5-羟色胺与结肠动力关系研究
2014-10-17 00:52:18俞媛洁陈继红罗和生JanHuizinga
胃肠病学和肝病学杂志 2014年1期
俞媛洁,陈继红,罗和生,Jan D Huizinga
1.武汉大学人民医院消化内科,湖北 武汉 430060;2.麦克马斯特大学健康科学学院医学系,加拿大 哈密尔顿
5-羟色胺(5-hydroxytryptamine,5-HT),也称血清素(serotonin),是胃肠道重要的信号分子,参与肠道运动和感知的调节[1]。临床上5-HT类制剂广泛用于治疗结肠动力相关性疾病,并获得较好的疗效,但具体作用机理不甚清楚。本文围绕5-HT与结肠动力的关系作一综述。
1 5-HT的来源与分布
膳食中的色氨酸经色氨酸羟化酶(tryptophan hydroxylase,TpH)转化为5-羟基-L-色氨酸(5-HTP),经L-氨基酸脱羧酶转化为5-HT。TpH1主要在肠上皮隐窝肠嗜铬细胞(enterochromaffin cells,ECs)表达,是5-HT生物合成的限速酶,而TpH2仅在神经组织表达,是另一种基因产物[2]。
大脑合成极少数5-HT[3]。人体大约95%的5-HT储存于肠道[3]。肠道5-HT分别在内分泌细胞肠嗜铬细胞以及肌间神经丛血清素能神经元内经TpH催化合成,称为黏膜源性5-HT和神经源性5-HT。
1.1 肠黏膜嗜铬细胞源性5-HT 人十二指肠和直肠含有大量的ECs,且直肠ECs含量最高[1]。90%以上的5-HT储存于ECs基底分泌颗粒[4]。ECs是一种传感器,对肠腔内压力和化学刺激非常敏感,肠腔内压力升高即可引起5-HT释放。研究发现,迷走神经刺激[5-6]、腔内酸化[7]和进食[8]等刺激均可诱发 ECs释放5-HT。
ECs基底外侧缘释放的5-HT进入血循环与胃肠道[3]。血小板缺乏TpH,无法合成5-HT,它能摄取血液循环中95%的5-HT,是血清5-HT的唯一来源。释放入肠道的5-HT作用于黏膜下传入神经神经元上的5-HT受体,激发蠕动反射,并调节肠道分泌。
结肠对扩张刺激表现出的明显收缩反应与ECs释放5-HT有关,且不被河豚毒(tetrodotoxin,TTX)阻断[9]。研究表明,黏膜刺激引起ECs释放5-HT,作用于传入神经元的5-HT4受体,诱导蠕动反射,促进结肠推进性运动[10]。ECs激活内在初级传入神经元(intrinsci primary afferent neurons,IPANs)和外在初级传入神经元(extrinsic primary afferent neurons,EPANs),黏膜下IPANs分泌Ach和降钙素,作用于5-HT1PR,启动蠕动与分泌反射[11]。
有研究发现,TpH1敲除小鼠ECs无法合成5-HT,但肠道动力仍正常[12-13],且 Keating 等[14]去除结肠黏膜后,结肠移行性运动复合波(colonic migrating motor complexes,CMMCs)仍存在,提示结肠运动并不依赖ECs源性5-HT,ECs源性5-HT仅起调节作用。此外,Heredia等[15-16]发现去除结肠黏膜后,自发性CMMCs消失,但仍存在诱导的CMMCs。ECs源性5-HT与结肠动力的关系仍需深入研究。
1.2 神经源性5-HT 5-HT是一种肌间神经丛神经递质[17]。虽然仅有2%的神经元为5-HT能神经元,但其重要性毋庸置疑,它与50%的肌间神经丛其他神经元形成突触,促进胆碱能运动神经元、氮能神经元释放乙酰胆碱(Ach)[18-19]和 NO[19-20],分别引起平滑肌收缩与舒张。
研究发现,TpH2敲除小鼠神经源性5-HT合成受阻,血清素能神经传递缺失,引起肠道传输时间延长、小肠推进性运动与结肠动力减弱[12]。因为神经源性5-HT不仅是一种神经递质,也是肠神经系统(enteric nervous system,ENS)发育的重要生长因子,敲除TpH2后肌间肠神经系统发育不完整。有研究支持,5-HT能中间神经元[3]可能直接或间接影响运动神经元、Cajal间质细胞(interstitial cells of Cajal,ICCs)[21]和平滑肌[22],显示神经源性5-HT可能在调控结肠运动中起主要作用。
2 5-HT受体
5-HT 存在多种受体(5-HT receptor,5-HTR),目前发现其至少有7种亚型(5-HT1~5-HT7),并在肠上皮细胞、内在神经元、外在神经元、间质细胞以及肠平滑肌细胞表达(见表1)。IPANs表达5-HT3、5-HT1A、5-HT4和5-HT7受体[23],其他肌间神经丛神经元表达5-HT3和5-HT4受体。5-HT3和5-HT4主要分布于肠道,与胃肠运动功能最为密切[3]。5-HT3受体在IPANs黏膜末端表达,介导快兴奋性突触电位[24-25]。黏膜施以5-HT可通过5-HT3受体激活局部反射通路,增强肠道蠕动[26-27]。5-HT能增加黏膜下IPANs释放ACh与降钙素基因相关肽,诱发肠道推进性蠕动[28]。5-HT受体间关系和协调作用未见报道。
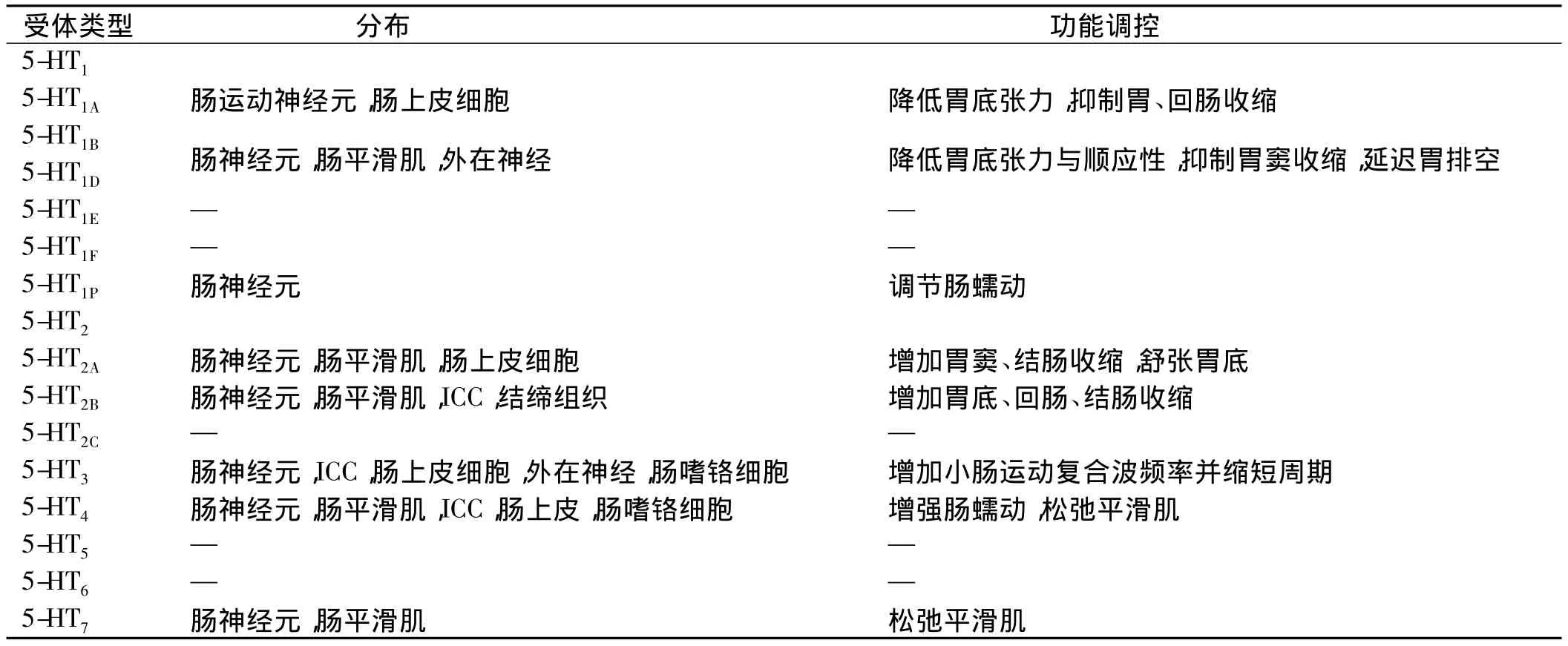
表1 消化道5-HT受体分布及其动力调控Tab1 The distribution and regulation of 5-HT receptor in the gastrointestinal tract
3 5-HT3受体拮抗剂与结肠动力
5-HT3受体能够介导血清素能中间神经元突触间的快兴奋性神经传导,以及肌间IPANs黏膜刺激的传导。
5-HT3受体拮抗剂延迟结肠以及全肠道传输时间[29],抑制肠动力。能增加肠水分吸收与大便黏稠度[30],抑制餐后肠蠕动[31-32]。可引起便秘,适用于腹泻型肠易激综合征(irritable bowel syndrome,IBS)。
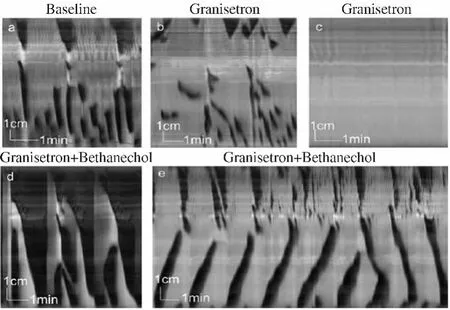
图1 格拉司琼抑制大鼠全结肠推进性运动[39]Fig1 Granisetron inhibited rats colonic motility
选择性5-HT3受体拮抗剂阿洛司琼(alosetron)最初报道仅对女性腹泻型IBS有效[33],后证明对男性效果类似[1]。可诱发缺血性结肠炎,发生率为0.15%[34],较正常人(0)高。还引发便秘,发生率为29%,严重便秘可引起肠梗阻、肠道破裂,甚至死亡。该现象与我们近期大鼠全结肠实验的发现相吻合,大鼠远端结肠施以格拉司琼(granisetron)后推进性运动受抑,长距离收缩(long distance contractions,LDCs)减少,非推进性运动(分节运动等)增加,但再给予氯贝胆碱(bethanechol)可引发强有力的节律性逆向收缩(见图1)[35]。2000年11月,在阿洛司琼问市9个月后,因消化道副反应严重危及生命,美国食品与药物管理局(Food and Drug Administration,FDA)宣布撤市。2002年7月FDA再次批准上市,用于治疗女性腹泻为主的严重IBS。此外,有研究报道,西兰司琼(cilansetron)也可引起缺血性结肠炎[36-37]。
4 5-HT4受体激动剂与结肠动力
肠神经元和平滑肌细胞表达5-HT4受体。肠神经系统胆碱能神经末梢5-HT4受体激活,中间神经元与运动神经元释放Ach,推进性运动增强[38]。研究发现[39],黏膜5-HT4受体激活能促进结肠推进性运动。5-HT4激动剂能与多种受体结合,受体亲和力(见表2)。
非选择性5-HT4受体激动剂,如替加色罗(tegaserod)与西沙必利(cisapride),能抑制5-HT再摄取转运体(serotonin reuptake transporter,SERT)活性,增强结肠蠕动,加快近端结肠排空与传输,增加排便频率,有效改善便秘症状,缓解腹部疼痛不适,用于治疗便秘型IBS与慢性便秘[40]。研究发现,替加色罗增加女性肠蠕动总数[41-43]。但替加色罗可诱发心血管不良事件(心肌缺血),机制不清[1],可能与5-HT1受体亚型有关,西沙必利能导致QT间期延长,可能与hERG编码的钾通道有关[44]。
新型选择性5-HT4受体激动剂,如普鲁卡必利(prucalopride)、维司曲格(velusetrag)、奈莫必利(nemonapride)能加快结肠传输[45],加速升结肠排空[46],增加排便频率与自发肠蠕动[47],并降低大便黏稠度[48],对慢传输型便秘(slow transit constipation,STC)效果显著。有报道,老年患者应用4周普鲁卡必利(2 mg,1次/d)后便秘症状有所改善[49]。新型 5-HT4受体激动剂副作用主要表现为轻型腹泻,降低剂量或停药后症状消失[3]。
新型非选择性5-HT4受体激动剂,如伦扎必利(renzapride)与普鲁卡必利作用类似,能兴奋肠肌间神经元5-HT4受体,释放Ach,刺激平滑肌收缩,且呈剂量依赖,常用于治疗便秘型IBS与交替型IBS。莫沙必利(mosapride)代谢产物为5-HT3受体拮抗剂,对结肠动力作用弱[50]。
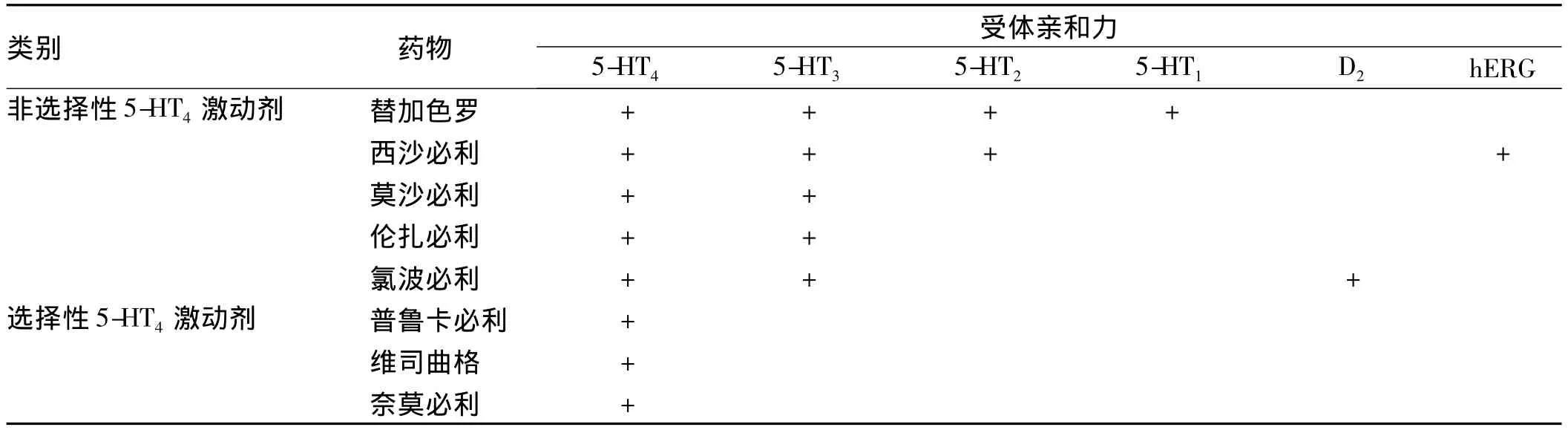
表2 5-HT4激动剂的受体亲和力Tab2 The receptor affinity of 5-HT4agonist
5 5-HT再摄取转运体(SERT)
5-HT再摄取转运体(serotonin reuptake transporter,SERT,5-HTT)摄取并灭活5-HT。血清素能神经元质膜能表达特异性SERT,介导5-HT再摄取[51],肠黏膜此类神经元缺乏,但小鼠、大鼠、豚鼠以及人黏膜上皮细胞均表达 SERT[52-53]。小肠 SERT 表达最多[54]。炎症性肠病(inflammation bowel disease,IBD)与IBS的结肠 SERT 表达减少[53]。
体外抑制肠内SERT,起初能增强肠蠕动,但随着5-HT受体敏感性降低,蠕动反射将终止,局部刺激黏膜后,黏膜下IPANs增加,提示小肠黏膜上皮SERT参与ECs源性5-HT灭活。
当SERT被抑制或敲除时,有机阳离子转运体和多巴胺转运蛋白可部分代偿SERT功能,但不足以维持正常的功能。SERT敲除小鼠结肠动力增强,粪便含水量增加,表现为腹泻,或腹泻便秘交替[52],与IBS患者症状相似。选择性5-HT再摄取抑制剂(selective serotonin reuptake inhibitors,SSRIs)和三环类抗抑郁药可调节SERT功能,理论上可缓解IBS症状。
6 5-HT与结肠动力障碍
5-HT参与肠道运动功能调控。血清素能神经元受损时肠道收缩活动紊乱,肠道运动障碍患者5-HT功能明显受损。
5-HT代谢异常可能与IBS发病有关。腹泻型IBS与感染后IBS循环5-HT增加,便秘型IBS循环5-HT减少[55]。腹泻型IBS结肠黏膜5-HT浓度升高,便秘型则降低[56]。感染后IBS患者ECs数量和5-HT阳性的肠神经纤维增加[57]。5-HT3与5-HT4受体拮抗剂能延迟腹泻型IBS结肠传输,提示D-IBS患者5-HT增加[58]。便秘型IBS患者ECs数量大幅度下降,5-HT与ECs数目比增加,提示便秘型IBS患者5-HT释放异常。
慢性便秘患者5-HT信号异常[28]。慢传输型便秘患者结肠肌层神经元5-HT增加,但平滑肌5-HT受体减少,5-HT3依赖的胃结肠反射受损。Dinning等[59-60]在慢性便秘患者结肠测压中观测到推进性收缩减少,逆向运动增加导致结肠传输减慢、排便困难。慢性便秘中5-HT受体可用性、密度以及功能是否降低尚不确定[61]。
总之,5-HT参与结肠运动调节,但具体调节机制复杂,受体在各段结肠分布不同,受体间相互作用不清,5-HT作用于平滑肌具体方式不明,难以直接从临床效果上判断各5-HT制剂对结肠运动的影响。若按结肠部位独立研究,有望阐明结肠5-HT的生理机制,以及各5-HT制剂的特定效应,为临床提供理论依据。
[1]Hasler WL.Serotonin and the GI tract[J].Curr Gastroenterol Rep,2009,11(5):383-391.
[2]Côté F,Thévenot E,Fligny C,et al.Disruption of the nonneuronal tph1 gene demonstrates the importance of peripheral serotonin in cardiac function[J].Proc Natl Acad Sci U S A,2003,100(23):13525-13530.
[3]Gershon MD,Tack J.The serotonin signaling system:from basic understanding to drug development for functional GI disorders[J].Gastroenterology,2007,132(1):397-414.
[4]Racké K,Reimann A,Schwörer H,et al.Regulation of 5-HT release from enterochromaffin cells[J].Behav Brain Res,1996,73(1-2):83-87.
[5]Ahlman H,Demagistris L,Zinner M,et al.Release of immunoreactive serotonin into the lumen of the feline gut in response to vagal nerve stimulation[J].Science,1981,213(4513):1254-1255.
[6]Gronstad K,Dahlstrom A,Florence L,et al.Regulatory mechanisms in endoluminal release of serotonin and substance P from feline jejunum[J].Dig Dis Sci,1987,32(4):393-400.
[7]Kellum J,Mccabe M,Schneier J,et al.Neural control of acid-induced serotonin release from rabbit duodenum [J].Am J Physiol,1983,245(6):G824-G831.
[8]Ferrara A,Zinner MJ,Jaffe BM.Intraluminal release of serotonin,substance P,and gastrin in the canine small intestine[J].Dig Dis Sci,1987,32(3):289-294.
[9]Fujimiya M,Okumiya K,Kuwahara A.Immunoelectron microscopic study of the luminal release of serotonin from rat enterochromaffin cells induced by high intraluminal pressure [J].Histochem Cell Biol,1997,108(2):105-113.
[10]Grider JR.Desensitization of the peristaltic reflex induced by mucosal stimulation with the selective 5-HT4 agonist tegaserod[J].Am J Physiol Gastrointest Liver Physiol,2006,290(2):G319-G327.
[11]Gershon MD.Nerves,reflexes,and the enteric nervous system:pathogenesis of the irritable bowel syndrome [J].J Clin Gastroenterol,2005,39(5 Suppl 3):S184-S193.
[12]Gershon MD.5-Hydroxytryptamine(serotonin)in the gastrointestinal tract[J].Curr Opin Endocrinol Diabetes Obes,2013,20(1):14-21.
[13]Li Z,Chalazonitis A,Huang YY,et al.Essential roles of enteric neuronal serotonin in gastrointestinal motility and the development/survival of enteric dopaminergic neurons[J].J Neurosci,2011,31(24):8998-9009.
[14]Keating DJ,Spencer NJ.Release of 5-hydroxytryptamine from the mucosa is not required for the generation or propagation of colonic migrating motor complexes[J].Gastroenterology,2010,138(2):659-670.
[15]Heredia DJ,Dickson EJ,Bayguinov PO,et al.Localized release of serotonin(5-hydroxytryptamine)by a fecal pellet regulates migrating motor complexes in murine colon [J].Gastroenterology,2009,136(4):1328-1338.
[16]Zagorodnyuk VP,Spencer NJ.Localization of the sensory neurons and mechanoreceptors required for stretch-evoked colonic migrating motor complexes in mouse colon[J].Front Physiol,2011,2:98.
[17]Wade PR,Tamir H,Kirchgessner AL,et al.Analysis of the role of 5-HT in the enteric nervous system using anti-idiotopic antibodies to 5-HT receptors[J].Am J Physiol,1994,266(3 Pt 1):G403-G416.
[18]Neal KB,Bornstein JC.Mapping 5-HT inputs to enteric neurons of the guinea-pig small intestine[J].Neuroscience,2007,145(2):556-567.
[19]Briejer MR,Akkermans LM,Schuurkes JA.Interactions of serotonin with multiple receptors and neurotransmitters in the guinea-pig isolated colon[J].Arch Int Pharmacodyn Ther,1995,329(1):121-133.
[20]Toda N,Herman AG.Gastrointestinal function regulation by nitrergic efferent nerves[J].Pharmacol Rev,2005,57(3):315-338.
[21]Liu HN,Ohya S,Nishizawa Y,et al.Serotonin augments gut pacemaker activity via 5-HT3 receptors[J].PLoS One,2011,6(9):e24928.
[22]Wouters MM,Farrugia G,Schemann M.5-HT receptors on interstitial cells of Cajal,smooth muscle and enteric nerves[J].Neurogastroenterol Motil,2007,19 Suppl 2:5-12.
[23]Neal KB,Bornstein JC.Serotonergic receptors in therapeutic approaches to gastrointestinal disorders[J].Curr Opin Pharmacol,2006,6(6):547-552.
[24]Monro RL,Bertrand PP,Bornstein JC.ATP and 5-HT are the principal neurotransmitters in the descending excitatory reflex pathway of the guinea-pig ileum[J].Neurogastroenterol Motil,2002,14(3):255-264.
[25]Zhou X,Galligan JJ.Synaptic activation and properties of 5-hydroxytryptamine(3)receptors in myenteric neurons of guinea pig intestine[J].J Pharmacol Exp Ther,1999,290(2):803-810.
[26]Gwynne RM,Bornstein JC.Local inhibitory reflexes excited by mucosal application of nutrient amino acids in guinea pig jejunum[J].Am J Physiol Gastrointest Liver Physiol,2007,292(6):G1660-G1670.
[27]Tuladhar BR,Kaisar M,Naylor RJ.Evidence for a 5-HT3 receptor involvement in the facilitation of peristalsis on mucosal application of 5-HT in the guinea pig isolated ileum[J].Br J Pharmacol,1997,122(6):1174-1178.
[28]Pan H,Gershon MD.Activation of intrinsic afferent pathways in submucosal ganglia of the guinea pig small intestine [J].J Neurosci,2000,20(9):3295-3309.
[29]Clemens CH,Samsom M,Van Berge HG,et al.Effect of alosetron on left colonic motility in non-constipated patients with irritable bowel syndrome and healthy volunteers [J].Aliment Pharmacol Ther,2002,16(5):993-1002.
[30]Andresen V, MontoriVM, KellerJ, etal. Effectsof 5-hydroxytryptamine(serotonin)type 3 antagonists on symptom relief and constipation in nonconstipated irritable bowel syndrome:a systematic review and meta-analysis of randomized controlled trials[J].Clin Gastroenterol Hepatol,2008,6(5):545-555.
[31]Talley NJ,Phillips SF,Haddad A,et al.GR 38032F(ondansetron),a selective 5HT3 receptor antagonist,slows colonic transit in healthy man [J].Dig Dis Sci,1990,35(4):477-480.
[32]von der Ohe MR,Hanson RB,Camilleri M.Serotonergic mediation of postprandial colonic tonic and phasic responses in humans[J].Gut,1994,35(4):536-541.
[33]Cremonini F,Delgado-Aros S,Camilleri M.Efficacy of alosetron in irritable bowel syndrome:a meta-analysis of randomized controlled trials[J].Neurogastroenterol Motil,2003,15(1):79-86.
[34]Chang L,Chey WD,Harris L,et al.Incidence of ischemic colitis and serious complications of constipation among patients using alosetron:systematic review of clinical trials and post-marketing surveillance data[J].Am J Gastroenterol,2006,101(5):1069-1079.
[35]Chen JH,Zhang Q,Yu Y,et al.Neurogenic and myogenic properties of pan-colonic motor patterns and their spatiotemporal organization in rats[J].PLoS One,2013,8(4):e60474
[36]Camilleri M.Treating irritable bowel syndrome:overview,perspective and future therapies [J].Br J Pharmacol,2004,141(8):1237-1248.
[37]Olden KW,Crowell MD.Cilansetron[J].Drugs Today(Barc),2005,41(10):661-666.
[38]Langlois M,Fischmeister R.5-HT4 receptor ligands:applications and new prospects[J].J Med Chem,2003,46(3):319-344.
[39]Hoffman JM,Tyler K,Maceachern SJ,et al.Activation of colonic mucosal 5-HT(4)receptors accelerates propulsive motility and inhibits visceral hypersensitivity[J].Gastroenterology,2012,142(4):844-854.
[40]De Maeyer JH,Lefebvre RA,Schuurkes JA.5-HT4 receptor agonists:similar but not the same[J].Neurogastroenterol Motil,2008,20(2):99-112.
[41]Camilleri M.Review article:tegaserod[J].Aliment Pharmacol T-her,2001,15(3):277-289.
[42]Evans BW,Clark WK,Moore DJ,et al.Tegaserod for the treatment of irritable bowel syndrome and chronic constipation[J].Cochrane Database Syst Rev,2007(4):CD003960.
[43]Müller-Lissner SA,Fumagalli I,Bardhan KD,et al.Tegaserod,a 5-HT(4)receptor partial agonist,relieves symptoms in irritable bowel syndrome patients with abdominal pain,bloating and constipation[J].Aliment Pharmacol Ther,2001,15(10):1655-1666.
[44]Tack J,Camilleri M,Chang L,et al.Systematic review:cardiovascular safety profile of 5-HT(4)agonists developed for gastrointestinal disorders[J].Aliment Pharmacol Ther,2012,35(7):745-767.
[45]Emmanuel AV,Roy AJ,Nicholls TJ,et al.Prucalopride,a systemicenterokinetic,for the treatment of constipation[J].Aliment Pharmacol Ther,2002,16(7):1347-1356.
[46]De Schryver AM,Andriesse GI,Samsom M,et al.The effects of the specific 5HT(4)receptor agonist,prucalopride,on colonic motility in healthy volunteers[J].Aliment Pharmacol Ther,2002,16(3):603-612.
[47]Sloots CE,Poen AC,Kerstens R,et al.Effects of prucalopride on colonic transit,anorectal function and bowel habits in patients with chronic constipation[J].Aliment Pharmacol Ther,2002,16(4):759-767.
[48]Camilleri M,Kerstens R,Rykx A,et al.A placebo-controlled trial of prucalopride for severe chronic constipation[J].N Engl J Med,2008,358(22):2344-2354.
[49]Sanger GJ.Translating 5-HT receptor pharmacology[J].Neurogastroenterol Motil,2009,21(12):1235-1238.
[50]Carlsson L,Amos GJ,Andersson B,et al.Electrophysiological characterization of the prokinetic agents cisapride and mosapride in vivo and in vitro:implications for proarrhythmic potential?[J].J Pharmacol Exp Ther,1997,282(1):220-227.
[51]Blakely RD,Berson HE,Fremeau RJ,et al.Cloning and expression of a functional serotonin transporter from rat brain [J].Nature,1991,354(6348):66-70.
[52]Chen JJ,Li Z,Pan H,et al.Maintenance of serotonin in the intestinal mucosa and ganglia of mice that lack the high-affinity serotonin transporter:Abnormal intestinal motility and the expression of cation transporters[J].J Neurosci,2001,21(16):6348-6361.
[53]Coates M D,Mahoney CR,Linden DR,et al.Molecular defects in mucosal serotonin content and decreased serotonin reuptake transporter in ulcerative colitis and irritable bowel syndrome[J].Gastroenterology,2004,126(7):1657-1664.
[54]van Lelyveld N,Ter Linde J,Schipper ME,et al.Regional differences in expression of TPH-1,SERT,5-HT(3)and 5-HT(4)receptors in the human stomach and duodenum [J].Neurogastroenterol Motil,2007,19(5):342-348.
[55]Dunlop SP,Coleman NS,Blackshaw E,et al.Abnormalities of 5-hydroxytryptamine metabolism in irritable bowel syndrome[J].Clin Gastroenterol Hepatol,2005,3(4):349-357.
[56]Spiller R.Serotonin and GI clinical disorders[J].Neuropharmacology,2008,55(6):1072-1080.
[57]Dunlop SP,Jenkins D,Neal KR,et al.Relative importance of enterochromaffin cell hyperplasia,anxiety,and depression in postinfectious IBS[J].Gastroenterology,2003,125(6):1651-1659.
[58]De Ponti F,Tonini M.Irritable bowel syndrome:new agents targeting serotonin receptor subtypes[J].Drugs,2001,61(3):317-332.
[59]Dinning PG,Smith TK,Scott SM.Pathophysiology of colonic causes of chronic constipation[J].Neurogastroenterol Motil,2009,21 Suppl 2:20-30.
[60]Dinning PG,Zarate N,Hunt LM,et al.Pancolonic spatiotemporal mapping reveals regional deficiencies in,and disorganization of colonic propagating pressure waves in severe constipation[J].Neurogastroenterol Motil,2010,22(12):e340-e349.
[61]Costedio MM,Hyman N,Mawe GM.Serotonin and its role in colonic function and in gastrointestinal disorders[J].Dis Colon Rectum,2007,50(3):376-388.
猜你喜欢
天津医科大学学报(2021年4期)2021-08-21 02:14:52
中国民间疗法(2020年22期)2021-01-07 07:39:34
中国中医急症(2019年10期)2019-05-21 07:20:46
中成药(2018年10期)2018-10-26 03:41:22
天然产物研究与开发(2018年6期)2018-07-09 06:01:46
川北医学院学报(2015年5期)2015-12-05 08:22:43
中国医疗美容(2015年1期)2015-07-12 10:06:55
医学研究杂志(2015年5期)2015-06-10 06:43:26
中国卫生标准管理(2015年3期)2015-01-27 00:57:55
西南军医(2015年2期)2015-01-22 09:09:46