
多排螺旋 CT 血管成像对评估肢体骨骼肌肉肿瘤毗邻血管受侵的临床价值
2014-02-14 09:01:57张毅军
中国骨与关节杂志 2014年11期
刘 刚 张毅军
. 骨科影像学 Orthopaedic radiology .
多排螺旋 CT 血管成像对评估肢体骨骼肌肉肿瘤毗邻血管受侵的临床价值
刘 刚 张毅军
目的通过与手术所见对比,评价多排螺旋 CT 血管成像 ( multi-slice spiral computerized tomography angiograph,MDCTA ) 判定骨骼肌肉肿瘤毗邻血管受侵的临床价值。方法回顾性分析 2008 年1 月至 2014 年 6 月,我院经 MRI 诊断为骨骼肌肉肿瘤并侵犯其毗邻血管的患者 21 例,所有患者均行手术治疗,并在术前进行 MDCTA 检查。其中男 12 例,女 9 例;平均年龄 33 岁;肢体骨肿瘤 11 例,肢体软组织肿瘤 10 例。采用双盲法通过 MDCTA 判断是否存在肿瘤毗邻血管受侵。以手术所见为金标准,进行统计学分析对比。结果12 例 MDCTA 未显示血管受侵者,手术所见也为阴性 ( 真阴性 12 例 );9 例 MDCTA 显示血管受侵者中,3 例虽术中发现血管与肿瘤粘连,但易于分离,被认为术中所见为阴性 ( 假阳性 3 例 ),其余 6 例手术证实血管受侵 ( 真阳性 6 例 )。对比手术所见,MDCTA 的敏感性为 100%,特异性为 80%,阳性预测值为66.7%,阴性预测值为 100%,准确率为 85.7%。结论MDCTA 评价骨骼肌肉肿瘤对毗邻血管侵犯更为准确,可提供真实可靠的影像学信息。
体层摄影术,螺旋计算机;血管造影术;骨肿瘤;软组织肿瘤;肿瘤浸润
在肢体骨骼肌肉肿瘤手术前,骨科医生常需要了解肿瘤毗邻血管受侵情况。MRI 作为骨骼肌肉肿瘤以及骨肿瘤样病变最有价值的检查方法[1-3],尽管可在肿瘤结构、大小、对周围组织侵犯方面,提供极具价值的影像学信息,但是在评价肿瘤与其毗邻主要血管的解剖关系方面却不尽如人意[4-5]。随着近 10 年来影像后处理技术的进步,多排螺旋 CT血管成像 ( multi-slice spiral computerized tomography angiograph,MDCTA ) 已经成为广受欢迎的评估血管结构的检查方法。回顾性分析 2008 年 1 月至2014 年 6 月,我院经 MRI 诊断为骨骼肌肉肿瘤并侵犯其毗邻血管的患者 21 例,所有患者均行手术治疗,并在术前进行 MDCTA 检查。对比 MDCTA 判定肿瘤毗邻血管受侵情况与手术所见的一致性,探讨MDCTA 在评价骨骼肌肉肿瘤毗邻血管受侵的临床价值,现报道如下。
资料与方法
一、一般资料
本组共 21 例,男 12 例,女 9 例,平均年龄33 ( 12~69 ) 岁。其中肢体骨肿瘤 11 例,肢体软组织肿瘤 10 例。骨肿瘤位于股骨 ( n=7 ),胫骨 ( n=3 ),腓骨 ( n=1 );软组织肿瘤位于大腿 ( n=5 ),腋部 ( n=1 ),上臂 ( n=1 ),小腿 ( n=3 )。所有病例在进行 MDCTA 之前均行穿刺活检,其中骨肉瘤9 例,尤文氏肉瘤 2 例,脂肪肉瘤 3 例,多形细胞肉瘤 1 例,恶性外周神经鞘瘤 2 例,恶性纤维组织细胞瘤 1 例,梭形细胞间质瘤 1 例,滑膜肉瘤1 例,良性间叶瘤 1 例,在行 MRI 检查后 1~7 天( 平均 3 天 ) 进行 MDCTA 检查,在 MDCTA 检查后6~13 天 ( 平均 9 天 ) 进行手术。
二、MRI 检查
MRI 怀疑肿瘤毗邻血管受侵标准:( 1 ) 肿瘤与邻近血管之间缺乏正常组织;( 2 ) 血管被肿瘤推压移位;( 3 ) 血管被肿瘤包埋。所有病例均应用德国西门子公司生产的 1.5 T NOVUS 超导型 MRI 成像系统进行扫描:常规选择横断面 T1WI 和 T2WI 扫描,均采用快速自旋回波序列 ( turbo spin echo,TSE )。
三、MDCTA 检查
1. 仪器设备:所有病例均采用 Phillips 公司的Brilliance iCT 扫描机 ( 128 排 256 层螺旋 CT 采集成像系统 );影像后处理工作站采用 Phillips 公司 EBW ( extended brilliance workspace ) 工作站、高级血管分析 ( advantage vessel analysis,AVA ) 软件;高压注射器采用美国 Medra 公司双筒高压注射器 ( 型号SCT 211 );对比剂采用碘海醇 ( 350 mg / ml ) 注射液,美国通用电气药业 ( 上海 ) 有限公司生产。
2. 扫描参数设置:管电压 120 kV,管电流280~360 mA,层厚 1.25 mm,间隔 5 mm,螺距0.985∶1,扫描总时间为 25~35 s。延迟时间采用智能触发法,利用 Smartprep 跟踪技术,将感兴趣区设置在腹主动脉远端,将启动扫描阈值设为 120 HU,延迟时间设为 10 s。
3. 扫描方法:患者取仰卧位,头先进,扫描范围一般从 L4椎体下缘水平扫描至足尖,将 100~150 ml 对比剂经高压注射器从肘前静脉留置的套管针注入,注射速率控制在 3.5~4.0 ml / s。将以上采集到的原始图像经薄层重建后传输至影像工作站。
四、CT 血管造影 ( computerized tomography angiograph,CTA ) 所见评价
所有病例经 2 位放射科高年资主治医生通过双盲法进行评价:在影像工作站上利用 AVA 软件,以断层图像为基础,当怀疑血管受侵后,采用 MIP、MPR、VR 各种重建方式显示受累血管,综合各种重建图像,最终得出结论。MDCTA 诊断血管受侵的标准:( 1 ) 肿瘤与血管之间脂肪层消失;( 2 ) 肿瘤毗邻血管移位;( 3 ) 肿瘤毗邻血管局部管腔狭窄。
五、手术所见
术中观察肿块毗邻血管是否受侵:当肿瘤毗邻血管无法剥离,则视为手术所见阳性,此类患者常需要血管搭桥手术替代受侵血管或进行截肢手术;对血管被肿瘤粘连包埋,但在术中能够剥离者,则视为手术所见阴性。
六、统计学分析
以术中所见为金标准,应用 kappa 一致性检验评价结果的一致性 ( P<0.05 ),分别评估 MDCTA诊断肢体骨骼肌肉肿瘤毗邻血管受侵的敏感性、特异性、阳性预测值、阴性预测值以及准确度,使用SPSS 17.0 软件进行统计学分析。
结 果
一、MRI 所见
由于本组收集的所有病例都被 MRI 诊断为血管受侵,故以手术所见为金标准,MRI 的敏感度为100% ( 6 / 6 ),阳性预测值为 28.6% ( 6 / 21 )。
二、MDCTA 与手术所见对比
本组 21 例中,12 例 CTA 示肿瘤与血管结构之间有清晰明确的脂肪层,诊断为血管受侵阴性;其余 9 例 CTA 示肿瘤与血管结构之间脂肪层消失,诊断为血管受侵阳性。CTA 发现 16 例出现毗邻血管移位,6 例出现毗邻血管管腔狭窄。在 6 例肿瘤毗邻血管管腔狭窄的患者中,4 例手术证实为阳性,2 例手术证实为阴性;在 15 例 CTA 未见毗邻血管管腔狭窄病例中有 1 例手术发现血管受侵;有 5 例 CTA 未见血管移位者,术中亦未发现血管受侵 ( 表 1~3 )。
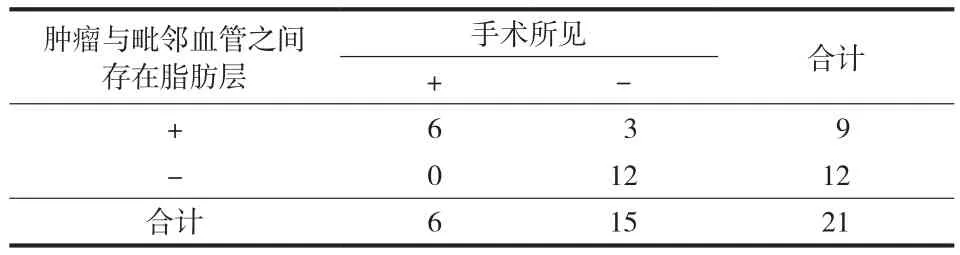
表1 MDCTA 通过肿瘤与毗邻血管之间是否存在脂肪层诊断血管受侵与手术所见比较 ( 例 )Tab.1 Dianosis of vascular invasion in the patients with or without a fat layer between tumors and vessels in MDCTA examination was confrmed by surgical fndings ( case )
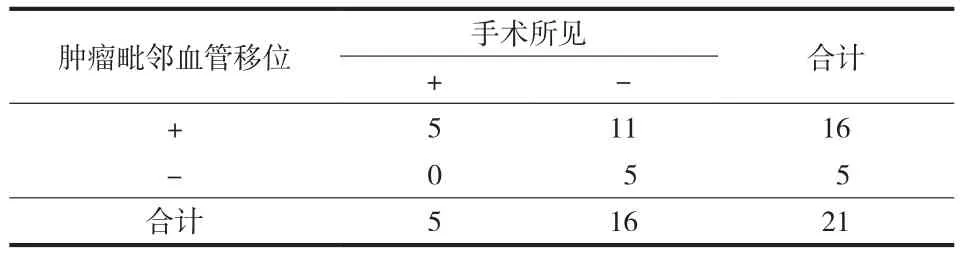
表2 MDCTA 通过肿瘤毗邻血管移位诊断血管受侵与手术所见比较 ( 例 )Tab.2 Dianosis of vascular invasion in the patients with or without vascular displacement in MDCTA examination was confirmed by surgical fndings ( case )
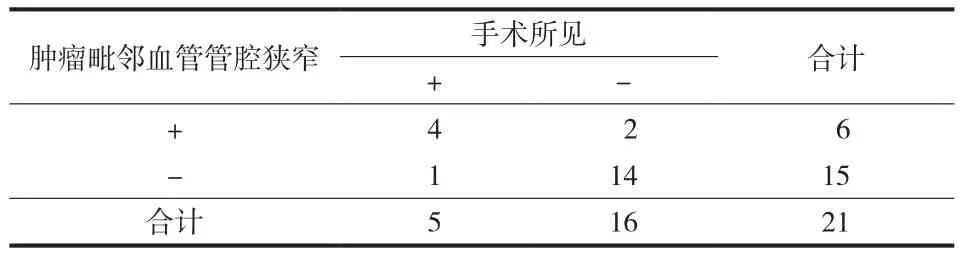
表3 MDCTA 通过肿瘤毗邻血管管腔狭窄诊断血管受侵与手术所见比较 ( 例 )Tab.3 Dianosis of vascular invasion in the patients with or without artery stenosis in MDCTA examination was confirmed by surgical fndings ( case )
CTA 诊断为血管受侵阴性的 12 例,在术中可见肿瘤与其毗邻血管之间有明显的正常组织以及脂肪层。其余 9 例,术中发现有 3 例血管部分与肿瘤粘连,但在手术中很容易被剥离,故被视为手术所见阴性,另 6 例由于血管受侵严重,无法剥离,行与肿瘤一并切除并血管搭桥手术或截肢手术。
受肿块压迫所导致的血管腔中度狭窄会引起继发性移位,所以,这些所见不足以诊断血管受侵。我们认为,MDCTA 所见肿瘤与毗邻血管之间的是否存在清晰脂肪层是评价血管是否受侵的重要因素( 图 1,2 ),当我们把这一因素与手术所见进行对比后发现,其敏感性为 100%,特异性为 80%,阳性预测值为 66.7%,阴性预测值为 100%,准确度为85.7% ( P=0.002 ) ( 表 4 )。
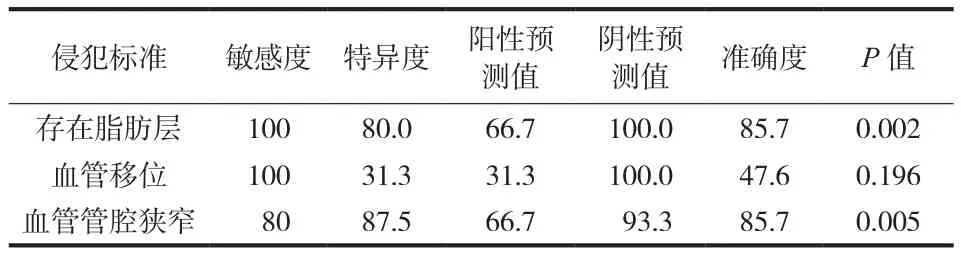
表4 以手术所见为金标准,CTA 与手术所见统计学对比 ( % )Tab.4 Statistical conparison between CTA examination results and surgical findings with the surgical findings as the golden standard ( % )

图1 患者,男,15 岁,MRI 检查怀疑“右股骨远端恶性肿瘤性病变毗邻动脉受侵”。经穿刺活检,病理回报证实为骨肉瘤。CTA 显示右股骨下段骨皮质不连续,可见穿凿样骨质破坏,破坏的骨皮质周围可见不规则样、絮状瘤骨形成,局部呈放射状,相应髓腔密度增高,周围可见软组织肿块影a~b:MPR 提示右动脉与肿块之间局部脂肪层消失,管腔狭窄,管壁毛糙。提示骨肉瘤毗邻动脉受侵;c~d:VR 图像可见右动脉受推移改变,右动脉发出多支小血管分布于肿瘤内;肿瘤表面可见多条杂乱增粗的小静脉,回流至股静脉内,股静脉提前显影。该病例经手术证实为右股骨远端骨肉瘤毗邻动脉受侵,遂于全麻下行右股骨远端骨肉瘤经髋关节离断术Fig.1 Popliteal artery invasion was suspected in a 15-year-old male patient with malignent tumors in the right distal femur based on MRI. Osteosarcoma was confrmed according to the pathological report after aspiration biopsy. The CTA examination showed cortical discontinuity in the inferior segment of the right femur and punched-out bone destruction with irregular and cotton-shaped osteoma around. A radical pattern was noticed locally and the density in the corresponding medullary cavity was increased, with a soft tissue mass shadow around a-b: Showed part of the fat layer disappeared between the right popliteal artery and the mass, with narrow lumen and rough wall based on MPR; c-d: Were VR images, which showed the right popliteal artery was changed by the push. There were a few small vessels in the tumor issued by the right popliteal artery. Some rough and widened small veins existed on the surface of the tumor, which fowed back to the femoral vein, and then an image of the femoral vein developed in advance. Popliteal artery invasion in the patient with osteosarcoma in the right distal femur was surgically confirmed. Hip disarticulation was performed under general anesthesia for osteosarcoma in the right distal femur
讨 论
尽管 MRI 被认为是对骨骼肌肉肿瘤进行分期的最佳影像学检查方法[1-3],但是其在显示肿瘤毗邻血管结构方面确有其局限性。Lang 等[4]认为 MRI无法使肿瘤与血管同时显示,除非将 MRA 融合到MRI 图像中。在轴位图像中由于血管倾斜走行所致部分容积效应,肿瘤与其毗邻血管之间的正常组织常常会显示不清。Meaney 等[6]认为早期静脉回流会导致 MRI 图像的解读困难,而且由于空间分辨率的限制,也使得一些小血管难以显示。此外,在常规 MRI 图像中,肿瘤的占位效应所致血管结构的变形和移位,也会影响对血管是否受侵的判读。尽管CTA 不是肿瘤分期常规的检查手段,但 CTA 有助于发现肿瘤内的骨化和钙化[7]并可有效评价骨质破坏[1-3,8]。CTA 作为非侵入性成像技术,可以显示肿瘤与其毗邻的主要血管的空间解剖关系、肿瘤的供血动脉以及血供情况,并可显示不同平面的详细血管结构。

图2 患者,男,60 岁,MRI 检查怀疑“右大腿内侧大收肌内肿物,右侧股深动脉受侵”,经穿刺活检,病理结果为少量梭形细胞组织呈肿瘤样增生,考虑纤维组织来源可能性大 a~b:为 CTA VR 重建,提示右侧大腿内侧大收肌内可见软组织肿块影,肿块与周围肌肉组织境界欠清晰,与右侧股骨皮质内侧关系密切,肿块大小约 13 cm × 8 cm × 6 cm,CTA 可见肿块内异常增粗迂曲肿瘤血管,可见右股深动脉及其分支 ( 旋股内动脉、旋股外动脉、穿动脉 ),进入肿块内部,可见右股静脉提前显影。未见肿块毗邻血管受侵征象。术中未见肿块毗邻血管受侵,遂行右大腿肿物扩大切除术,术后病理符合良性间叶瘤Fig.2 Tumors in the adductor magnus of the right medial thigh and deep artery invasion in the right femur were suspected in a 60-year-old male patient. Tumor-like proliferation was noticed in a few spindle cells according to the pathological report after aspiration biopsy. It might be caused by fibrous tissues a-b: were CTA VR reconstruction, which showed a soft tissue mass shadow in the adductor magnus of the right medial thigh. Unclear boundary was seen between the mass and surounding muscle tissues, which was closely connected with the medial contex of the right femur. The size of the mass was about 13 cm×8 cm×6 cm. The CTA examination showed seriouesly widened and tortuous tumor vessels in the mass and also the right deep artery and its bramches ( medial and lateral femoral circumfex arteries and perforating arteries ). An image of the right femoral vein developed in advance, and no signs of vascular invasion were noticed. No vascular invasion was surgically found. Tumorectomy was performed in the right thigh, and benign mesenchymoma was confrmed according to the postoerative pathological results
CTA 较超声多普勒、MRA、DSA 具有如下优势:( 1 ) 与超声多普勒相比,CTA 的三维展示更容易被临床医生接受;( 2 ) 与 MRA 相比,CTA 的费用更为低廉[9];( 3 ) CTA 噪声明显低于 MRA 而空间分辨率高于 MRA[10];( 4 ) 在进行 MRA 检查时,患者必须较长时间保持静止不动,这往往使一些因骨骼肌肉肿瘤疼痛的患者难以忍受[11];( 5 ) 血液在血管内缓慢流动导致的信号丢失会造成 MRA 的假性狭窄;( 6 ) 对于体内有金属植入物以及具有幽闭恐惧症的患者则只能选择 CTA 检查;( 7 ) 既往采用 DSA作为诊断四肢动脉狭窄及闭塞性病变的金标准,但由于 DSA 为有创检查,其使用受到了一定的限制,DSA 是通过观察由于肿块占位效应所致的血管的移位、狭窄、闭塞来判断血管是否受侵,并且仅可提供管腔内的信息而无法获取血管壁或血管腔以外信息;( 8 ) 尽管 DSA 具有较高的空间分辨率,但是无法单独依靠 DSA 发现先于狭窄与闭塞发生的动脉外膜的受侵;( 9 ) DSA 通过注入足量的对比剂以及多方位投照才能获取满意的影像,而 CTA 只需要一次扫描和一次注入对比剂,即可重复获得多平面的图像。基于多排螺旋 CT 容积扫描的特点,使得图像的各向同性成为可能,MDCTA 逐渐应用于临床,为患者术前评估及术后随访提供了安全、无创、可靠的新途径,其优势在于可提供高质量的多平面、三维、四维重建图像,从任意角度清晰观察狭窄病变、血管壁的情况并且可以通过侧支循环显示闭塞血管远端的血管,空间分辨率的提高可实现对小血管的显示,并且能够多方位立体显示血管与周围结构的空间关系。
不同的后处理技术对下肢病变的显示各有优势:( 1 ) 最大密度投影 ( MIP ) 显示血管清晰,对比度高,对股浅动脉,胫前、后动脉及腓动脉等中小血管的显示能力较强,其反转像类似于 DSA 像,可很好地显示下肢动脉的狭窄、闭塞及闭塞段侧支循环,丰富了图像细节;( 2 ) MPR 重建可获得下肢动脉冠状面、矢状面和任意角度斜面位的图像;( 3 )曲面重建 ( CPR ) 可清晰显示病变大小、范围及栓子,将感兴趣区血管全程展示在一幅图像上;( 4 )容积再现 ( VR ) 空间立体感强,能较好地显示血管和周围组织的关系,对展示重叠血管效果更佳,能显示血管壁广泛的不规则狭窄及节段性闭塞。
通过上述技术的多方位观察,可获得主要动、静脉及其一级分支的清晰图像,使得血管情况的判断更为准确,断层图像与 MIP、VR、MPR 相结合观察,可明确显示血管病变的部位、范围和程度,亦可直观显示肿瘤侵犯血管的范围以及侧支循环代偿情况[12]。
Li 等[13]对 13 例肢体骨肉瘤患者进行 MDCT检查,分别应用 CT 增强检查以及 CTA 评估肿瘤毗邻血管受侵情况,以手术所见为金标准,进行kappa 一致性检验,CT 增强检查敏感度为 100%,特异度为 83.3%,阳性预测值为 87.5%,阴性预测值为 100%,准确度 92.3%;CTA VR 检查敏感度为 71.4%,特异度为 100%,阳性预测值为 100%,阴性预测值为 75%,准确度为 84.6%。笔者认为,在临床实践中,放射科医生在利用影像工作站进行CTA 重建的过程,其实就是重建、观察、诊断同时进行的过程。本研究中,我们综合利用影像工作站血管分析软件,横断层血管图像与 MIP、VR、MPR相结合观察,以手术所见为金标准,经过统计学分析发现,MDCTA 评估肿瘤毗邻血管受侵的敏感性为100%,特异性为 80%,阳性预测值为 66.7%,阴性预测值为 100%,准确度为 85.7%。此外,本研究结果与 Feydy 等[14]报道相似,他们是使用 MRA 评估血管受侵情况,当肿瘤毗邻血管出现移位、狭窄、闭塞时即认为血管受侵,其敏感度、特异度、阳性预测值、阴性预测值和准确度分别为 82%,85%,75%,90%,84%。
需要指出的是,VR 在评价血管纵轴受累程度以及显示受累血管的完整性上具有优势。此外,一些肿瘤供血动脉的异常扩张也能够被发现,从而避免术中触碰一些由于血管扩张所致菲薄管壁而引起严重出血。肢体骨骼肌肉肿瘤患者术前进行 MDCTA检查,可准确显示肿瘤与其毗邻血管的空间解剖关系、肿瘤导致的血管狭窄受侵以及肿瘤供血动脉的来源和走行,有助于制订手术计划、设计手术方案。由于肢体骨骼肌肉肿瘤本身较为罕见,使得本研究的样本量较小,不足以比较不同类型肿瘤的影像学特点,这是本研究的不足之处。
总之,本研究结果提示,对于肢体骨骼肌肉肿瘤患者,如果 MRI 怀疑肿瘤毗邻血管受侵,MDCTA检查可以提供更为真实可靠的影像学信息,为制订手术计划提供有力的依据。
[1]Peabody TD, Gibbs CP Jr, Simon MA. Evaluation and staging of musculoskeletal neoplasms. J Bone Joint Surg Am, 1998, 80(8):1204-1218.
[2]Pettersson H, Gillespy T 3rd, Hamlin DJ, et al. Primary musculoskeletal tumors: examination with MR imaging compared with conventional modalities. Radiology, 1987, 164(1):237-241.
[3]Berquist TH. Magnetic resonance imaging of musculoskeletal neoplasms. Clin Orthop Relat Res, 1989, (244):101-118.
[4]Lang P, Grampp S, Vahlensieck M, et al. Primary bone tumors: value of MR angiography for preoperative planning and monitoring response to chemotherapy. AJR Am J Roentgenol, 1995, 165(1):135-142.
[5]Swan JS, Grist TM, Sproat IA, et al. Musculoskeletal neoplasms: preoperative evaluation with MR angiography. Radiology, 1995, 194(2):519-524.
[6]Meaney JF, Ridgway JP, Chakraverty S, et al. Stepping-table gadolinium-enhanced digital subtraction MR angiography of the aorta and lower extremity arteries: preliminary experience. Radiology, 1999, 211(1):59-67.
[7]Parsons TW 3rd, Frink SJ, Campbell SE. Musculoskeletal neoplasia: helping the orthopaedic surgeon establish the diagnosis. Semin Musculoskelet Radiol, 2007, 11(1):3-15.
[8]Ouwendijk R, Kock MC, Visser K, et al. Interobserver agreement for the interpretation of contrast-enhanced 3D MR angiography and MDCT angiography in peripheral arterial disease. AJR Am J Roentgenol, 2005, 185(5):1261-1267.
[9]Ouwendijk R, de Vries M, Stijnen T, et al. Multicenter randomized controlled trial of the costs and effects of noninvasive diagnostic imaging in patients with peripheral arterial disease: the DIPAD trial. AJR Am J Roentgenol, 2008, 190(5):1349-1357.
[10]Heijenbrok-Kal MH, Kock MC, Hunink MG. Lower extremity arterial disease: multidetector CT angiography meta-analysis. Radiology, 2007, 245(2):433-439.
[11]Ouwendijk R, de Vries M, Pattynama PM, et al. Imaging peripheral arterial disease: a randomized controlled trial comparing contrast-enhanced MR angiography and multidetector row CT angiography. Radiology, 2005, 236(3): 1094-1103.
[12]Willmann JK, Baumert B, Schertler T, et al. Aortoiliac and lower extremity arteries assessed with 16-detector row CT angiography: prospective comparison with digital subtraction angiography. Radiology, 2005, 236(3):1083-1093.
[13]Li Y, Zheng Y, Lin J, et al. Evaluation of the relationship between extremity soft tissue sarcomas and adjacent major vessels using contrast-enhanced multidetector CT and threedimensional volume-rendered CT angiography: a preliminary study. Acta Radiol, 2013, 54(8):966-972.
[14]Feydy A, Anract P, Tomeno B, et al. Assessment of vascular invasion by musculoskeletal tumors of the limbs: use of contrast-enhanced MR angiography. Radiology, 2006, 238(2): 611-621.
( 本文编辑:王萌 李贵存 )
Clinical signifcance of multi-slice spiral computerized tomography angiograph in the assessment of vascular invasion by musculoskeletal tumors of the limbs
LIU Gang, ZHANG Yi-jun. Department of Radiology, the first Affliated Hospital of the General Hospital of CPLA, Beijing, 100048, PRC
ObjectiveTo evaluate the effectiveness of multi-slice spiral computerized tomography angiograph ( MDCTA ) in determining vascular invasion in patients with musculoskeletal tumors, and to compare the results with the surgical fndings. MethodsFrom January 2008 to June 2014, 21 patients diagnosed musculoskeletal tumors with vascular invasion based on magnetic resonance imaging ( MRI ) underwent MDCTA examination before surgical treatment. Their clinical data were retrospecitvely analyzed, including 11 cases of limb bone tumors and 10 cases of limb soft tissue tumors. There were 12 males and 9 females, whose mean age was 33 years old. The doubleblind method was used to determine the presence of vascular invasion based on MDCTA examination results. The statistical analysis was carried out by using surgical fndings as the gold standard.ResultsTwelve patients without vascular invasion according to the MDCTA examination were also surgically negative ( true negative ). Among the 9 patients with vascular invasion shown by the MDCTA examination, only 3 patients had adhesions and were considered surgically negative ( false positive ). The other 6 patients had vascular invasion proven by surgery and were considered surgically positive ( true positive ). Based on the surgical fndings, the sensitivity of MDCTA was 100%, specifcity 80%, positive predictive value 66.7%, negative predictive value 100%, and accuracy 85.7%.ConclusionsMDCTA is an accurate imaging technique in evaluating vascular invasion of musculoskeletal tumors, which can provide valuable and authentic imaging information.
Tomography, spiral computed; Angiography; Bone neoplasms; Soft tissue neoplasms; Tumor infltrating
10.3969/j.issn.2095-252X.2014.11.006
R738.1, R445
100048 北京,解放军总医院第一附属医院放射科
张毅军,Email: 304a800@163.com
2014-08-14 )
猜你喜欢
企业界(2024年8期)2024-07-05 10:59:04
中华实用诊断与治疗杂志(2022年2期)2022-09-02 01:47:28
今日农业(2021年19期)2022-01-12 06:16:32
中老年保健(2021年5期)2021-12-02 15:48:21
环境保护与循环经济(2021年7期)2021-11-02 08:10:54
中老年保健(2021年5期)2021-08-24 07:06:28
国外核新闻(2020年8期)2020-03-14 02:09:19
中国生殖健康(2019年11期)2019-01-07 01:27:38
小布老虎(2017年1期)2017-07-18 10:57:27
肝胆胰外科杂志(2015年4期)2015-02-27 11:12:29
