
神经根沉降征在腰椎滑脱症和腰椎间盘突出症中的差异
2014-07-05 16:39:07孙晓雷邓树才马信龙
天津医药 2014年12期
田 鹏 付 鑫 孙晓雷 邓树才 马信龙,2△
神经根沉降征在腰椎滑脱症和腰椎间盘突出症中的差异
田 鹏1付 鑫1孙晓雷1邓树才1马信龙1,2△
目的 评价神经根沉降征在腰椎滑脱症(LS)和腰椎间盘突出症(LDH)患者中的表现,并比较其在二者中的差异。方法收集天津市天津医院脊柱外科2012年7月—2014年3月行手术治疗的腰椎退行脊柱病患者资料151例,分为LS组48例和LDH组103例。采用JOA评分评估2组患者术前临床表现,比较2组患者神经根沉降征阳性率,分析JOA评分与神经根沉降征的关系。结果LS组和LDH患者在JOA评分差异无统计学意义(15.83±3.57 vs 16.76±3.10,t=1.624,P=0.107)。LS组神经根沉降征阳性39例(81.25%),而LDH组65例(63.11%),差异有统计学意义(χ2=5.028,P=0.031)。LS组中,神经根沉降征阳性者JOA评分低于阴性者(15.33±3.50 vs 18.00± 3.20,t=2.092,P=0.042);而LDH组中,神经根沉降征阳性和阴性者JOA评分差异无统计学意义(16.40±3.13 vs 17.37±2.99,t=1.539,P=0.127)。结论神经根沉降征阳性也见于腰椎间盘突出症中,但在临床表现更严重的腰椎滑脱症患者中更易出现。
椎间盘移位;腰椎滑脱;腰椎间盘突出;神经根沉降征;JOA评分
腰椎管狭窄症是腰椎管容量减少,压迫椎管及神经根管神经而出现功能障碍的总称,是临床常见脊柱手术原因之一[1]。腰椎滑脱和椎间盘突出是造成腰椎管狭窄的常见原因。腰椎管狭窄症的诊断困难在于休息时疼痛消失,只有体力活动时才出现疼痛及功能受限。评估腰椎管狭窄症的常见MRI评价方法有硬膜囊横截面积(cross-sectional area,CSA)、形态学等级A~D和神经根沉降征。Barz等[2]早在2010年就提出神经根沉降征的概念,指仰卧位MRI中,腰神经根不随重力沉降到硬膜囊背侧,依然停留在硬膜囊腹侧和中央,并指出神经根沉降征阳性率与腰椎管狭窄症有关。最新研究指出神经根沉降征阳性最易出现在临床显著腰椎管狭窄、且需要手术干预的患者中[3]。既往研究大多是比较腰椎管狭窄症和非特异性腰痛患者,而神经根沉降征在腰椎滑脱中的研究相对较少。本研究观察单节段L4~5和L5~S1手术治疗的腰椎间盘突出症(lumbar disc herniation,LDH)患者中神经根沉降征阳性率,同时分析同期手术治疗的腰椎滑脱症(lumbar spondylolisthesis,LS)中神经根沉降征的表现情况,并比较二者差异。
1 资料与方法
1.1 一般资料 收集2012年7月—2014年3月天津市天津医院手术治疗且影像资料完整的腰椎退行脊柱病患者151例,包括LS 48例和LDH 103例。所有患者均通过病史、体检及影像学(X线片、MRI、CT)获得证实。排除标准如下:(1)周围血管性疾病,下肢静脉曲张或动脉闭塞性疾病。(2)下肢关节疾病,如髋关节和膝关节骨性关节炎或类风湿性关节炎等。(3)腰椎既往手术病史。(4)脊柱蛛网膜炎症疾病。LS组中L4前滑脱41例,L5前滑脱7例,根据Meyerding法该组患者均为Ⅰ度滑脱。LDH组中L4~5节段55例,L5~S1节段48例。
1.2 方法
1.2.1 神经根沉降征在MRI横断面上判断标准 参考Barz 等[2]方法,于MRI T2加权图像横断面上,在腰椎双侧小关节顶点间作一水平直线,除本节段离开硬膜囊的神经根外,还有其他神经根位于连线的腹侧,此即为神经根沉降征阳性,见图1A。在连线的腹侧除离开硬膜囊的神经根之外若无其他神经根,此现象定义为神经根沉降征阴性,见图1B。
1.2.2 神经根沉降征评估 观察每例患者腰椎MRI横断面扫描(包括L1~L5节段)硬膜囊上神经根的分布情况,只要有1个节段有神经根沉降征阳性,即定义为神经根沉降征阳性。由2名脊柱外科医师独立在MRI扫描上评估神经根沉降征,再进一步分析之前,针对两名研究者的最初评级不一致的神经根沉降征,经二者协商后达成一致。
1.2.3 JOA腰背痛评分 根据JOA腰痛评分系统对每例患者进行术前评价。JOA评分包括主观症状(9分)、临床体征(6分)、日常生活受限情况(14分),总计29分,根据膀胱功能情况相应减分(-6分)[4]。比较LS组和LDH组患者JOA评分的差异,并比较各组内神经根沉降征阳性和阴性患者JOA评分的差异。
1.3 统计学方法 应用SPSS 19.0软件进行数据分析。计量资料以均数±标准差(±s)表示,2组间比较采用t检验,计数资料采用例表示,组间比较采用χ2检验。P<0.05表示差异有统计学意义。
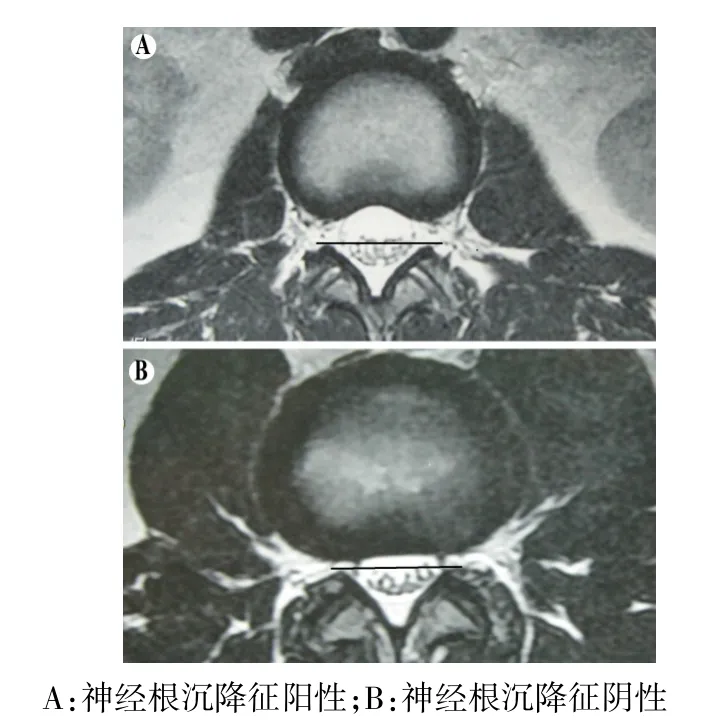
Fig.1 The performance of nerve root in transverse MRI scan图1 MRI横断面扫描神经根表现
2 结果
2.1 2组临床一般资料比较 LS组患者年龄大于LDH组,且女性患者比例较高。2组患者JOA腰痛评分差异无统计学意义,见表1。
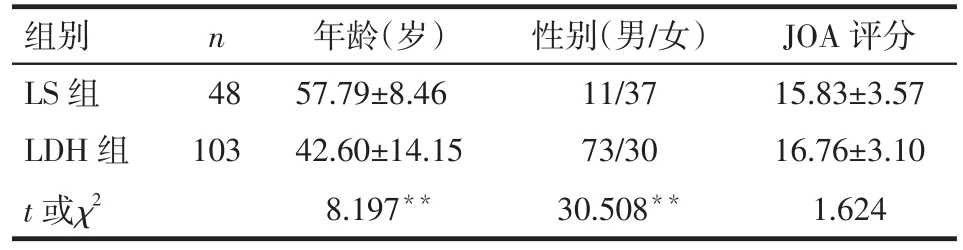
Tab.1 Comparison of JOA score,gender and age of patients between LS group and LDH group表1 LS组和LDH组患者的年龄、性别、JOA评分比较
2.2 2组患者神经根沉降征阳性率比较 在LS组中,39例神经根沉降征阳性,阳性率81.25%;LDH组中65例神经根沉降征阳性,阳性率63.11%,低于LS组(χ2=5.028,P<0.05)。神经根沉降征阳性节段位于病变节段水平以上,见图2。
2.3 2组患者中神经根沉降征阳性和阴性患者JOA评分比较 LS组中,神经根沉降征阳性患者JOA评分为15.33±3.50,阴性为18.00±3.20,差异有统计学意义(t=2.092,P=0.042)。LDH组中,神经根沉降征阳性患者JOA评分为16.40±3.13,阴性为17.37± 2.99,差异无统计学意义(t=1.539,P=0.127)。
3 讨论
3.1 腰椎管狭窄症与神经根沉降征的诊断 脊柱MRI被认为是腰椎管狭窄症诊断、描绘病变程度及位置的重要的术前评估工具。既往有研究证实无症状群体中椎管狭窄比例较高,然而寻找更有价值的临床相关影像学指标具有一定难度[5]。有研究证实患者Oswestry功能障碍指数(Oswestry disability index,ODI)与腰椎管狭窄程度和CSA间无相关性[6],以致MRI在腰椎管狭窄中诊断作用受到质疑[7]。然而,也有研究显示CSA和形态学等级A~D能够后较好地评价腰椎管狭窄症[8]。因此神经根沉降征在腰椎管狭窄症中的应用越来越多地受到关注。
3.2 神经根沉降征在腰椎管狭窄症中的应用 Barz 等[2]首次报道了症状性腰椎管狭窄症患者中神经根沉降征阳性率为94%,提出该征在诊断腰椎管狭窄症时具有较高的灵敏度。本研究中LS组神经根沉降征阳性率为81.25%,与既往研究基本一致,本研究纳入腰椎滑脱症,而Barz等[2]研究对象为中央型腰椎管狭窄患者。也有研究比较腰椎管狭窄症、腰痛、血管性跛行及无症状对照组患者中神经根沉降征阳性情况,证实其灵敏度为42%~66%,特异度为49%~78%,特别是最小CSA小于80 mm2患者灵敏度从60%提高到96%,神经根沉降征能够区分腰椎管狭窄症患者与对照组,但是该征不能区分腰椎管狭窄症和腰痛及血管性跛行[9]。本研究中,LS患者神经根沉降征阳性率高于LDH患者,造成此征阳性率差异的原因在于二者造成椎管狭窄的发病机制不同。
国外有学者发现腰椎狭窄症患者伴有神经根沉降征阳性时,其狭窄节段硬膜外压力平均值达22 mmHg(1 mmHg=0.133 kPa),其结果不受狭窄节段CSA影响,证实腰椎管狭窄症患者在狭窄节段硬膜外压力升高,从而提出腰神经根未沉到硬膜囊背侧是由于狭窄节段束缚了腰神经根[10]。本研究纳入的腰椎滑脱症为退变性,椎管狭窄缓慢进展过程中,神经根受压缺血导致损伤,神经损伤修复过程中逐渐出现炎性反应,从而引起神经根粘连。但是具体的机制需要后续继续研究。
有研究提出在MRI中硬膜囊最小CSA是定量评价椎管狭窄的一种客观指标,特别是针对<100 mm2时更有临床意义[11]。但也有研究指出ODI评分和硬膜囊最小CSA之间不存在相关性,ODI可能不是评估腰椎狭窄症患者最理想的方法[6,12]。因此本研究未进行CSA与神经根沉降征相关比较研究。本研究显示LS组中神经根沉降征阳性患者具有较低的JOA评分,说明其有较严重的临床表现。国外有研究证实在退变腰椎管狭窄症患者中女性相比于男性有更重的腰腿痛症状[13]。本研究中LS组年龄较大且女性比例高,与国外报道一致,原因可能是女性患者症状重且就医接受手术的比例高,这也需要大宗病例的临床研究来进一步验证。
本研究难免存在一定的局限性。本研究仅是观察我院手术治疗LS及LDH群体,且是回顾分析术前MRI上神经根沉降征的差异,在随访时大多患者无法再行MRI检查,不能比较术前与术后沉降征的表现差异。今后可在研究前周密设计研究计划,定期随访,力争获得完整详细的随访资料,从而获得严谨的研究结果。
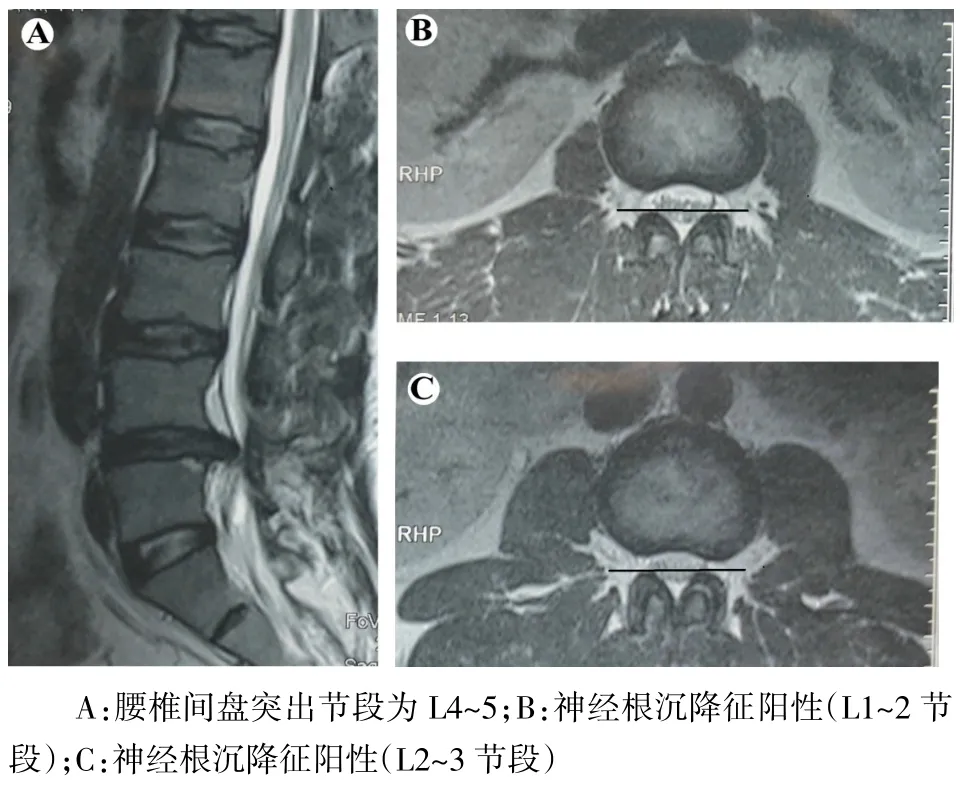
Fig.2 T2-weighted MRI scans of a LDH patient with a positive nerve root sedimentation sign图2 T2加权MRI显示腰椎间盘突出症患者神经根沉降征阳性表现
[1]Atlas SJ,Keller RB,Robson D,et al.Surgical and nonsurgical management of lumbar spinal stenosis:four-year outcomes from the maine lumbar spine study[J].Spine(Phila Pa 1976),2000,25(5): 556-562.
[2]Barz T,Melloh M,Staub LP,et al.Nerve root sedimentation sign: evaluation of a new radiological sign in lumbar spinal stenosis[J]. Spine (Phila Pa 1976),2010,35(8):892-897. doi:10.1097/ BRS.0b013e3181c7cf4b.
[3]Fazal A,Yoo A,Bendo JA.Does the presence of the nerve root sedimentation sign on MRI correlate with the operative level in patients undergoing posterior lumbar decompression for lumbar stenosis [J]?Spine J,2013,13(8):837-842. doi:10.1016/j.spinee.2013. 02.067.
[4]Taneichi H,Suda K,Kajino T,et al.Unilateral transforaminal lumbar interbody fusion and bilateral anterior-column fixation with two Brantigan I/F cages per level:clinical outcomes during a minimum 2-year follow-up period[J].J Neurosurg Spine,2006,4(3):198-205. doi:10.3171/spi.2006.4.3.198.
[5]Madsen R,Jensen TS,Pope M,et al.The effect of body position and axial load on spinal canal morphology:an MRI study of central spi-nal stenosis[J].Spine(Phila Pa 1976),2008,33(1):61-67. doi: 10.1097/BRS.0b013e31815e395f.
[6]Sirvanci M,Bhatia M,Ganiyusufoglu KA,et al.Degenerative lumbar spinal stenosis:correlation with Oswestry Disability Index and MR imaging[J].Eur Spine J,2008,17(5):679-685.doi:10.1007/ s00586-008-0646-5.
[7]Ishimoto Y,Yoshimura N,Muraki S,et al.Prevalence of symptomatic lumbar spinal stenosis and its association with physical performance in a population-based cohort in Japan:the Wakayama Spine Study[J].Osteoarthritis Cartilage,2012,20(10):1103-1108. doi: 10.1016/j.joca.2012.06.018.
[8]Lonne G,Odegard B,Johnsen LG,et al.MRI evaluation of lumbar spinal stenosis:is a rapid visual assessment as good as area measurement[J]?Eur Spine J,2014,23(6):1320-1324.doi:10.1007/ s00586-014-3248-4.
[9]Tomkins-Lane CC,Quint DJ,Gabriel S,et al.Nerve root sedimentation sign for the diagnosis of lumbar spinal stenosis:reliability,sensitivity,and specificity[J].Spine(Phila Pa 1976),2013,38(24): E1554-1560.doi:10.1097/BRS.0b013e3182a8c2da.
[10]Barz T,Melloh M,Staub LP,et al.Increased intraoperative epidural pressure in lumbar spinal stenosis patients with a positive nerve root sedimentation sign[J].Eur Spine J,2014,23(5):985-990.doi: 10.1007/s00586-013-3071-3.
[11]Kanno H,Ozawa H,Koizumi Y,et al.Dynamic change of dural sac cross-sectional area in axial loaded magnetic resonance imaging correlates with the severity of clinical symptoms in patients with lumbar spinal canal stenosis[J].Spine(Phila Pa 1976),2012,37(3): 207-213.doi:10.1097/BRS.0b013e3182134e73.
[12]Wang DM,Yang QG,Gao SS,et al.The study of relationship between the nerve root sedimentation syndrome and lumbar spinal stenosis[J].Acta Universitatis Medicinalis Anhui,2013,48(5):520-523.[汪大明,杨庆国,高胜山,等.神经根沉降症与腰椎管狭窄的相关性研究[J].安徽医科大学学报,2013,48(5):520-523.]
[13]Kim HJ,Suh BG,Lee DB,et al.Gender difference of symptom severity in lumbar spinal stenosis:role of pain sensitivity[J].Pain physician,2013,16(6):E715-723.
(2014-08-08收稿 2014-09-02修回)
(本文编辑 李鹏)
The Different Sign of Nerve Root Sedimentation on MRI in Patients between Lumbar Spondylolisthesis and Lumbar Disc Herniation
TIAN Peng1,FU Xin1,SUN Xiaolei1,DENG Shucai1,MA Xinlong1,2△
1 Tianjin Hospital,Tianjin 300211,China;2 Tianjin Medical University General Hospital
△
E-mail:maxinlong8686@sina.com
ObjectiveTo evaluate and compare the presence of the nerve root sedimentation sign in patients with lumbar spondylolisthesis(LS)and lumbar disc herniation(LDH).MethodsOne hundred and fifty-one patients with degenerative lumbar spinal disease treated by surgery from July 2012 to March 2014 were reviewed retrospectively in Tianjin Hospital.All the patients were divided into two groups:LS group(48 cases)and LDH group(103 cases).The clinical outcomes were evaluated by Japanese Orthopedic Association(JOA).The probability of positive sedimentation sign was compared between LS group and LDH group.Correlation between the JOA score and nerve root sedimentation sign were analysed in two groups.ResultsThere was no statistical difference in JOA score between LS group and LDH group(15.83±3.57 vs 16.76± 3.10,t=1.624,P=0.107).A positive sedimentation sign was identified in 39 patients in the LS group(81.25%)but in 65 patients in the LDH group(63.11%).The difference between LS group and LDH group was statistically significant(χ2=5.028, P=0.031).In LS group,JOA scores of patients with positive nerve root sedimentation sign were lower than those of patients with negative nerve root sedimentation sign(15.33±3.50 vs 18.00±3.20,t=2.092,P=0.042);but in LDH group,there was no statistical difference in JOA scores of patients between positive nerve root sedimentation sign and negative nerve root sedimentation sign(16.40±3.13 vs 17.37±2.99,t=1.539,P=0.127).ConclusionA positive sedimentation sign also occurs in patients with LDH,but positive nerve root sedimentation sign are more likely to appear in patients with lumbar spondylolisthesis who have worse clinical symptoms.
intervertebral disk displacement;lumbar spondylolisthesis;lumbar disc herniation;nerve root sedimentation sign;JOA score
R681.5
A
10.3969/j.issn.0253-9896.2014.12.018
国家自然科学基金资助项目(81401792);天津市中医药管理局中医、中西医结合科研课题(13123);天津市卫生局攻关项目(10KG111)
1天津市天津医院(邮编300211);2天津医科大学总医院
△通讯作者 E-mail:maxinlong8686@sina.com
猜你喜欢
中国港湾建设(2022年12期)2022-12-28 05:27:24
基层中医药(2021年12期)2021-06-05 06:56:34
中华养生保健(2020年5期)2020-11-16 01:44:42
中外医疗(2016年15期)2016-12-01 04:25:39
中国继续医学教育(2015年2期)2016-01-06 01:36:25
实用肝脏病杂志(2015年5期)2015-12-03 06:28:03
结核与肺部疾病杂志(2015年1期)2015-07-18 11:09:22
现代电生理学杂志(2015年1期)2015-07-18 11:02:15
中医研究(2014年11期)2014-03-11 20:29:52
筑路机械与施工机械化(2014年3期)2014-03-01 02:58:23
