016-11-15
中国实用医药(2016年24期)2016-10-17
中国实用医药(2016年24期)2016-10-17
中国实用医药(2016年24期)2016-10-17
上海医药(2016年17期)2016-10-12
中国实用医药(2016年11期)2016-05-04
上海医药(2016年5期)2016-04-14
