结肠镜和组织病理学检查在炎症性肠病诊断中的价值
2012-10-22 12:10:34沈博
胃肠病学 2012年12期
沈 博
美国克利夫兰医学中心胃肠病学和肝病学系
炎症性肠病(IBD)主要包括克罗恩病(CD)和溃疡性结肠炎(UC)两种疾病,目前其诊断和治疗仍是难题。回肠结肠镜检查是该病最重要的诊断手段,主要用于明确诊断、鉴别诊断、癌变监控以及评估病灶范围、疾病活动度和治疗应答。
一、回肠结肠镜
结肠回肠镜能直接观察直肠、结肠和末端回肠,并可取黏膜行活检。除非有禁忌证,如暴发性结肠炎或中毒性巨结肠,否则对临床表现疑似IBD的患者均应行结肠镜检查,以充分观察整个直肠、结肠和末端回肠。由于磷酸钠[1,2]和非甾体消炎药(NSAIDs)[3]可能致肠黏膜损伤,使肠黏膜发生类似于IBD的组织学改变,因此在行结肠镜前应避免使用磷酸钠作为肠道准备以及服用NSAIDs。
多种肠道疾病的临床和内镜下表现与IBD类似,包括感染性肠炎、药物性肠炎、憩室结肠炎、缺血性结肠炎、器官移植后结肠炎、自身免疫性肠炎和放射性肠炎。组织病理学检查不仅能为鉴别IBD与非IBD疾病提供有价值的线索,而且对CD和UC亦有一定的鉴别价值。这是因为一旦开始治疗后,原本的病灶分布会发生改变,变得不典型,如UC原本弥漫分布的病灶可能变成片状分布,甚至发生直肠未受累的情况,而这类型的病灶原本在CD中更常见[4,5]。在一项包含 39 例 UC 患者的临床研究[5]中,经局部或系统治疗后,内镜下44%的患者病灶呈片状分布,13%直肠未受累;33%的患者组织学可见片状病灶,15%组织学未受累。行结肠镜检查时,应特别注意肛门和肛周病变,如脓肿、线状裂隙、瘘管和大皮赘(“象耳”状),上述病变多见于CD。CD最典型的内镜下特征表现为病灶呈节段性分布(如斑片状病灶)、直肠未受累、累及末端回肠和回盲瓣、肛门和肛周病灶,可与UC进行鉴别。内镜下阿弗他溃疡、非连续性溃疡、匐行性溃疡和黏膜呈鹅卵石样改变亦可提示CD,但需指出的是,上述特征性改变对诊断CD和UC缺乏特异性。
回肠镜对鉴别回肠末端的炎症为CD回肠炎还是倒灌性回肠炎具有重要意义。倒灌性回肠炎在活动性UC中所占的比例约为10%,尤其是并发原发性硬化性胆管炎(PSC)的患者[6]。倒灌性回肠炎的内镜和组织学表现与弥漫性右半结肠炎十分相似,其回盲瓣常保持开放状态,呈“鱼嘴”样(见图1)。而CD回肠炎的主要特征为非连续性溃疡、末端回肠或回盲瓣变形和狭窄[6~8]。
远端型UC可能会逐渐向近端发展[9]。阑尾孔周围的炎症称为“斑片状盲肠炎”或“斑片状阑尾周围炎”,常并发左半结肠炎而右半结肠正常,应避免与 CD 混淆[10,11]。
结肠镜结合其他检查可有效鉴别CD与UC,准确率≥85%[12]。一项对350例IBD患者随访超过22个月的前瞻性研究[13]发现,结肠镜结合黏膜活检能准确鉴别89%的CD与UC,4%的患者排除了IBD的诊断,7%诊断为未定型结肠炎。但目前对未定型结肠炎的诊断标准尚未达成共识。
二、组织病理学的诊断和鉴别诊断价值
黏膜活检对诊断和鉴别诊断疑似IBD患者十分重要。虽然目前尚缺乏能明确诊断UC或CD的病理学标准,但黏膜组织病理学评估仍是诊断和鉴别诊断IBD的首要步骤。结肠镜检查的进镜深度应达回肠末端,回肠末端和直肠必须取活检,右半结肠和左半结肠亦应取活检。对病灶和病灶周围看似正常的组织,均应取活检。不同部位的活检标本应分瓶标记,这是因为即使是正常黏膜,不同肠段,如结肠与直肠、左半结肠与右半结肠的组织学表现并不相同。Paneth细胞是特殊分化的小肠细胞,但在部分正常人中可出现于右半结肠,而左半结肠和(或)直肠黏膜中的 Paneth细胞则提示为IBD所致的慢性黏膜损伤。需指出的是,内镜下炎症的严重程度与组织学表现可能并不平行。组织学检查示黏膜慢性炎症改变的患者,内镜下可表现为正常黏膜,反之亦然。
各种急性或活动性炎症的组织学表现,如嗜中性或嗜酸性粒细胞浸润、内镜下糜烂和溃疡均缺乏特异性,仅反映炎症的严重程度,对诊断IBD无特殊价值。“局灶性活动性炎症”是个令人费解的组织学术语,“局灶性”的描述常被误解为CD的“节段性”或“斑片状”病灶。局灶性活动性炎症常因服用NSAIDs、感染或使用磷酸钠行肠道准备所致。
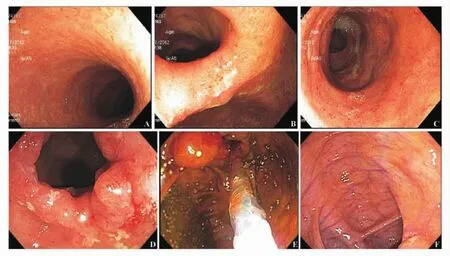
图1 UC倒灌性回肠炎与CD回肠炎的区别
目前认为组织学缺乏慢性非特异性炎症,就不能作出IBD的诊断。这是因为IBD的诊断一旦确立就是终身的。慢性炎症的组织学特征性改变包括隐窝结构扭曲变形、基底层淋巴细胞增多、绒毛钝化、细胞固有层单核细胞聚集、幽门腺化生、Paneth细胞化生和黏膜肌层增生[14~16]。非干酪样肉芽肿提示CD,但内镜标本中肉芽肿的检出率仅为15% ~36%[17]。溃疡和阿弗他糜烂边缘取活检能提高肉芽肿的检出率[18]。肉芽肿对诊断CD缺乏特异性,其还可见于肠结核、真菌和细菌感染、改道性结肠炎、结节病[19]和排异反应(主要发生于肠切除术后的缝线处)。对新诊断的CD,尤其是病灶位于末端回肠处,推荐采用AFB染色或黏膜样本PCR法排除肠结核。在慢性肠炎患者中(无论是否为IBD),肠黏膜上皮破坏(特别是杯状细胞)可导致黏蛋白样物质溢出,导致黏液性肉芽肿或异物肉芽肿。
黏膜活检有助于发现结肠炎症,并可对炎症的范围和程度进行分级。炎症范围可分级为直肠炎、左半结肠炎(炎症自下向上发展到脾区)和广泛性结肠炎(从近端发展到脾区)。结肠镜下炎症严重程度与和组织学结果并没有相关性。与组织学检查相比,结肠镜观察常会低估IBD的严重程度[20],尤其是处于治疗中的患者。炎症范围(广泛性肠炎、左半结肠炎或直肠炎)的评判更应依赖组织学诊断,而非内镜检查[20,21]。
组织学检查对评估难治性IBD患者和应用免疫抑制剂患者的巨细胞病毒和EB病毒重复感染具有十分重要的意义。在三级医疗机构中,已常规开展应用免疫组化判断巨细胞病毒感染和染色体原位杂交诊断EB病毒感染的工作。
黏膜活检的主要缺点是无法评价CD透壁性肠炎。手术可获取理想的肠壁全层病理学标本,但具有创伤性,使其临床应用受到局限。此外,重度UC患者可发生淋巴细胞聚集的透壁性肠炎,尤其是在深溃疡区域,病理医师常将其诊断为未定型结肠炎。
三、结肠镜监控疾病活动度
内镜下UC直肠炎或左半结肠炎的发生率约为1/3 ~1/2[22,23],随着病程的延长(如病程 > 20 ~30年),全结肠炎的病变范围会逐渐缩小[22]。
结肠镜能客观评估IBD的疾病活动度,与此相反,主观症状并不能准确判断疾病的严重程度。此外,症状评分与内镜下炎症程度的相关性以及临床缓解与黏膜愈合的相关性均较弱[24]。结肠镜检查有助于指导药物治疗和判断是否需手术干预[25,26]。目前有不少基于临床表现和(或)内镜检查结果的疾病活动性评分系统[26~29]。结肠镜检查常用于判断免疫抑制剂和生物制剂抗肿瘤坏死因子治疗IBD的疗效[30,31]。在最近的一些药物临床研究[32,33]中,应用结肠镜判断黏膜愈合情况已成为评估IBD结局的重要指标,黏膜愈合预示疾病复发和日后需外科手术的可能性较低。
四、异型增生的监控
病程长、受累肠段广泛的IBD患者发展为异型增生甚至结直肠癌(CRC)的危险性明显增高。CRC风险与长期病程、广泛重度UC病变范围、CRC家族史、发病年龄、倒灌性回肠炎以及并发PSC呈正相关[34~37]。超过1/3全结肠受累的 CD患者的 CRC风险亦升高[38,39]。受累肠段范围的评估需由内镜检查和病理学检查共同完成[40]。一项UC的病例对照研究[41]发现,长期结肠镜随访可明显降低CRC的死亡率。
病变范围广泛的IBD患者在发病8~10年后应每1~2年复查一次结肠镜,而对伴有PSC者,UC确诊时应即刻定期复查结肠镜。确诊为全结肠炎的患者,应从盲肠至直肠每隔10 cm行4象限活检,至少取33块标本[40]。活检标本应包括狭窄、大面积病变、肉眼可见的异常,而不必包括假息肉[42,43]。由于分级的一致性较差,对异型增生的诊断需2名病理专家确认,特别是低级别异型增生[40]。如平坦型黏膜中发现高级别异型增生或多灶性低级别异型增生,应考虑结肠切除术。单发病灶的低级别异型增生是否需手术目前尚存争议。对腺瘤样息肉,应采用息肉切除术彻底切除,并对邻近黏膜取活检判断是否存在异型增生。如非炎症活动区发现一个异型增生性息肉,且邻近黏膜无异型增生,则按照非IBD的散发性息肉进行处理。如异型增生性息肉发生在活动性炎症区(发育不良相关性损害和团块)且息肉多为扁平型、邻近黏膜可见异型增生,但又不适合采用内镜下息肉切除术治疗,则应行结肠切除术[34~36,44~46]。如在活动性炎症区发现一个边界清晰且适合行内镜下切除的息肉,病灶彻底切除后应取邻近黏膜行活检,标本应单独保存[47]。
五、总结和结论
IBD患者应常规行回肠结肠镜检查,可评估病情并鉴别UC与CD。回肠结肠镜可为评估病变范围和程度提供有价值的信息。黏膜活检同样有非常重要的诊断价值,并可鉴别CD和UC。CD和UC的组织学特征均可表现为慢性炎症。如内镜下结肠炎或末端回肠炎未表现出相应的组织学慢性改变,则确诊IBD存在一定难度。病程长、范围广的IBD发生异型增生的概率明显增高,定期接受结肠镜检查监控病情十分必要。
1 Zwas FR,Cirillo NW,el-Serag HB,et al.Colonic mucosal abnormalities associated with oral sodium phosphate solution[J].Gastrointest Endosc,1996,43(5):463-466.
2 Rejchrt S,Bures J,Siroký M,et al.A prospective,observationalstudy ofcolonic mucosalabnormalities associated with orally administered sodium phosphate for colon cleansing before colonoscopy[J]. Gastrointest Endosc,2004,59(6):651-654.
3 Lengeling RW,Mitros FA,Brennan JA,et al.Ulcerative ileitis encountered atileo-colonoscopy:likely role of nonsteroidal agents[J].Clin Gastroenterol Hepatol,2003,1(3):160-169
4 Kim B,Barnett JL,Kleer CG,et al.Endoscopic and histological patchiness in treated ulcerative colitis[J].Am J Gastroenterol,1999,94(11):3258-3262.
5 Bernstein CN,Shanahan F,Anton PA,et al.Patchiness of mucosal inflammation in treated ulcerative colitis:a prospective study[J].Gastrointest Endosc,1995,42(3):232-237.
6 Chutkan RK,Wayne JD.Endoscopy in inflammatory bowel disease.In:Kirsner JB,ed.Inflammatory bowel disease[M].5th ed.Philadelphia:Saunders Baltimore:Williams and Wilkins,2000:453-477.
7 Moum B,Ekbom A,Vatn MH,et al.Change in the extent of colonoscopic and histological involvement in ulcerative colitis over time[J].Am J Gastroenterol,1999,94(6):1564-1569.
8 Rutgeerts P.Strategies in the prevention of post-operative recurrence in Crohn’s disease[J].Best Pract Res Clin Gastroenterol,2003,17(1):63-73.
9 Geboes K,Ectors N,D’Haens G,et al.Is ileoscopy with biopsy worthwhile in patients presenting with symptoms of inflammatory bowel disease[J]?Am J Gastroenterol,1998,93(2):201-206.
10 Okawa K,Aoki T,Sano K,et al.Ulcerative colitis with skip lesions at the mouth of the appendix:a clinical study[J].Am J Gastroenterol,1998,93(12):2405-2410.
11 Byeon JS,Yang SK,Myung SJ,et al.Clinical course of distal ulcerative colitis in relation to appendiceal orifice inflammation status[J].Inflamm Bowel Dis,2005,11(4):366-371.
12 Chutkan RK,Scherl E,Waye JD.Colonoscopy in inflammatory bowel disease[J].Gastrointest Endosc Clin N Am,2002,12(3):463-483.
13 Pera A,Bellando P,Caldera D,et al.Colonoscopy in inflammatoryboweldisease. Diagnostic accuracy and proposal of an endoscopic score[J].Gastroenterology,1987,92(1):181-185.
14 Surawicz CM,Belic L.Rectal biopsy helps to distinguish acute self-limited colitis from idiopathic inflammatory bowel disease[J].Gastroenterology,1984,86(1):104-113.
15 Dundas SA,Dutton J,Skipworth P.Reliability of rectal biopsy in distinguishing between chronic inflammatory bowel disease and acute self-limiting colitis[J].Histopathology,1997,31(1):60-66.
16 Tanaka M,Saito H,Kusumi T,et al.Spatial distribution and histogenesis of colorectal Paneth cell metaplasia in idiopathic inflammatory bowel disease[J].J Gastroenterol Hepatol,2001,16(12):1353-1359.
17 Ramzan NN,Leighton JA,Heigh RI,et al.Clinical significance of granuloma in Crohn’s disease[J].Inflamm Bowel Dis,2002,8(3):168-173.
18 Pötzi R,Walgram M,Lochs H,et al.Diagnostic significance of endoscopic biopsy in Crohn’s disease[J].Endoscopy,1989,21(2):60-62.
19 Sands BE.From symptom to diagnosis:clinical distinctions amongvariousformsofintestinalinflammation[J].Gastroenterology,2004,126(6):1518-1532.
20 Kiesslich R,Fritsch J,Holtmann M,et al.Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis[J].Gastroenterology,2003,124(4):880-888.
21 Florén CH,Benoni C,Willén R.Histologic and colonoscopic assessment of disease extension in ulcerative colitis[J].Scand J Gastroenterol,1987,22(4):459-462.
22 Meucci G,Vecchi M,Astegiano M,et al.The natural history of ulcerative proctitis:a multicenter,retrospective study.Gruppo di Studio per le Malattie Infiammatorie Intestinali(GSMII)[J].Am J Gastroenterol,2000,95(2):469-473.
23 Langholz E,Munkholm P,Davidsen M,et al.Changes in extent of ulcerative colitis:a study on the course and prognostic factors[J].Scand J Gastroenterol,1996,31(3):260-266.
24 Landi B,Anh TN,Cortot A,et al.Endoscopic monitoring of Crohn’s disease treatment:a prospective,randomized clinical trial.The Groupe d’Etudes Therapeutiques des Affections Inflammatoires Digestives[J].Gastroenterology,1992,102(5):1647-1653.
25 Carbonnel F,Lavergne A,Lémann M,et al.Colonoscopy of acute colitis.A safe and reliable tool for assessment of severity[J].Dig Dis Sci,1994,39(7):1550-1557.
26 Mary JY,Modigliani R.Development and validation of an endoscopic index of the severity for Crohn’s disease:a prospective multicentre study. Groupe d’Etudes Thérapeutiques desAffectionsInflammatoiresdu Tube Digestif(GETAID)[J].Gut,1989,30(7):983-989.
27 Ferguson A.Assessment and management of ulcerative colitis in children[J].Eur J Gastroenterol Hepatol,1997,9(9):858-863.
28 Geboes K,Dalle I.Influence of treatment on morphological features of mucosal inflammation[J].Gut,2002,50 Suppl 3:Ⅲ37-Ⅲ42.
29 Samuel S,Bruining DH,Loftus EV Jr,et al.Validation of the ulcerative colitis colonoscopic index of severity and its correlation with disease activity measures [J]. Clin Gastroenterol Hepatol,2012 [Epub ahead of print].
30 D’haens G,Van Deventer S,Van Hogezand R,et al.Endoscopic and histological healing with infliximab antitumor necrosis factor antibodies in Crohn’s disease:A European multicenter trial[J].Gastroenterology,1999,116(5):1029-1034.
31 D’Haens G,Geboes K,Rutgeerts P.Endoscopic and histologic healing of Crohn’s(ileo-)colitis with azathioprine[J].Gastrointest Endosc,1999,50(5):667-671.
32 Rutgeerts P,Sandborn WJ,Feagan BG,et al.Infliximab for induction and maintenance therapy for ulcerative colitis[J].N Engl J Med,2005,353(23):2462-2476.
33 D’Haens G,Geboes K,Ponette E,et al.Healing of severe recurrent ileitis with azathioprine therapy in patients with Crohn’s disease[J].Gastroenterology,1997,112(5):1475-1481.
34 Eaden JA,Abrams KR,Mayberry JF.The risk of colorectal cancer in ulcerative colitis:a meta-analysis[J].Gut,2001,48(4):526-535.
35 Prior P,Gyde SN,Macartney JC,et al.Cancer morbidity in ulcerative colitis[J].Gut,1982,23(6):490-497.
36 Kornfeld D,Ekbom A,Ihre T.Is there an excess risk for colorectal cancer in patients with ulcerative colitis and concomitant primary sclerosing cholangitis?A population based study[J].Gut,1997,41(4):522-525.
37 Lindberg BU,Broomé U,Persson B.Proximal colorectal dysplasia or cancer in ulcerative colitis.The impact of primary sclerosing cholangitis and sulfasalazine:results from a 20-year surveillance study[J].Dis Colon Rectum,2001,44(1):77-85.
38 Bernstein CN,Blanchard JF,Kliewer E,et al.Cancer risk in patients with inflammatory bowel disease:a populationbased study[J].Cancer,2001,91(4):854-862.
39 Friedman S,Rubin PH,Bodian C,et al.Screening and surveillance colonoscopy in chronic Crohn’s colitis[J].Gastroenterology,2001,120(4):820-826.
40 Itzkowitz SH,Present DH;Crohn’s and Colitis Foundation of America Colon Cancer in IBD Study Group.Consensus conference:Colorectal cancer screening and surveillance in inflammatory bowel disease[J].Inflamm Bowel Dis,2005,11(3):314-321.
41 Choi PM,Nugent FW,Schoetz DJ Jr,et al.Colonoscopic surveillance reduces mortality from colorectal cancer in ulcerative colitis[J].Gastroenterology,1993,105(2):418-424.
42 Eaden JA,Mayberry JF;British Society for Gastroenterology;Association of Coloproctology for Great Britain and Ireland.Guidelines for screening and surveillance of asymptomatic colorectalcancerin patientswith inflammatory bowel disease[J].Gut,2002,51 Suppl 5:Ⅴ10-Ⅴ12.
43 Rutter MD,Saunders BP,Wilkinson KH,et al.Most dysplasia in ulcerative colitis is visible at colonoscopy[J].Gastrointest Endosc,2004,60(3):334-339.
44 Eaden J,Abrams K,Ekbom A,et al.Colorectal cancer prevention in ulcerative colitis:a case-control study[J].Aliment Pharmacol Ther,2000,14(2):145-153.
45 Rutter M,Saunders B,Wilkinson K,et al.Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis[J].Gastroenterology,2004,126(2):451-459.
46 Heuschen UA,Hinz U,Allemeyer EH,et al.Backwash ileitis is strongly associated with colorectal carcinoma in ulcerative colitis[J].Gastroenterology,2001,120(4):841-847.
47 Odze RD,Farraye FA,Hecht JL,et al.Long-term followup after polypectomy treatment for adenoma-like dysplastic lesions in ulcerative colitis[J].Clin Gastroenterol Hepatol,2004,2(7):534-541.
猜你喜欢
现代实用医学(2022年10期)2022-12-08 05:50:00
现代畜牧科技(2021年9期)2021-10-13 06:39:10
肝博士(2021年1期)2021-03-29 02:32:08
中国医药指南(2017年3期)2017-11-13 02:55:23
中国内镜杂志(2017年2期)2017-03-20 16:18:08
中国民族医药杂志(2016年2期)2016-05-14 07:11:57
中国民族医药杂志(2016年5期)2016-05-09 07:43:45
成都中医药大学学报(教育科学版)(2016年1期)2016-01-22 07:24:50
实用肝脏病杂志(2015年5期)2015-12-03 06:28:04
国际消化病杂志(2015年5期)2015-02-27 12:11:10