
Metabolic response to 6-week aerobic exercise training and dieting in previously sedentary overweight and obese pre-menopausal women: A random ized trial
2014-03-21 03:20PetriWiklunMrkkuAlenEveliinMunukkShuMeiChengBoYuStuPekklSulinCheng
Petri Wiklun,Mrkku Alen,Eveliin Munukk,Shu Mei Cheng, Bo Yu,Stu Pekkl,Sulin Cheng,,e,*
aDepartment of Health Sciences,University of Jyva¨skyla¨,FI-40014 Jyva¨skyla¨,Finland
bDepartment of Medical Rehabilitation,Oulu University Hospital,Oulu FI-90029,Finland
cInstitute of Health Sciences,University of Oulu,Oulu FI-90014,Finland
dSchool of Kinesiology,Shanghai University of Sport,Shanghai 200438,China
eDepartmentof Sportand Physical Education,Shanghai Jiao Tong University,Shanghai200240,China
Metabolic response to 6-week aerobic exercise training and dieting in previously sedentary overweight and obese pre-menopausal women: A random ized trial
Petri Wiklunda,b,Markku Alenb,c,Eveliina Munukkaa,Shu Mei Chenga, Bo Yud,Satu Pekkalaa,Sulin Chenga,d,e,*
aDepartment of Health Sciences,University of Jyva¨skyla¨,FI-40014 Jyva¨skyla¨,Finland
bDepartment of Medical Rehabilitation,Oulu University Hospital,Oulu FI-90029,Finland
cInstitute of Health Sciences,University of Oulu,Oulu FI-90014,Finland
dSchool of Kinesiology,Shanghai University of Sport,Shanghai 200438,China
eDepartmentof Sportand Physical Education,Shanghai Jiao Tong University,Shanghai200240,China
Background:The aim of this study was to compare 6 weeks short-term moderate intensity aerobic exercise and dieting on serum metabolom ics and cardio-metabolic risk factors in pre-menopausal women.
Methods:Ninety previously inactive overweight and obese(BM I 25—35 kg/m2)women(age 41.5±7.6 years)were random ized to either a 6-week Nordic walking exercise program(EX,n=45)or dietary counseling group(DI,n=45).Body composition,serum glucose,insulin and lipids were measured.Serum low-molecular-weight metabolites and lipid constituents were analyzed by nuclear magnetic resonance spectroscopy.Measurements were done at baseline and 7 days after the last training session.
Results:Six weeks aerobic exercise program yielded reductions in serum free fatty acids(-34.7%,95%confidence interval(CI),-50 to-18, p<0.001),glucose(-9.6%,95%CI,-15 to-4,p<0.001)and homeostasis model assessment of insulin resistance(HOMA-IR)(-28.7%, 95%CI,-48 to-10,p=0.005)w ithout changes in body weight or fat mass.Diet counseling resulted in loss of body weight(1.5%,95%CI, -2.3 to-0.7,p=0.001)but no changes in free fatty acids,fasting glucose,or HOMA-IR were found.
Conclusion:Our results indicate thatsmallweight loss does notproduce measurable health benefi ts,whereas short-term regular aerobic exercise can improve glucose and lipid metabolism even in the absence of weight loss in previously sedentary overweight and obese women.
CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.A ll rights reserved.
Dieting;Exercise;Metabolism;Metabolom ics;Women
1.Introduction
The modern way of life,characterized by abundance of energy-enriched foods coupled w ith sedentary lifestyles is associated w ith increased obesity and cardiovascular disease (CVD).1Although men and women are both vulnerable to the ram ifications of modern lifestyles,accumulating evidence indicate that CVD affect more women than men.2This phenomenon is generally attributed to the mounting toll of time simply because women tend to live longer than men.However,another fact that may partly explain the greater cumulative impact of CVD among women is that women usually receive less aggressive treatment for cardiovascular risk factors,and are less often referred to cardiac rehabilitation and CVD prevention programs than men.2,3Such disparity relative to sex in patient care may partly be related to the misconception that women are protected from CVD by estrogen.4However, the cardio-protective effects of estrogen erode during menopause.5,6Many women also tend to express more sedentary behaviorand reduction in leisure-time physicalactivity as they move toward and beyond menopause.7,8Therefore,overweight and obese women are at high risk to develop CVD as they advance from m iddle age to older years.
A recent meta-analysis showed that insulin resistance, hyperinsulinemia,and hyperglycaem ia together w ith hypertriglyceridem ia,low high-density lipoprotein cholesterol(HDLC)and elevated low-density lipoprotein cholesterol(LDL-C) and central obesity,are associated w ith 2-fold increase in cardiovascular outcomes and a 1.5-fold increase in all-cause mortality.9Recent studies have confi rmed the benefi ts of long-term lifestyle changes on these cardiovascular and metabolic risk factors,10,11indicating that the impact of lifestyle decisions on cardiovascular and metabolic health is crucial. However,whether the benefi ts of lifestyle modifications on reducing the risk of CVD are delivered through exercise or changes in dietary habits is not clear.It also remains to be determined whether the benefi ts of exercise and dieting on cardio-metabolic health are visible in the short-term.To address these questions we used nuclear magnetic resonance(NMR)-based metabolic profi ling technologies for acquiring high throughput“snap shots”of a whole organism’s status12allowing the study of the molecular response to exercise and dieting.
The objective of this study was to compare the effect of 6 weeks short-term moderate intensity aerobic exercise program and dietcounseling on cardio-metabolic risk factors and serum metabonomics in previously sedentary pre-menopausal overweight and obese women.
2.M aterials and methods
2.1.Ethical approval
The study protocolwas approved by the EthicalComm ittee of Central Finland Health Care District.W ritten informed consents were obtained from all subjects prior to the assessments.
2.2.Study design
The study subjects were recruited from Jyva¨skyla¨Central Finland Health District/Health Promotion Hospital initiative program.The study was conducted from May to November in 2009.One hundred and sixty-one women(all hospital staff) responded to our invitation.Sample size was estimated for differentpurposes on the primary outcome of the study results (such as physical fi tness measured by walking test and maximum oxygen uptake (VO2max),heart rate (HR) variability,and insulin resistance).All the sample sizes w ill have 85%power to detectdifferences w ithp<0.05 two-sided significance level.Taking into account the compliance and drop-out(10%),the totalnumber of subjects was estimated to meet each specific aims.One hundred met the screening criteria and were invited by phone or e-mail to participate in baseline measurements.A physician exam ined the physical condition of the subjects and ensured that subjects meet the inclusion criteria:20—50 years old pre-menopausal woman w ith a body mass index(BM I)between 25 and 38 kg/m2who participated regular exercise≤2 times/week and≤45 m in/ time,and had no serious cardiovascular or musculoskeletal problems,no diagnosed type I diabetes,and had not lost or gained more than 5 kg in weightduring the previous 6 months. The eligible participants were random ized into parallel exercise(EX)or diet intervention(DI)groups after being enrolled to the study and the qualification being checked.A computer program(http://www.random.org/)was used to generate the random number by blocks(50 numbers in each block).The random ized number was assigned to the subjects according to the order of enrollment.The randomization was done by a researcher thatwas blinded during the trialand was unblinded at the conclusion of the trial.All main investigators in the projectwere also blinded until the end of the intervention.The flow chart of the study participants is given in Fig.1.Ninety women started intervention(n=45 in the exercise group(EX) andn=45 in the diet group(DI)).Eighty-three women completed the 6-week intervention and had follow-up measurements(39 in the EX and 44 in the DI).The study was registered in International Standard Random ized Controlled Trial Number Register(ISRCTN87529813).Full trial protocol is available online (http://www.controlled-trials.com/ ISRCTN87529813/87529813).
2.3.Background information and anthropometrics
Background information including medical history and current health status was collected via self-adm inistered questionnaires.Food consumption and intakes of total energy and energy-yielding nutrients were assessed from 3-day food records at baseline and at the end of the study and analyzed using M icro-Nutrica software developed by the Social Insurance Institution of Finland and updated w ith data for new foodstuffs by the study nutritionist.13
Heightwasdeterm ined using a wall-fixed measuring device, and body mass using a calibrated scale,and from these BM I, which isexpressed as(weight(kg)/height2(m2)),wascalculated. Body composition was assessed using a bioelectricalimpedance analysisdevice(Inbody 720;Biospace Co.Ltd.,Seoul,Republic of Korea).Inbody is a multifrequency impedance plethysmograph body composition analyzer,which takesreadings from the body using an 8-point tactile electrode method.Itmeasures the resistance at five specific frequencies(1 kHz,50 kHz,250 kHz, 500 kHz,and 1 MHz)and reactance atthree specific frequencies (5 kHz,50 kHz,and 250 kHz).Total body water(TBW)was estimated from area,volume,length,impedance,and a constant proportion(specific resistivity).Fat free mass(FFM)wasestimated by dividing TBW by 0.73,and the fatmass(FM)was calculated by subtracting the FFM from the body weight.Precision of the repeated measurements of FM expressed as coefficient of variation was on average 0.6%.Subjects were measured in the morning after 12-h fasting.Before the measurement,subjects were asked to excrete and refrain from drinking excessive amounts ofwater.
2.4.Blood samples
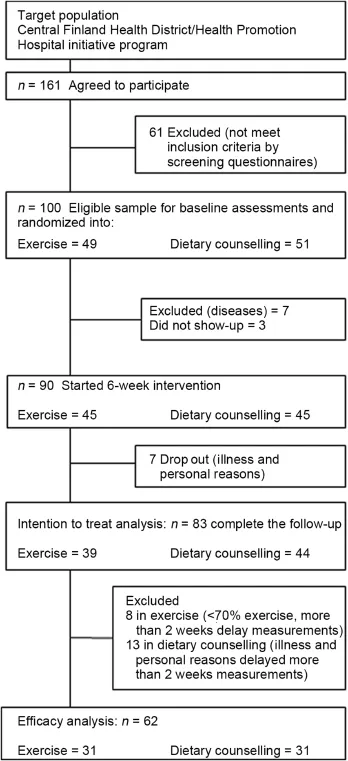
Fig.1.Flow-chart of the study participants.
Venous blood samples for biochem icalanalyses were taken in standardized fasting conditions in the mornings between 7:00 am and 9:00 am before and after intervention.Serum samples were stored frozen at-80°C until analyzed.Serum concentrations of glucose,total and HDL cholesterol,triacylglycerol,and non-esterified fatty acids(NEFA)were analyzed using the KONELAB 20XTi analyzer(Thermo Fischer Scientific Inc.,Waltham,MA,USA).LDL cholesterol was calculated using the Friedewald equation.14Serum fasting insulin concentrations were analyzed using the IMMULITE 1000 analyzer(Siemens Healthcare diagnostics,Mannheim, Germany).The homeostasis model assessment of insulin resistance(HOMA-IR)index was calculated as(fasting insulin concentration×fasting glucose concentration)/22.5.15Serum leptin and adiponectin were measured by ELISA(DuoSetⓇ; R&D Systems,M inneapolis,MN,USA).The interleukin-6 (IL-6) and interleukin-8 (IL-8) concentrations were measured from the serum samples using Cytokine Bead Array (CBA)Flex Sets kit(BD Biosciences,San Diego,CA,USA) and a flow cytometer(FACSCalibur;BD Biosciences)according to the manufacturer’s instructions.The data were analyzed by using FCAP Array software(BD Biosciences). All measurements were performed after 12 h fasting at baseline and 7 days after the last training session to m inimize any acute effects of exercise.
2.5.Serum NMR metabonomics
All serum samples were analyzed using a high-throughput serum NMR metabonom ics platform;the experimental protocols including sample preparation and NMR spectroscopy have been described in detail elsewhere.12,16,17This platform provides comprehensive quantitative information on lipoprotein subclass concentrations,low-molecular-weight metabolites such as am ino acids,ketone bodies,and gluconeogenic intermediates and detailed molecular information on serum lipids including,e.g.,Ω-3 andΩ-6 fatty acids.This platform has recently been applied in various large-scale epidemiological and genetic studies.18—21
2.6.Fitness test
VO2max(m L/kg/m in)was assessed by a bicycle ergometer under the supervision of a physician.The test began w ith a 2-min warm-up at50 W.After that the intensity was increased by 25 W at 2-min intervals until exhaustion.Electrocardiography was monitored and continuously and HR and maximal work load were recorded at the end of every load.Oxygen uptake was assessed by breath-by-breath method using respiratory gas analyzer(Sensor Medics Vmax,Yorba Linda,CA, USA).Maximal oxygen uptake was reached,when measured VO2reached a plateau orstarted to decrease orsubject feltshe had reached her maximal level and wanted to stop the test.
2.7.Exercise program
Nordic walking(walking with poles)was chosen as the intervention exercise.A specific training program was developed afterbaseline assessmentson the basis ofeach individual’smaximum HR measured during the VO2maxtest.The exercise program was progressive based on the recommendation for sedentary adults.For intervention week 1,the intensity of exercise was 60%ofmaximum HR,for60 min persession and 3 times a week;for intervention weeks 2 and 3 the intensity of exercise was 65%of maximum HR for 45 m in per time and 4 times a week;for intervention weeks 4 and 5,the intensity of exercise was 70%ofmaximum HR for35 m in persession and 4 times a week;and for intervention week 6,the intensity of exercise was 75%ofmaximum HR for30 min per session and 3 times a week.Nordic walking was supervised at the beginning of the intervention(week 1).From week 1 onwards subjects followed the daily guidance of the w rist computer(Suunto Oy; Fitness line,Vantaa,Finland)to exercise 30 m in to 1 h a time and gradually increase the intensity and duration and participated in supervised exercise sessions tw ice perweek.
2.8.Dietary intervention
The DI group received dietary instruction from a clinical nutritionist according to the guidelines of Finnish nutrition recommendations targeting to lose 3 kg of body weight in 6 weeks(National Nutrition Council 2005).The instruction included controlling energy intake by reducing portion size using the plate model;controlling meal rhythm and regular eating between 3 and 4 h intervals;changing the composition of food stuffs including using light margarine(less than 40% fat)and vegetable oils,low-fat milk products,low-fat meat products and fish,lightbakery products,increasing fiber intake using whole-wheat products,vegetables,root vegetables, berries,fruits,and avoiding products rich in sugar;drinking 1.5—2 L of water per day,m ineral water,m ild juices,light beverages,coffee,and tea,and moderating alcohol consumption,preferably of m ildly alcoholic drinks only.In addition, subjects in the DI group were instructed to maintain their habitual physicalactivity butno specific exercise program was provided during the intervention.
2.9.Statistical analyses
A ll data were checked for normality using the Shapiro—W ilk’sWtest in SPSS 20 for W indows(SPSS Inc.,Chicago,IL,USA).If data were not normally distributed,a natural logarithm transform was applied.An intention-to-treat(ITT)analysis was performed to compare the EX to the DIgroup.The effects of the interventions were assessed using analysis of covariance(ANCOVA)for repeated measures(treatment group× time)w ith baseline values as a covariate.In addition to the ITT analysis,efficacy analysis was performed.Among the 83 women who had both baseline and follow-up assessments,21 were excluded from the efficacy analysis due to the follow ing reasons:in EX group,not completing at least 70%of exercise training (n=5),and more than 2 weeks delay in participating in the follow-up assessments(n=3);in the DI group,flu or other illness(n=7)and more than 2 weeks delay in participating in the follow-up assessments(n=6)(Fig.1).The percentage changes from baseline to follow-up were calculated and the comparison of percentage changes in different groups was performed usingttests.The data were presented as mean±SD.The level of statistical significance chosen for the comparisons wasp<0.05.
3.Results
At baseline,the DI group weighed more,had greater fat mass,visceral fat area,BM I,and leptin compared to the EX group(allp<0.05,Table 1).The DI group also had higher α-1-acid glycoprotein,pyruvate,isoleucine,leucine,phenylalanine,and tyrosine levels atbaseline(allp<0.05,Table 2). No differences in serum lipids,glucose,cytokines,aerobic fi tness,or dietary intake between groups were found.
3.1.Intention to treat
After 6 weeks intervention serum free fatty acids,glucose and HOMA-IR were significantly reduced in the EX group compared to the DI group(p<0.05 for all,Table 1).No significant differences(group by time interaction)in body weight,fat mass,visceral fat area and BM I were observed. Serum acetate and pyruvate decreased and lactate,glutam ine, lactate to pyruvate ratio,Ω-3 fatty acids,polyunsaturated fatty acids and DHA increased in the DIgroup butnot in EX group w ith time,and did not show significant group-by-time differences,except for glutam ine and lactate to pyruvate ratio (p=0.041 andp=0.007,Table 2).Tyrosine increased in the EX group but not in the DI group w ith time while phenylalanine,histidine,glycine,andα-1-acid glycoprotein increased significantly in both groups over time,butno significantgroup by time differences were found.
3.2.Efficacy analysis
Body weight decreased(on average 1 kg)significantly in the DI group compared to the EX group(1.2%,p<0.05, Fig.2),while significant reduction(group-by-time)in serum free fatty acids(27.6%,p< 0.001),glucose(11.1%,p<0.001),and HOMA-IR(21.2%,p=0.021)was observed in the EX group(Fig.3).DHA(26.3%,p=0.001)and lactate to pyruvate ratio(23%,p=0.003)increased significantly in the DIgroup compared to the EX group(Fig.4).
4.Discussion
The main findings of this study were that 6 weeks of moderate intensity aerobic exercise in previously sedentary overweight and obese premenopausal women was associated w ith significant reductions in serum free fatty acid,glucose, and HOMA-IR,w ithoutchange in body weight,while 6 weeks of dietary counseling resulted in a small degree of weight loss w ith no observable improvements in glucose or lipid metabolism.
Lifestyle interventions have been shown to be useful tools in treating cardio-metabolic disorders in pre-menopausal and post-menopausal women.22—24Lim ited research on the effects of hormone replacement therapy (HRT)and exercise on CVD risk factors in healthy postmenopausal women show that exercise and HRT have both independent and complimentary effects on body composition and serum lipid profi les.25—27The discrepancy may be due to differences in the type,amount and intensity of exercise and low sample sizes.28Nevertheless,recent studies suggest that w ith regard to lifestyle interventions,the greatest benefi ts arise from combined programs of exercise and dieting for both pre-29,30and post-menopausal women.31,32These health benefi ts seem to be attributed to weight loss achieved in the course of several months or years.33,34In the present study,DI group failed to achieve the targeted reduction of 3 kg of body weight in 6 weeks.As a result,no significant improvements in cardio-metabolic risk factors were observed,suggesting that lifestyle intervention using only dietary approaches may need considerably more significant energy restriction and longer duration in order to induce favorable changes in body weight and cardio-metabolic health.Exercise training,however,resulted in signifi cant reduction in free fatty acids,glucose,and HOMA-IR in the absence of weight loss.
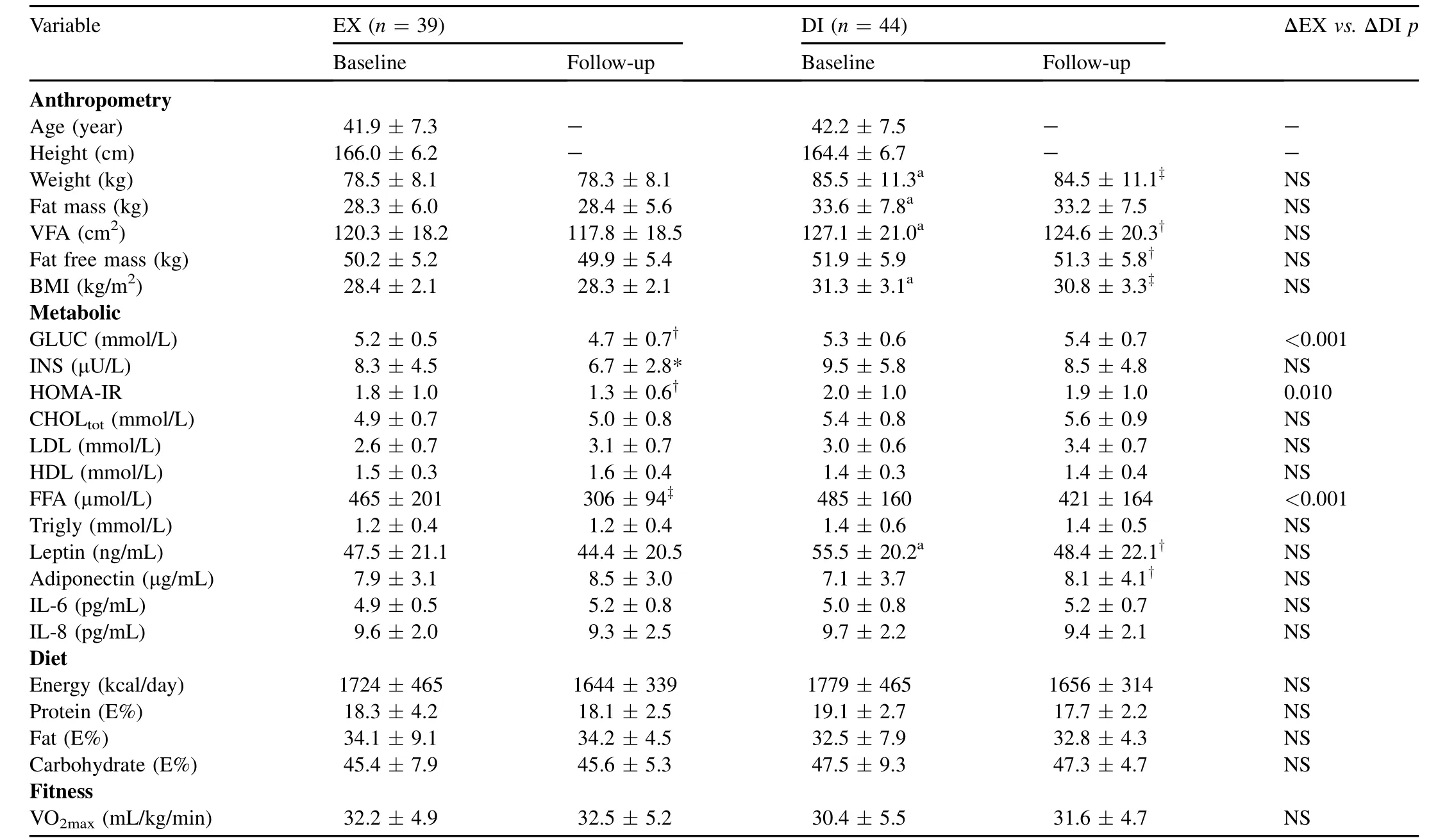
Table 1 Subject characteristics at baseline and after intervention(intention-to-treat)(mean±SD).
These findings are in agreement w ith a previous study that showed short-term(4 weeks)aerobic exercise decreased circulating free fatty acids w ithoutweight loss in previously sedentary obese men and pre-menopausal women.35In that study,signifi cant decrease in hepatic and visceral lipids was also observed,indicating that short-term aerobic exercise can m itigate cardiovascular risk and this is not contingent upon weight loss.In the present study,we did not measure hepatic content but exercise training tended to result in reduction in visceral fat.Therefore,we cannot rule out that reduction in hepatic and visceral fatmay have contributed to the reduction of free fatty acids,glucose,and insulin resistance in the EX group.However,dieting resulted in reduction in visceral fatw ithout concurrent changes in either lipid or glucose metabolism.These observations do not support the notion that reduction in free fatty acids and insulin resistance w ithin EX group was attributed to reduction of visceral fat.
To delineate the metabolic shifts underlying our observations we performed NMR-based serum metabolomics analysis. However,given the significant reduction in serum fatty acids and glucose in the EX group,surprisingly subtle changes were observed in serum metabolites levels.No change in leptin oradiponectin concentrations was observed after exercise training,whilst dieting significantly decreased leptin and increased adiponectin levels,indicating that the reduction in serum glucose and free fatty acids did not result from insulin sensitizing effects of adipokines.36Exercise training was not associated w ith changes in beta hydroxybutyrate to acetoacetate ratio or lactate to pyruvate ratio which are indicators of redox state in m itochondria,37suggesting that the beneficial effects of aerobic exercise on glucose and lipid metabolism was not ascribed to reduced reactive oxygen species production.Exercise resulted in increased serum phenylalanine and glycine and,to a lesser significant extent,tyrosine and histidine concentrations.Increased levels of serum phenylalanine and tyrosine have been associated w ith obesity and insulin resistance in previous studies,38whereas increased serum glycine has been associated w ith increased insulin sensitivity and fatty acid oxidation.39Thus,reductions in insulin resistance and serum free fatty acids in the EX group may have resulted from recovery of serum glycine concentrations and subsequent increase in m itochondrial function.Moreover,it has been shown that,in sedentary subjects,greater metabolic stress results in adaptation manifested by improved muscular mitochondrialbiogenesis and enhanced fatty acid oxidation,40which thereby may accelerate fatty acid removal from circulation.41Therefore,it is plausible that the mitochondrial adaptation to progressive exercise training was responsible for the reduction in free fatty acids and the subsequent reduction in insulin resistance in the present study.
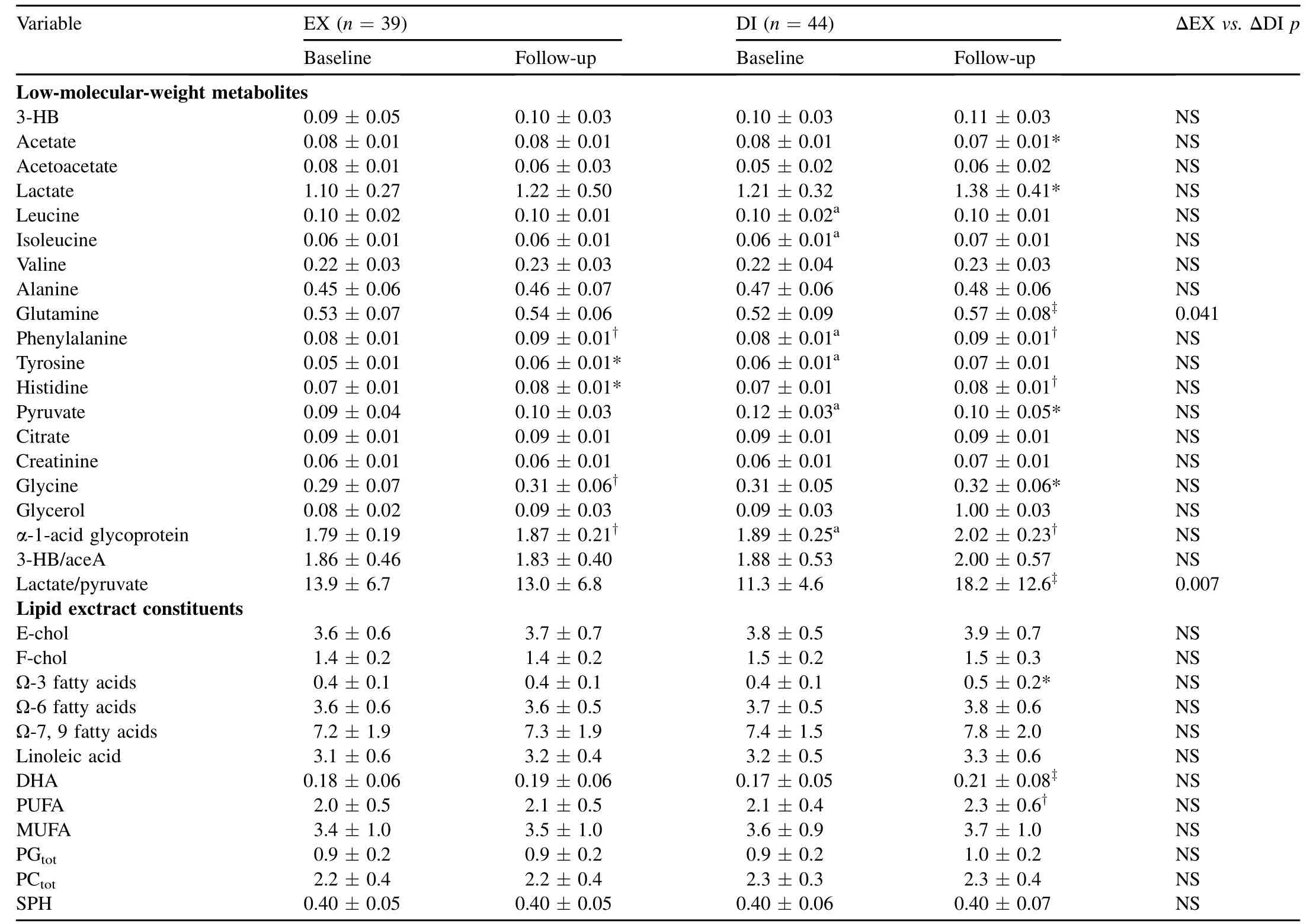
Table 2 Serum low-molecular-weight metabolites and lipid constituents at baseline and after intervention(intention-to-treat)(mean±SD).
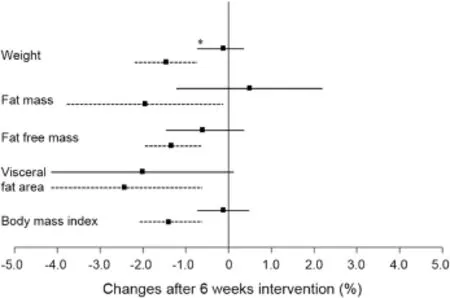
Fig.2.Mean changes of body composition(efficacy analysis)in women in the exercise(n=31,solid line)and dietary counseling(n=31,dotted line) groups.Squares represent mean values and lines indicate 95%confidence interval.*p<0.05,compared to diet group.
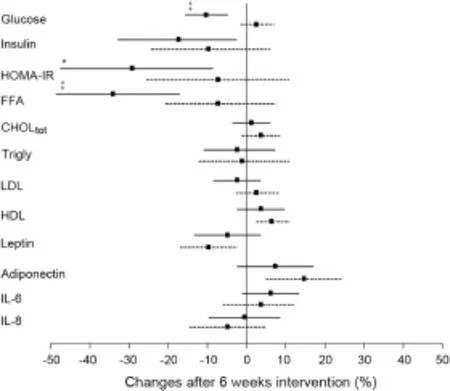
Fig.3.Mean changes of metabolic measures(efficacy analysis)in women in the exercise(n=31,solid line)and dietary counseling(n=31,dotted line) groups.Squares represent mean values and lines indicate 95%confidence interval.*p<0.05,■p<0.001,compared to diet group.FFA=free fatty acids;CHOLtot= total cholesterol;LDL = low density lipoprotein; HDL=high density lipoprotein.
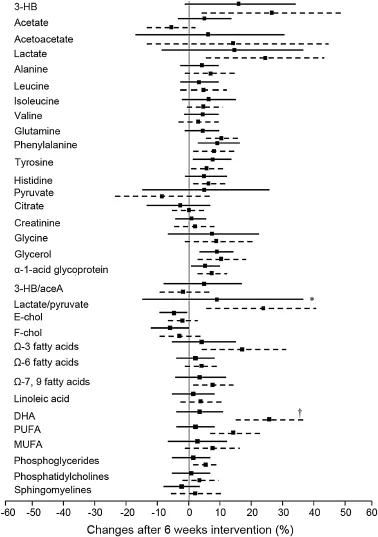
Fig.4.Mean changes of serum metabolites(efficacy analysis)in women in the exercise(n=31,solid line)and dietary counseling(n=31,dotted line). Squares represent mean values and lines indicate 95%confidence interval. *p<0.05,†p<0.01,compared to exercise group.3-HB=3-hydroxybutyrate; 3-HB/aceA=3-hydroxybutyrate to acetoacetate ratio;E-chol=esterified cholesterol;F-chol=free cholesterol;DHA=docosahexaenoic acid; PUFA=polyunsaturated fatty acids;MUFA=monounsaturated fatty acids.
The strength ofour randomized trialstudy design reached the methodological requirements of physicalactivity trials42to provide reliable and valid evidence on the effects of exercise.Our design also focused on moderate progressive aerobic exercise training because this is what is recommended in most public health guidelines for adults.43All the samples were analyzed in the same laboratory at the same time by a same person.However, the current study is lim ited by the homogeneous subjects consisting Finnish women.Therefore,our results may notbe transferrable to the general population.The fact that we used bioimpedance instead of dual-energy X-ray absorptiometry or magnetic resonance imaging to define body composition may predispose our results to measurement error.44Furthermore, VO2maxwasdefined by bicycle ergometer,while exercise training consisted ofNordic walking.Thismay wellaccountfor the failure to detectsignificantchanges in aerobic fi tness by VO2maxtest.
5.Conclusion
The results of the currentstudy show that smallweight loss induced by dieting does notproduce measurable health benefi ts in serum level,whereas short-term regular aerobic exercise can improve glucose and lipid metabolism even in the absence of weightlossin previously sedentary overweightand obese women.
Acknow ledgm ent
This study was financially supported by Suunto Oy(Grant 28.5.2009)and University of Jyva¨skyla¨Wellness program,the Shanghai Overseas Distinguished Professor Award Program 2013;and the Chinese M inistry of Science and Technology, China National Science and Technology Infrastructure Program 2012(Grant 2012BAK21B03-4).
1.Hu G,Lindstrom J,Jousilahti P,Peltonen M,Sjoberg L,Kaaja R,et al. The increasing prevalence ofmetabolic syndrome among Finnish men and women over a decade.J Clin Endocrinol Metab2008;93:832—6.
2.Mosca L,Linfante AH,Benjam in EJ,Berra K,Hayes SN,Walsh BW, et al.National study of physician awareness and adherence to cardiovascular disease prevention guidelines.Circulation2005;111: 499—510.
3.Ll Lloyd GW.Preventive cardiology and cardiac rehabilitation programmes in women.Maturitas2009;63:28—33.
4.Daniels KM,Arena R,Lavie CJ,Forman DE.Cardiac rehabilitation for women across the lifespan.Am J Med2012;125:937.e1—7.
5.Guthrie JR,Taffe JR,Lehert P,Burger HG,Dennerstein L.Association between hormonalchanges atmenopause and the risk of a coronary event: a longitudinal study.Menopause2004;11:315—22.
6.Kuh D,Langenberg C,Hardy R,Kok H,Cooper R,Butterworth S,et al. Cardiovascular risk atage 53 years in relation to the menopause transition and use of hormone replacement therapy:a prospective British birth cohort study.BJOG2005;112:476—85.
7.Sui X,Zhang J,Lee DC,Church TS,Lu W,Liu J,etal.Physical activity/ fi tness peaks during perimenopause and BM I change patterns are not associated w ith baseline activity/fi tness in women:a longitudinal study w ith a median 7-year follow-up.Br J Sports Med2013;47:77—82.
8.Chomistek AK,Manson JE,Stefanick ML,Lu B,Sands-Lincoln M, Going SB,et al.Relationship of sedentary behavior and physical activity to incident cardiovascular disease:results from the Women’s Health Initiative.J Am Coll Cardiol2013;61:2346—54.
9.Mottillo S,Filion KB,Genest J,Joseph L,Pilote L,Poirier P,et al.The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis.J Am Coll Cardiol2010;56:1113—32.
10.Saaristo T,Moilanen L,Korpi-Hyovalti E,Vanhala M,Saltevo J, Niskanen L,etal.Lifestyle intervention for prevention of type 2 diabetes in primary health care:one-year follow-up of the Finnish National Diabetes Prevention Program(FIN-D2D).Diabetes Care2010;33:2146—51.
11.Voeghtly LM,Neatrour DM,Decew icz DJ,Burke A,Haberkorn MJ, Lechak F,et al.Cardiometabolic risk reduction in an intensive cardiovascular health program.Nutr Metab Cardiovasc Dis2013;23:662—9.
12.Soininen P,Kangas AJ,Wurtz P,Tukiainen T,Tynkkynen T, Laatikainen R,et al.High-throughput serum NMR metabonomics for cost-effective holistic studies on systemic metabolism.Analyst2009;134:1781—5.
13.Lyytikainen A,Lamberg-Allardt C,Kannas L,Cheng S.Food consumption and nutrientintakesw ith aspecialfocuson milk productconsumption in early pubertalgirls in Central Finland.Public Health Nutr2005;8:284—9.
14.Friedewald WT,Levy RI,Fredrickson DS.Estimation of the concentration of low-density lipoprotein cholesterol in plasma,w ithout use of the preparative ultracentrifuge.Clin Chem1972;18:499—502.
15.Matthews DR,Hosker JP,Rudenski AS,Naylor BA,Treacher DF, Turner RC.Homeostasis model assessment:insulin resistance and betacell function from fasting plasma glucose and insulin concentrations in man.Diabetologia1985;28:412—9.
16.Tukiainen T,Tynkkynen T,Makinen VP,Jylanki P,Kangas A, Hokkanen J,et al.A multi-metabolite analysis of serum by 1H NMR spectroscopy:early system ic signs of A lzheimer’s disease.Biochem Biophys Res Commun2008;375:356—61.
17.Inouye M,Kettunen J,Soininen P,Silander K,Ripatti S,Kumpula LS, etal.Metabonom ic,transcriptomic,and genom ic variation of a population cohort.Mol Syst Biol2010;6:441.http://dx.doi.org/10.1038/msb.2010.93.
18.Chambers JC,Zhang W,Sehm i J,Li X,Wass MN,Van der Harst P,etal. Genome-w ide association study identifies loci influencing concentrations of liver enzymes in plasma.Nat Genet2011;43:1131—8.
19.Ehret GB,Munroe PB,Rice KM,Bochud M,Johnson AD,Chasman DI, et al.Genetic variants in novel pathways infl uence blood pressure and cardiovascular disease risk.Nature2011;478:103—9.
20.Kettunen J,Tukiainen T,Sarin AP,Ortega-A lonso A,Tikkanen E, Lyytikainen LP,et al.Genome-w ide association study identifies multiple loci influencing human serum metabolite levels.NatGenet2012;44:269—76.
21.Stancakova A,Paananen J,Soininen P,Kangas AJ,Bonnycastle LL, Morken MA,et al.Effects of 34 risk loci for type 2 diabetes or hyperglycem ia on lipoprotein subclasses and their composition in 6,580 nondiabetic Finnish men.Diabetes2011;60:1608—16.
22.Oh EG,Bang SY,Hyun SS,Kim SH,Chu SH,Jeon JY,etal.Effects of a 6-month lifestyle modification intervention on the cardiometabolic risk factors and health-related qualities of life in women w ith metabolic syndrome.Metabolism2010;59:1035—43.
23.Carroll S,Borkoles E,Polman R.Short-term effects of a non-dieting lifestyle intervention program on weight management,fi tness,metabolic risk,and psychological well-being in obese premenopausal females w ith the metabolic syndrome.Appl Physiol Nutr Metab2007;32:125—42.
24.Imayama I,Ulrich CM,Alfano CM,Wang C,Xiao L,Wener MH,etal. Effects of a caloric restriction weight loss diet and exercise on inflammatory biomarkers in overweight/obese postmenopausal women:a random ized controlled trial.Cancer Res2012;72:2314—26.
25.Binder EF,Birge SJ,Kohrt WM.Effects of endurance exercise and hormone replacement therapy on serum lipids in older women.J Am Geriatr Soc1996;44:231—6.
26.Figueroa A,Going SB,M illiken LA,Blew RM,Sharp S,Teixeira PJ,etal. Effects of exercise training and hormone replacement therapy on lean and fat mass in postmenopausal women.J Gerontol A Biol Sci Med Sci2003;58:266—70.
27.Lindheim SR,Notelovitz M,Feldman EB,Larsen S,Khan FY, Lobo RA.The independent effects of exercise and estrogen on lipids and lipoproteins in postmenopausal women.ObstetGynecol1994;83:167—72.
28.Haddock BL,Marshak HP,Mason JJ,Blix G.The effect of hormone replacement therapy and exercise on cardiovascular disease risk factors in postmenopausal women.Sports Med2000;29:39—49.
29.Meckling KA,Sherfey R.A random ized trial of a hypocaloric highprotein diet,w ith and w ithout exercise,on weight loss,fi tness,and markers of the metabolic syndrome in overweightand obese women.Appl Physiol Nutr Metab2007;32:743—52.
30.Lofgren IE,Herron KL,West KL,Zern TL,Brownbill RA,Ilich JZ,etal. Weight loss favorably modifies anthropometrics and reverses the metabolic syndrome in premenopausal women.JAmColl Nutr2005;24:486—93.
31.Foster-Schubert KE,A lfano CM,Duggan CR,Xiao L,Campbell KL, Kong A,etal.Effectof dietand exercise,alone or combined,on weight and body composition in overweight-to-obese postmenopausal women.Obesity(Silver Spring)2012;20:1628—38.
32.Abbenhardt C,M cTiernan A,Alfano CM,Wener MH,Campbell KL, Duggan C,et al.Effects of individual and combined dietary weight loss and exercise interventions in postmenopausal women on adiponectin and leptin levels.J Intern Med2013;274:163—75.
33.Brown TJ.Health benefi ts ofweight reduction in postmenopausalwomen: a systematic review.J Br Menopause Soc2006;12:164—71.
34.Kuller LH,Pettee Gabriel KK,Kinzel LS,Underwood DA,Conroy MB, Chang Y,et al.The women on the move through activity and nutrition (woman) study:final 48-month results.Obesity(SilverSpring)2012;20:636—43.
35.Johnson NA,Sachinwalla T,Walton DW,Sm ith K,Armstrong A, Thompson MW,et al.Aerobic exercise training reduces hepatic and visceral lipids in obese individuals w ithout weight loss.Hepatology2009;50:1105—12.
36.Dyck DJ.Adipokines as regulators of muscle metabolism and insulin sensitivity.Appl Physiol Nutr Metab2009;34:396—402.
37.Corkey BE.Banting lecture 2011:hyperinsulinem ia:cause or consequence?Diabetes2012;61:4—13.
38.Adams SH.Emerging perspectives on essentialam ino acid metabolism in obesity and the insulin-resistant state.Adv Nutr2011;2:445—56.
39.Huffman KM,Slentz CA,Bateman LA,Thompson D,Muehlbauer MJ, Bain JR,et al.Exercise-induced changes in metabolic intermediates, hormones,and inflammatory markers associated w ith improvements in insulin sensitivity.Diabetes Care2011;34:174—6.
40.Baar K.The signaling underlying FITness.Appl Physiol Nutr Metab2009;34:411—9.
41.Thompson PD,Cullinane EM,Sady SP,Flynn MM,Chenevert CB, Herbert PN.High density lipoprotein metabolism in endurance athletes and sedentary men.Circulation1991;84:140—52.
42.Schm itz KH,Holtzman J,Courneya KS,Masse LC,Duval S,Kane R. Controlled physical activity trials in cancer survivors:a systematic review and meta-analysis.CancerEpidemiolBiomarkersPrev2005;14:1588—95.
43.Pal S,Cheng C,Ho S.The effect of two different health messages on physical activity levels and health in sedentary,overweight middle aged women.BMC Public Health2011;11:204.
44.Jensky-Squires NE,Dieli-Conw right CM,Rossuello A,Erceg DN, M cCauley S,Schroeder ET.Validity and reliability of body composition analysers in children and adults.BrJNutr2008;100:859—65.
Received 3 February 2014;revised 3 March 2014;accepted 11 March 2014
*Corresponding author.Schoolof Kinesiology,ShanghaiUniversity of Sport, Shanghai 200438,China.
E-mail address:shulin.cheng@jyu.fi(S.Cheng)
Peer review under responsibility of Shanghai University of Sport
2095-2546/$-see front matter CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.A ll rights reserved. http://dx.doi.org/10.1016/j.jshs.2014.03.013
 Journal of Sport and Health Science2014年3期
Journal of Sport and Health Science2014年3期
- Journal of Sport and Health Science的其它文章
- Women’s health in exercise and aging:What do we know?
- Why women see differently from the way men see?A review of sex differences in cognition and sports
- Sex differences in exercise and drug addiction:A m ini review of animal studies
- Women and exercise in aging
- Effects of carbohydrate supplements on exercise-induced menstrual dysfunction and ovarian subcellular structural changes in rats
- Exercise training and antioxidant supplementation independently improve cognitive function in adult male and female GFAP-APOE m ice