冠心病病人PCI术后1年出血危险因素的模型构建和验证
2024-12-31 00:00:00宋利华付继京王俊伟
护理研究 2024年19期


Construction and validation of risk factors model related to hemorrhage in patients with coronary heart disease after PCI 1 year
Abstract" Objective:Based on LASSO⁃Logistic regression analysis of hemorrhage related factors in patients with coronary atherosclerotic heart disease(CHD) 1 year after percutaneous coronary intervention(PCI),and to establish a Nomogram prediction model for timely and effective clinical intervention.Methods:226 patients with coronary heart disease who underwent PCI in our hospital from January to December 2021 were selected as the study objects,and were divided into hemorrhage group and non⁃hemorrhage group according to whether they had hemorrhage one year after PCI.LASSO⁃Logistic regression was used to screen the risk factors of hemorrhage 1 year after PCI,and further construct a Nomogram prediction model.Receiver operating characteristic(ROC) curve and calibration curve were used to verify the value of Nomogram prediction model.Results:One year after PCI,the incidence of hemorrhage in 226 patients with coronary heart disease was 11.95%.Age≥60 years old,gastrointestinal history,chronic renal insufficiency,use of vessel closure,balloon dilation times,PARIS score,precision⁃DAPT score were the risk factors for bleeding 1 year after PCI(Plt;0.05).The Nomogram prediction model predicted the AUC of hemorrhage at 1 year after PCI to be 0.959.Conclusion:Age ≥60 years,history of digestive tract,chronic renal insufficiency,use of vessel closure,balloon dilation times,PARIS score and precision⁃DAPT score are risk factors for hemorrhage 1 year after PCI in patients with coronary heart disease.The establishment of a Nomogram prediction model based on LASSO⁃Logistic regression analysis has a certain value in predicting hemorrhage 1 year after PCI.Clinical screening and strict observation of high-risk groups should be carried out,and reasonable treatment measures should be formulated to reduce the risk of hemorrhage.
Keywords" coronary atherosclerotic heart disease; percutaneous coronary intervention,PCI; LASSO⁃Logistic regression; bleeding; Nomogram model; risk factors; forecast
摘要" 目的:基于LASSO⁃Logistic回归分析冠心病病人经皮冠状动脉介入(PCI)术后1年出血的危险因素,并建立Nomogram预测模型,以便临床采取及时、有效的干预方案。方法:选取2021年1月—12月在我院行PCI术的226例冠心病病人为研究对象,依据PCI术后1年是否出血分为出血组、未出血组。采用LASSO⁃Logistic回归筛选PCI术后1年出血的危险因素,进一步构建Nomogram预测模型。利用受试者工作特征(ROC)曲线、校准曲线验证Nomogram预测模型的价值。结果:PCI术后1年226例冠心病病人出血发生率为11.95%;年龄≥60岁、有消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、支架术后抗血小板药物停药模式(PARIS)评分、支架术后双重抗血小板治疗病人出血并发症预测(PRECISE⁃DAPT)评分为PCI术后1年出血的危险因素(Plt;0.05);Nomogram预测模型预测PCI术后1年出血的ROC曲线下面积为0.959。结论:年龄≥60岁、有消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分为冠心病病人PCI术后1年出血的危险因素,基于LASSO⁃Logistic回归分析建立的Nomogram预测模型对PCI术后1年出血具有一定预测价值,临床应筛查高危人群并实施严格观察,制定合理治疗措施,以降低出血风险。
关键词" 冠心病;经皮冠状动脉介入术;LASSO⁃Logistic回归;出血;Nomogram模型;危险因素;预测
doi:10.12102/j.issn.1009-6493.2024.19.004
冠心病是由冠状动脉粥样硬化性病变所致管腔狭窄的一种缺血性心脏病,经皮冠状动脉介入(PCI)术治疗后常采用双联抗血小板药物治疗(DAPT),以预防血栓形成[1⁃2]。DAPT治疗时存在出血风险,还可影响临床医师诊疗方案的制定,影响病人预后[3⁃4]。因而在PCI术前评估病人出血风险具有重要意义。随着机器学习能力成熟化,基于机器学习算法可建立预测PCI术后出血的预测模型,Nomogram模型属于可视化平面模型,是基于多因素回归分析结果并将其由互不相交线段展示在同一平面上,可整合不同变量生成直观评分系统,已被用于早期识别疾病发生风险、预测临床结局[5⁃6]。目前,针对冠心病病人PCI术后出血的评分系统尚未明确,基于此,本研究采用LASSO⁃Logistic回归分析冠心病病人PCI术后1年出血的危险因素,并建立Nomogram预测模型,进一步验证该模型对PCI术后1年出血的预测价值,为临床制定干预措施提供参考。
1" 资料与方法
1.1 一般资料
回顾性研究2021年1月—12月于本院行PCI术的冠心病病人。纳入标准:1)符合冠心病诊断标准[7];2)入院时未合并消化道出血、胃底静脉曲张者;3)既往无心外科手术治疗者。排除标准:1)伴有严重精神疾病者;2)近3个月内有接受外科手术计划者;3)合并血液系统疾病或恶性肿瘤者;4)合并心脏器质性疾病、代谢性疾病者;5)无法正常沟通交流者;6)术前伴有严重神经损伤者、心脏恶病质者;7)有出血倾向者。本研究经本院伦理委员会批准,审批号:〔2020〕伦审第(00131)号。
1.2 研究方法
1.2.1 治疗方法及分组
术前予以阿司匹林肠溶片、氯吡格雷负荷量,局部麻醉后行PCI术治疗,采用Seldinger法进行桡动脉穿刺,置入鞘管,回抽鞘管内血液、气泡,并注入肝素盐水封管[9]。术后以电话、门诊随访1年,统计随访期间出血情况。出血标准:依据出血时间分类,出血学术研究会(BARC)分型≥2型定义为出血事件[10⁃11]。根据病人PCI术后1年是否出血,将其分为出血组、未出血组。
1.2.2 临床资料的收集
通过调取研究对象电子病历收集临床资料,其中病变血管包括左前降支(LAD)、左回旋支(LCX)、右冠状动脉(RCA)、左主干(LM),用药情况包括阿司匹林和氯吡格雷、他汀类药物、β受体阻滞剂、血管紧张素转换酶抑制剂(ACEI)/血管紧张素受体拮抗剂(ARB)、钙离子通道阻滞剂(CCB)。
1.2.3 相关定义
支架置入术后抗血小板药物停药模式(PARIS)[12]:包括年龄、体质指数、目前吸烟、贫血、肌酐清除率、出院时三联抗栓治疗,其中年龄lt;50岁计0分,50~59岁计1分,gt;59~69岁计2分,gt;69~79岁计3分,gt;79岁计4分;体质指数lt;25 kg/m2或≥35 kg/m2计2分,25~lt;35 kg/m2计0分;吸烟计2分,不吸烟计0分;贫血计3分,无贫血计0分;肌酐清除率lt;60 mL/min计2分,≥60 mL/min计0分;出院时接受三联抗栓治疗计2分,未接受计0分。支架置入术后双重抗血小板治疗病人出血并发症预测评分(PRECISE⁃DAPT)[13]≥25分则采用短期DAPT治疗(3~6个月),lt;25分则采用长期DAPT治疗(12~24个月)。
1.3 统计学分析
采用SPSS 26.0软件分析数据,运用K⁃W检验分析连续变量正态性,组间差异采用Student⁃t检验进行检验,符合正态分布的定量资料以均数±标准差(x±s)表示;分类变量间差异采用检验及Fisher确切概率法,定性资料以例数、百分比(%)表示;采用R 3.6.3软件中glmnet对PCI术后1年出血的潜在危险因素进行LASSO回归分析;符合条件的变量纳入多因素Logistic回归分析,确定最优预测变量并计算比值比(OR);采用R 3.6.3软件建立并输出PCI术后1年出血的个体化Nomogram预测模型,绘制受试者工作特征(ROC)曲线并计算曲线下面积(AUC),采用Z检验评价Nomogram预测模型区分度即准确性;采用Hosmer⁃Lemeshow拟合优度检验、校准曲线评价Nomogram预测模型拟合优度、模型一致性,以Plt;0.05为差异有统计学意义。
2" 结果
2.1 冠心病病人一般资料
226例冠心病病人中,男124例、女102例,年龄52~80(69.32±3.02)岁,体质指数20~27(23.25±1.03)kg/m2,有吸烟史55例,有饮酒史45例,慢性肾功能不全31例,合并症:糖尿病22例,高脂血症65例;既往病史:冠心病家族史21例,脑卒中史5例,消化道病史47例。PCI术后1年,226例冠心病病人中27例发生出血,出血发生率为11.95%,其中消化道出血者14例,皮肤黏膜出血者8例,泌尿系统出血者3例,颅内出血者2例。
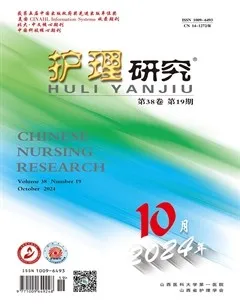
2.2 冠心病病人PCI术后1年出血危险因素的单因素分析
依据病人PCI术后1年是否出血分为出血组(n=27)、未出血组(n=199),单因素分析结果显示,两组年龄、合并高血压、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分比较,差异有统计学意义(Plt;0.05),详见表1。
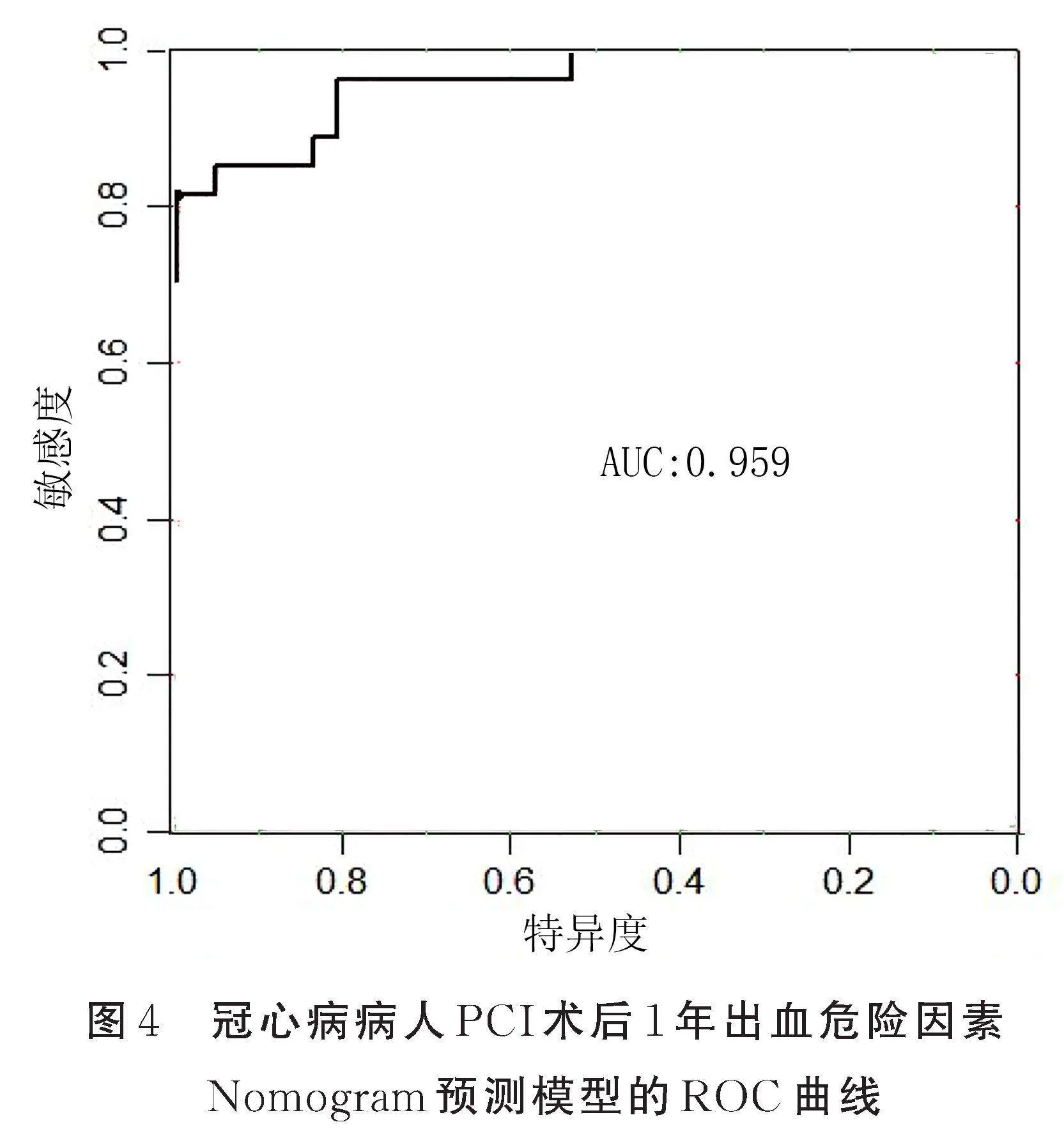
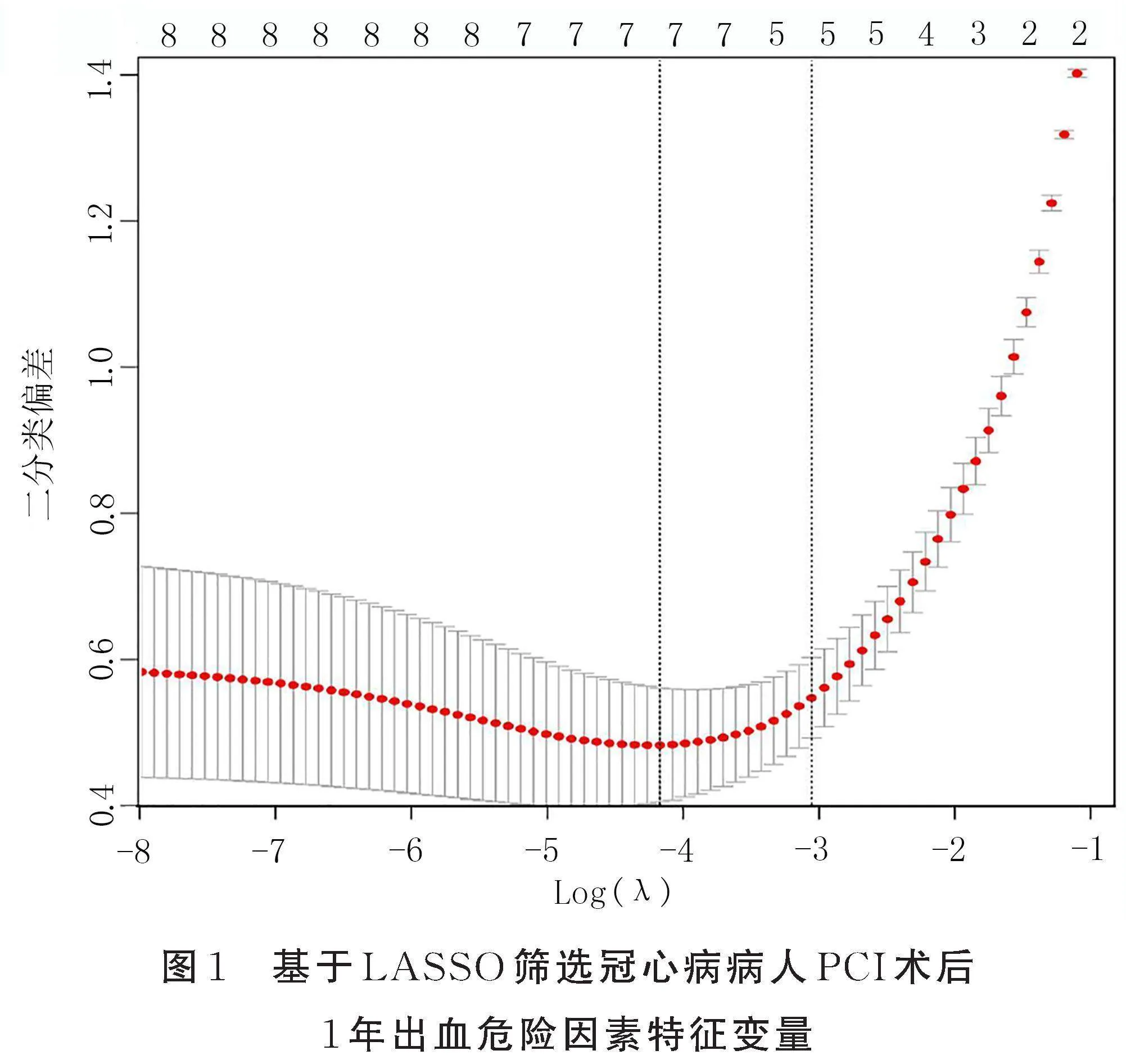
2.3 LASSO回归筛选预测模型因子
结合临床信息,利用R软件中glmnet进行LASSO回归,初始设置Lambda迭代为100次,误差最小时迭代次数为96次,Lambda值为0.015,所对应影响因素数量为7个,分别为年龄、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分。详见图1、图2。
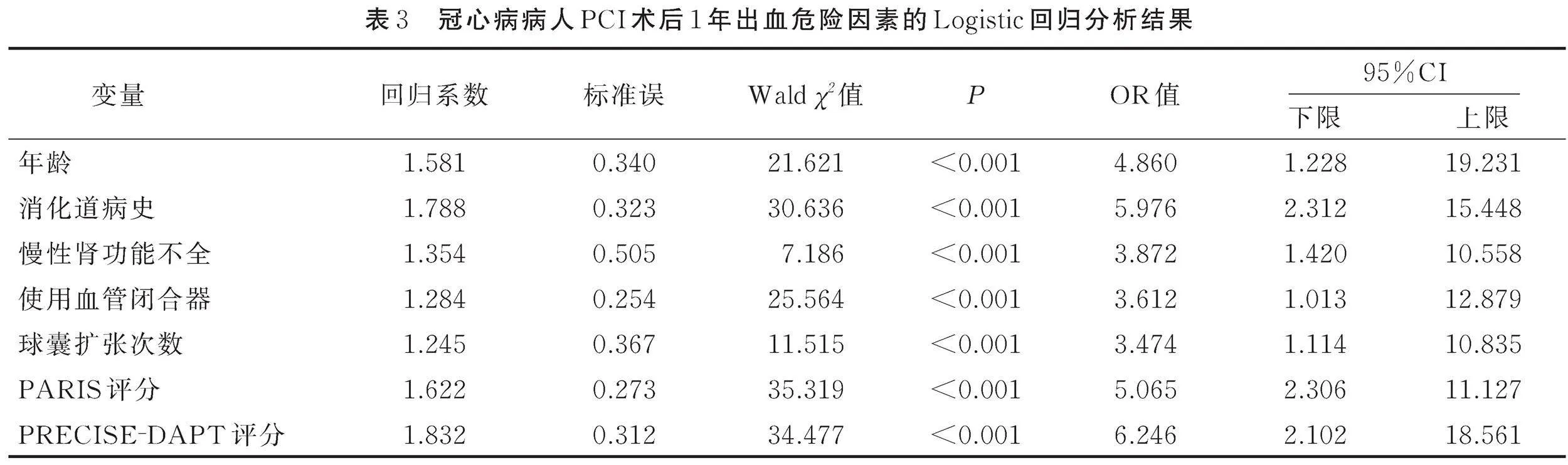
2.4 冠心病病人PCI术后1年出血危险因素的Logistic回归分析
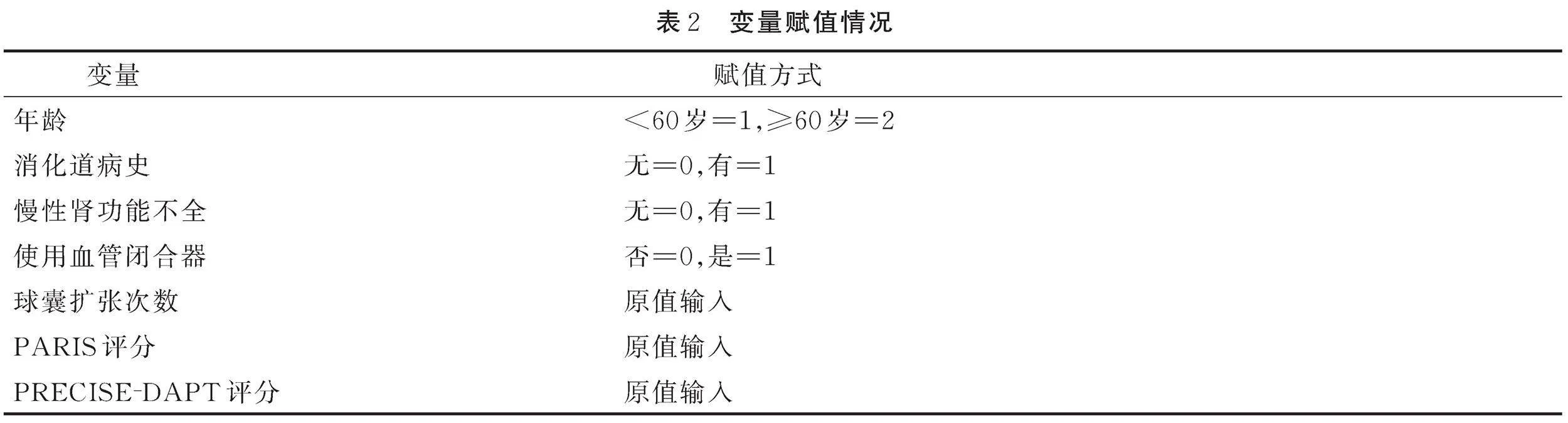
Logistic回归分析显示,年龄≥60岁、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分是冠心病病人PCI术后1年出血的危险因素(Plt;0.05),详见表2、表3。
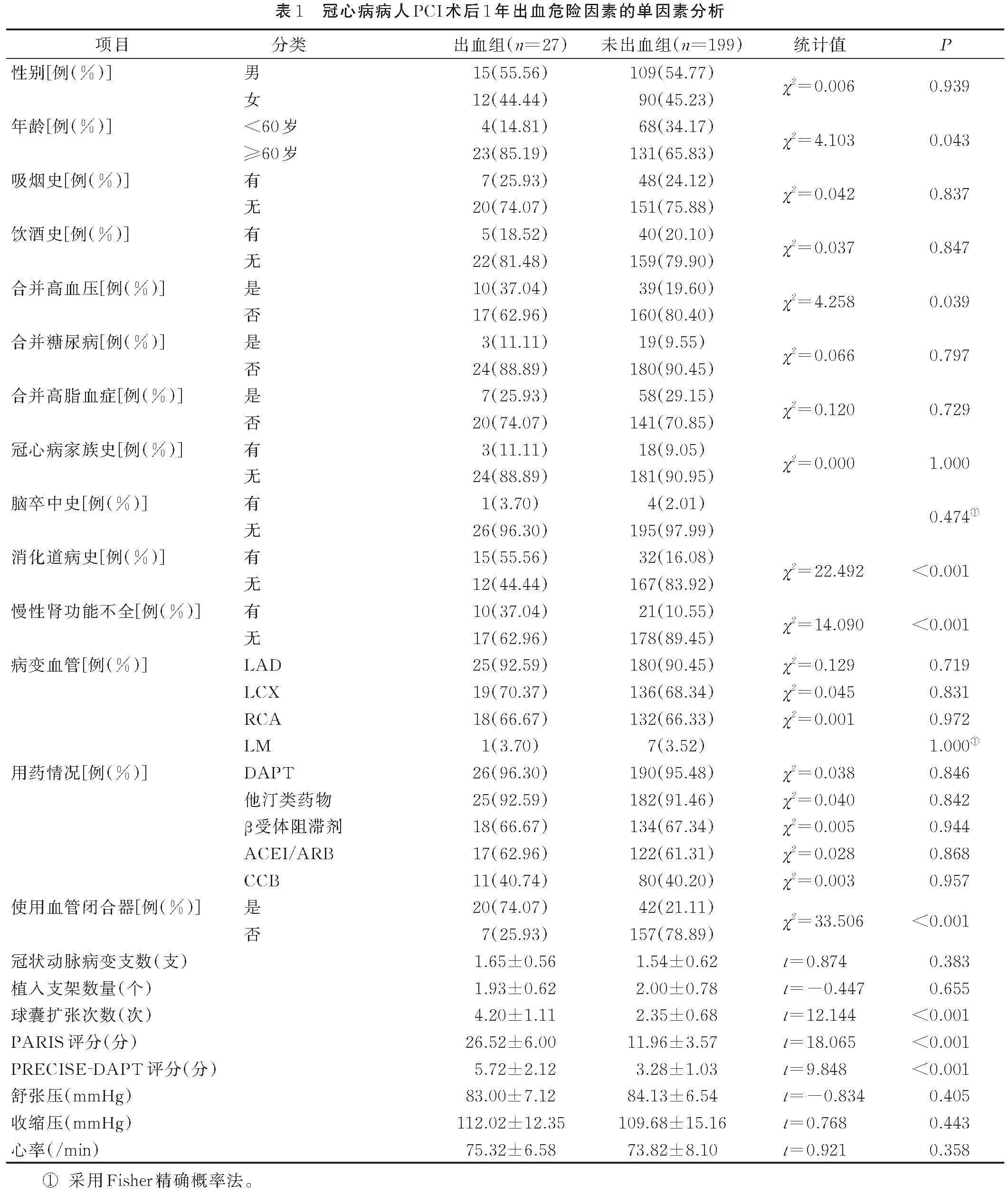
2.5 冠心病病人PCI术后1年出血危险因素预测模型的构建及验证
将Logistic回归方程筛选出的影响因素(年龄≥60岁、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分)纳入Nomogram预测模型,采用R 3.6.3软件建立并输出PCI术后1年出血的个体化Nomogram预测模型,见图3。绘制Nomogram预测模型预测冠心病病人PCI术后1年出血的ROC曲线,结果显示,此模型预测冠心病病人PCI术后1年出血的曲线下面积(AUC)为0.959,预测敏感度、特异度分别为99.50%、81.56%,见图4。对PCI术后1年出血的Nomogram预测模型进行评价和验证,设置因变量为PCI术后1年出血组和PCI术后1年未出血组,自变量为构建Nomogram预测模型风险总分进行校准曲线分析,结果显示,该校准曲线与理想曲线拟合较好,Hosmer⁃Lemeshow拟合优度检验χ2=8.728,P=0.536,表示Nomogram预测模型具有较好的校准能力,见图5。
3" 讨论
冠心病发病机制可能与炎性反应、血管内皮功能异常、斑块破裂、氧化应激反应加剧有关,而PCI术后出血可能与血流动力学恶化、肾上腺素释放过度、免疫效应、炎性反应等有关[14⁃16]。因而,明确PCI术后出血危险因素,对于提高防治水平具有重要意义。
LASSO回归可降维处理相关性变量,筛选具有非零系数特征的变量,并将符合条件的变量纳入多因素Logistic回归分析,选择最优预测变量[17⁃18]。本研究结果显示,LASSO筛选出7个预测因子,包括年龄、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分,进一步采用Logistic回归分析发现,年龄≥60岁、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分是PCI术后1年出血的危险因素。老年病人脏器代偿功能、抵抗力下降,抗凝药物作用下其耐受程度较低,并可引起药物积蓄,增加术后出血风险[19⁃20]。本研究结果显示,出血组年龄≥60岁占比高于未出血组。临床工作者应密切关注高龄病人,并予以相应治疗措施,以降低PCI术后出血风险。有消化道病史者消化道黏膜屏障保护功能受损,可阻碍胃黏膜表皮生长因子合成,破坏消化道保护屏障,降低胃肠道黏膜防御功能,增加消化道出血风险[21⁃22]。本研究结果显示,出血组有消化道病史比例高于未出血组,提示有消化道病史可能作为预测PCI术后出血的潜在指标。临床应在术中适当减少肝素使用量,并在术后密切监测各项生理指标,以防出血发生。慢性肾功能不全可减少抗血栓药物排泄,促使双抗药物血药浓度偏高,引起消化道血管破裂,增加出血风险[23⁃24]。本研究结果显示,出血组慢性肾功能不全比例高于未出血组,这与既往研究结果[25]相似。临床医师应嘱咐病人在术前规律口服保肾药物,提高肾脏灌注压,术后保证机体容量、肾脏灌注,避免肾脏缺血。本研究结果显示,使用血管闭合器可增加PCI术后1年出血风险,这是因为血管闭合器可损伤血管内膜,降低血管壁回位封口能力[26]。球囊扩张次数增多可能促使血栓破裂、脱落,减慢远端血流速度,病变血管再通后血流缓慢,可促使斑块内容物溢出,这些微小固体可阻塞冠状动脉远端微血管,激活血小板,形成微血栓[27]。本研究结果显示出血组球囊扩张次数高于未出血组,这是因为球囊扩张次数增多预示存在严重病变,同时手术时间也会延长,可增加肝素使用剂量,造成血管内膜损伤,为了预防术后血栓发生,临床通常会提高抗凝药物应用剂量,进一步提高再度出血的可能性。
PARIS评分可用于评估置入支架并使用DAPT病人出院后2年内冠状动脉血栓事件,其可识别心肌梗死出血高危病人,还可预测缺血风险,但该评分推导主要依据欧美病人,关于其对亚洲东部病人预测准确性尚不明确[28⁃29]。PRECISE⁃DAPT评分可用于评估急性冠脉综合征(ACS)病人PCI术后出血风险及获益,以便指导临床医师制定个性化合理DAPT方案,但该评分易造成假阳性结果,可能增加缺血事件发生概率[30]。目前,PARIS、PRECISE⁃DAPT评分对我国心血管疾病病人出血风险预测价值有待证实,本研究结果与Castini等[31]研究结果相似,出血组PARIS、PRECISE⁃DAPT评分高于未出血组。临床工作者术前应评估病人PARIS、PRECISE⁃DAPT评分,有助于临床医师权衡利弊,以便制订合理DAPT方案。Nomogram预测模型不同变量有对应的分值,简洁、直观且无须复杂运算,可优化个体预测精度,促使预测模型结果更具可读性[32]。本研究创新之处在于基于LASSO⁃Logistic回归分析结果建立Nomogram预测模型,结果显示,Nomogram预测模型PCI术后1年出血的ROC曲线下面积为0.959,且校准能力良好。由此可知本研究建立的Nomogram预测模型预测PCI术后1年出血的临床应用潜力较大,有助于临床提前调整临床诊疗措施,为后续临床研究提供同质化标准。临床工作者应充分利用Nomogram预测模型,尽可能对出血高风险人群做到早发现、早干预,在术后抗血栓治疗中充分衡量临床获益、出血风险,以便制定个体化诊疗方案,降低相关危险因素所致危险性出血风险。
4" 小结
综上所述,年龄≥60岁、消化道病史、慢性肾功能不全、使用血管闭合器、球囊扩张次数、PARIS评分、PRECISE⁃DAPT评分为冠心病病人PCI术后1年出血危险因素,依据上述危险因素建立Nomogram预测模型,该模型对PCI术后1年出血具有一定预测价值,临床应重视高危因素,早期筛查高风险人群,综合评估出血风险,并改进治疗计划,以降低出血发生风险。本研究存在不足之处,尚未对单一出血风险予以针对性预测及因素识别,下一步将扩大样本量并将其作为研究方向及重点。
参考文献:
[1]" DONG Y,CHEN H,GAO J,et al.Molecular machinery and interplay of apoptosis and autophagy in coronary heart disease[J].J Mol Cell Cardiol,2019,136:27-41.
[2]" NICHOLS S,MCGREGOR G,BRECKON J,et al.Current insights into exercise-based cardiac rehabilitation in patients with coronary heart disease and chronic heart failure[J].Int J Sports Med,2021,42(1):19-26.
[3]" NAKAMURA M,YAMASHITA T,HAYAKAWA A,et al.Bleeding risks associated with anticoagulant therapies after percutaneous coronary intervention in Japanese patients with ischemic heart disease complicated by atrial fibrillation:a comparative study[J].J Cardiol,2021,77(2):186-194.
[4]" DIXON L K,AKBERALI U,DI TOMMASO E,et al.Hybrid coronary revascularization versus coronary artery bypass grafting for multivessel coronary artery disease:a systematic review and meta-analysis[J].Int J Cardiol,2022,359:20-27.
[5]" 贾蕾蕾,张标.预测高血压合并冠心病PCI术后支架内再狭窄nomogram模型的建立与验证[J].中国动脉硬化杂志,2023,31(2):148-156.
JIA L L,ZHANG B.Establishment and validation of a nomogram model for predicting in-stent restenosis after PCI in patients with hypertension and coronary heart disease[J].Chinese Journal of Arteriosclerosis,2023,31(2):148-156.
[6]" 赵忠平,丁晓云,罗正义.冠心病合并心房颤动患者PCI术后出血风险预测列线图的构建及验证[J].心脑血管病防治,2020,20(6):553-556.
ZHAO Z P,DING X Y,LUO Z Y.The construct and testing of prognostic nomogram concerning bleeding after percutaneous coronary intervention in patients with coronary disease combined with atrial fibrillation[J].Cardio-Cerebrovascular Disease Prevention and Treatment,2020,20(6):553-556.
[7]" 胡盛寿,高润霖,刘力生,等.《中国心血管病报告2018》概要[J].中国循环杂志,2019,34(3):209-220.
HU S S,GAO R L,LIU L S,et al.Summary of \"the 2018 report on cardiovascular diseases in China\"[J].Chinese Circulation Journal,2019,34(3):209-220.
[8]" HOWELL N J,KEOGH B E,BONSER R S,et al.Mild renal dysfunction predicts in-hospital mortality and post-discharge survival following cardiac surgery[J].Eur J Cardiothorac Surg,2008,34(2):390-395.
[9]" 中华医学会心血管病学分会,中华心血管病杂志编辑委员会.经皮冠状动脉介入治疗指南(2009)[J].中华心血管病杂志,2009,37(1):4-25.
Chinese Medical Association Cardiovascular Branch,Editorial Committee of Chinese Journal of Cardiovascular Disease.Guidelines for percutaneous coronary intervention(2009)[J].Chinese Journal of Cardiology,2009,37(1):4-25.
[10]" LU Y,LOFFROY R,LAU J Y,et al.Multidisciplinary management strategies for acute non-variceal upper gastrointestinal bleeding[J].Br J Surg,2014,101(1):e34-e50.
[11]" MEHRAN R,RAO S V,BHATT D L,et al.Standardized bleeding definitions for cardiovascular clinical trials:a consensus report from the Bleeding Academic Research Consortium[J].Circulation,2011,123(23):2736-2747.
[12]" MAHAFFEY K W,WOJDYLA D M,CARROLL K,et al.Ticagrelor compared with clopidogrel by geographic region in the platelet inhibition and patient outcomes(PLATO) trial[J].Circulation,2011,124(5):544-554.
[13]" KALETA F P,GILCHRIST I C.PRECISE-DAPT:a tool to measure if afib patients may risk being stretched too thin[J].Catheter Cardiovasc Interv,2021,98(5):846-847.
[14]" LIU Y,YE T,CHEN L,et al.Systemic immune-inflammation index predicts the severity of coronary stenosis in patients with coronary heart disease[J].Coron Artery Dis,2021,32(8):715-720.
[15]" YAMAMOTO K,NATSUAKI M,MORIMOTO T,et al.Ischemic and bleeding events after first major bleeding event in patients undergoing coronary stent implantation[J].Am J Cardiol,2022,162:13-23.
[16]" SAMUELSEN P J,EGGEN A E,STEIGEN T,et al.Incidence and risk factors for major bleeding among patients undergoing percutaneous coronary intervention:findings from the Norwegian coronary stent trial(NORSTENT)[J].PLoS One,2021,16(3):e0247358.
[17]" MORTAZAVI B J,BUCHOLZ E M,DESAI N R,et al.Comparison of machine learning methods with national cardiovascular data registry models for prediction of risk of bleeding after percutaneous coronary intervention[J].JAMA Netw Open,2019,2(7):e196835-e196845.
[18]" MA K,LI J,SHEN G,et al.Development and validation of a risk nomogram model for predicting contrast-induced acute kidney injury in patients with non-ST-elevation acute coronary syndrome undergoing primary percutaneous coronary intervention[J].Clin Interv Aging,2022,17:65-77.
[19]" ELAMRY E,ALKADY H M,MENAISSY Y,et al.Predictors of in-hospital mortality in isolated total anomalous pulmonary venous connection[J].Heart Surg Forum,2019,22(3):E191-E196.
[20]" SHI W,FAN X,YANG J,et al.In-hospital gastrointestinal bleeding in patients with acute myocardial infarction:incidence,outcomes and risk factors analysis from China Acute Myocardial Infarction Registry[J].BMJ Open,2021,11(9):e044117.
[21]" UEKI Y,VÖGELI B,KARAGIANNIS A,et al.Ischemia and bleeding in cancer patients undergoing percutaneous coronary intervention[J].JACC Cardio Oncol,2019,1(2):145-155.
[22]" CHOLANKERIL G,HU M,CHOLANKERIL R,et al.Inpatient outcomes for gastrointestinal bleeding associated with percutaneous coronary intervention[J].J Clin Gastroenterol,2019,53(2):120-126.
[23]" CHEN Y,TU S,CHEN Z,et al.Ticagrelor versus clopidogrel in patients with severe renal insufficiency undergoing PCI for acute coronary syndrome[J].J Interv Cardiol,2022,2022:6476777.
[24]" KUNO T,CLAESSEN B,CAO D,et al.Impact of renal function in high bleeding risk patients undergoing percutaneous coronary intervention:a patient-level stratified analysis from four post-approval studies[J].J Thromb Thrombolysis,2021,52(2):419-428.
[25]" 李博,欧柏青,邓婷智.PCI术后双联抗血小板导致消化道大出血的相关因素分析[J].湖南师范大学学报(医学版),2022,19(2):19-22.
LI B,OU B Q,DENG T Z.Analysis on related factors of massive gastrointestinal hemorrhage caused by dual antiplatelet therapy after PCI[J].Journal of Hunan Normal University(Medical Sciences),2022,19(2):19-22.
[26]" 邬晓臣,丁盛,王舰,等.血管闭合器在再次经股动脉途径主动脉腔内修复术中的临床疗效和安全性[J].心脏杂志,2022,34(6):680-682.
WU X C,DING S,WANG J,et al.Clinical efficacy and safety of endovascular closure device in patients undergoing another transarterial thoracic aortic repair[J].Chinese Heart Journal,2022,34(6):680-682.
[27]" DOOST A,MABOTE T,CLUGSTON R,et al.A case of covered stent failure in sealing up a coronary perforation potentially related to intravascular lithotripsy treatment:insights from optical coherence tomography[J].Eur Heart J Case Rep,2022,6(10):410.
[28]" VALGIMIGLI M,CAO D,ANGIOLILLO D J,et al.Duration of dual antiplatelet therapy for patients at high bleeding risk undergoing PCI[J].J Am Coll Cardiol,2021,78(21):2060-2072.
[29]" MOALEM K,BABER U,CHANDRASEKHAR J,et al.Incidence,predictors,and outcomes of DAPT disruption due to non-compliance vs.bleeding after PCI:insights from the PARIS Registry[J].Clinical Research in Cardiology,2019,108(6):643-650.
[30]" DANNENBERG L,AFZAL S,CZYCHY N,et al.Risk prediction of bleeding and MACCE by PRECISE-DAPT score post-PCI[J].Int J Cardiol Heart Vasc,2021,33:100750.
[31]" CASTINI D,CENTOLA M,FERRANTE G,et al.Comparison of CRUSADE and ACUITY-HORIZONS bleeding risk scores in patients with acute coronary syndromes[J].Heart Lung Circ,2019,28(4):567-574.
[32]" ZHENG W,ZHANG Y J,LIU R,et al.Prediction of gastrointestinal bleeding events in patients with acute coronary syndrome undergoing percutaneous coronary intervention:an observational cohort study (STROBE compliant)[J].Medicine (Baltimore),2020,99(30):e21312.
猜你喜欢
天津医科大学学报(2021年4期)2021-08-21 02:14:32
现代畜牧科技(2021年6期)2021-07-16 05:50:14
中国民间疗法(2021年1期)2021-04-20 02:31:16
基层中医药(2020年10期)2020-11-27 01:58:58
智慧健康(2019年36期)2020-01-14 15:22:58
饲料与畜牧(规模养猪)(2016年5期)2016-12-01 03:48:41
实用临床医学(2016年8期)2016-06-07 01:28:24
中国卫生标准管理(2015年3期)2016-01-14 03:41:45
山东医药(2015年14期)2016-01-12 00:39:55
天津护理(2015年4期)2015-11-10 06:11:29