
Analysis of factors impacting postoperative pain and quality of life in patients with mixed hemorrhoids: A retrospective study
2024-05-07 13:20XiaoWenSunJingYiXuChangZhenZhuSiJiaLiLuJiaJinZhiDongZhu
Xiao-Wen Sun,Jing-Yi Xu,Chang-Zhen Zhu,Si-Jia Li,Lu-Jia Jin,Zhi-Dong Zhu
Abstract BACKGROUND Hemorrhoids are among the most common and frequently encountered chronic anorectal diseases in anorectal surgery.They are venous clusters formed by congestion,expansion,and flexion of the venous plexus in the lower part of the rectum.Mixed hemorrhoids bleed easily and recurrently,and this can result in severe anemia.Hence,they may have a negative effect on the health of the patient and surgical treatment is required.Milligan-Morgan hemorrhoidectomy has been widely used since 1937 for the treatment of grade III and IV hemorrhoids.However,most patients experience different degrees of postoperative pain that may cause anxiety.AIM To assess the factors influencing pain scores and quality of life (QoL) in patients with mixed hemorrhoids post-surgery.METHODS The clinical data of patients with mixed hemorrhoids who underwent Milligan-Morgan hemorrhoidectomy were collected retrospectively.The basic characteristics of the enrolled patients with mixed hemorrhoids were recorded,and based on the Goligher clinical grading system,the hemorrhoids were classified as grades III or IV.The endpoint of this study was the disappearance of pain in all patients.Quantitative data were presented as mean ± SD,such as age,pain score,and QoL score.Student’s t-test was used to compare the groups.RESULTS A total of 164 patients were enrolled.The distribution of the visual analog scale pain scores of all patients at 3,7,14 and 28 d after surgery showed that post-surgery pain was significantly reduced with the passage of time.Fourteen days after the operation,the pain had completely disappeared in some patients.Twenty-eight days after the surgery,none of the patients experienced any pain.Comparing the World Health Organization Quality of Life -BREF self-reporting questionnaire scores of patients between 14 and 28 d after surgery,we observed that the quality-of-life scores of the patients post-surgery had significantly improved.There were six items that were compared at 14-and 28-d post-surgery.The mean QoL score 28 d after surgery (4.79 ± 0.46) was higher than that at 14 d post-surgery (3.79 ± 0.57).The mean health condition score 28 d after surgery (4.80 ± 0.41) was also higher than that at 14 d post-surgery (4.01 ± 0.62).The mean physical health score 28 d after surgery (32.10 ± 2.96) was significantly higher than that at 14 d post-surgery (23.41 ± 2.85).The mean psychological health score 28 d after surgery (27.22 ± 1.62) was significantly higher than that at 14 d post-surgery (21.37 ± 1.70).The mean social relations score 28 d after surgery (12.21 ± 1.59) was significantly higher than that at 14 d post-surgery (6.32 ± 1.66).The mean surrounding environment score 28 d after surgery (37.13 ± 2.88) was significantly higher than that at 14 d post-surgery (28.42 ± 2.86).The differences in quality-of-life scores at day 14 and day 28 post-surgery were observed to be statistically significant (P < 0.001).CONCLUSION Milligan-Morgan hemorrhoidectomy can significantly improve the postoperative QoL of patients.Age,sex,and the number of surgical resections were important factors influencing Milligan-Morgan hemorrhoidectomy.
Key Words: Hemorrhoids;Mixed hemorrhoids;Milligan organ hemorrhoidectomy;Postoperative pain;Quality of life;Anesthesia mode
lNTRODUCTlON
Hemorrhoids are among the most common and frequently encountered chronic anorectal diseases in anorectal surgery[1].They are venous clusters formed by congestion,expansion,and flexion of the venous plexus in the lower part of the rectum[2].The symptoms of hemorrhoids include bright red bleeding from the anus and intestines,mucus discharge,perianal irritation or itching,pain around the anus,hemorrhoid pad prolapse or protruding masses,and staining of the underwear[3].Hemorrhoids affect 4.40% of the global population,with a global incidence of approximately 49.14%[4].In China,51.14% adults of the total surveyed population suffer from anorectal diseases,where hemorrhoids constitute the highest incidence rate (50.28%)[5].According to the Goligher clinical grading system,hemorrhoids are classified as grades I-IV[6].Grades I and II can usually be controlled with conservative treatment,while Grades III and IV often require surgery.Mixed hemorrhoids are among the most common types of hemorrhoids and are comprised of internal and external hemorrhoid vascular plexuses of the corresponding site of mutual fusion[7].The pathological mechanism that generates internal hemorrhoids involves the supporting structure of the anal cushion (anal canal vascular cushion),pathological changes and displacement of the vascular plexus,and arteriovenous anastomosis[8].The pathological mechanism of external hemorrhoids involves the expansion of the subcutaneous vascular plexus in the distal dentate line,blood flow stasis,thrombosis,or tissue hyperplasia[9].Mixed hemorrhoids bleed easily and recurrently,and this can result in severe anemia.Hence,they may have a negative effect on the health of the patient and surgical treatment is required.Milligan-Morgan hemorrhoidectomy has been widely used since 1937 for the treatment of grade III and IV hemorrhoids.However,most patients experience different degrees of postoperative pain that may cause anxiety[10].Based on the current status of surgical options for grade III and IV hemorrhoids,this study aimed to evaluate the curative effect of mixed hemorrhoid surgery through patient feedback.
MATERlALS AND METHODS
Patients
This was a retrospective study involving patients with mixed hemorrhoids (grade III or IV).All patients underwent external pile-excision and internal pile-ligature operations for mixed hemorrhoid treatment in Beijing Tsinghua Changgung Hospital from November 1,2020,to October 31,2021 (Figure 1).

Figure 1 Flow chart of the study showing inclusion and exclusion criteria.
Inclusion criteria:The following inclusion criteria were applied in this study: (1) Patients who were diagnosed with mixed hemorrhoids (grades III and IV) based on the Goligher clinical grading system for the classification of hemorrhoids;(2) Patients who had clinical symptoms that may affect daily life;(3) Patients who had ineffective conservative treatment;(4) Patients who underwent surgery with good compliance;(5) Patients who had never undergone mixed hemorrhoid surgery before;(6) Patients who had signed the consent forms voluntarily;(7) Patients who successfully completed the surgery;and (8) Patients who were followed up and observed for 28 d after the operation.
Exclusion criteria:The exclusion criteria were as follows: (1) Patients who have had mixed hemorrhoids surgery or other perianal disease surgery before;(2) Patients who had severe systemic diseases or severe primary diseases (such as cardiac,cerebrovascular,hepatic,renal,or hematopoietic system diseases);(3) Patients who had severe mental illness,such as severe depression or mania;(4) Patients who were either pregnant,breastfeeding or were women experiencing menstrual periods;(5) Patients with rectal cancer,tuberculosis,Crohn's disease and other rectal and anal diseases;(6) Patients with allergies;or (7) Patients who voluntarily abandoned treatment prior to surgery.
Methods
Surgical method:We employed Milligan-Morgan hemorrhoidectomy to remove mixed hemorrhoids.
Observational indicators and follow up:The observational indicators for this study were as follows: (1) Improvement in pain post-surgery;(2) Changes in quality-of-life post-surgery.The patients were observed for 28 d after surgery.At 3,7,14,and 28 d after surgery,the Visual Analog Scale (VAS) of pain intensity was used to assess the pain levels of patients.At 14-and 28-d post-surgery,the World Health Organization Quality of Life -BREF (WHOQOL-BREF) self-reporting questionnaire was used to assess the quality of life (QoL) of patients.At 3-,7-,and 14-d post-surgery,the patients did not undergo digital rectal examination to avoid suture tearing.At 28 d post-surgery,we evaluated the treatment effect by using a digital rectal examination.
Statistical analysis
Data were processed by using the SPSS 27 software (IBM SPSS,Armonk,NY,USA).Quantitative data,such as age,pain scores,and QoL scores,were presented as mean ± SD.The Student’st-test was used to compare the groups.Factors influencing postoperative pain and the WHOQOL-BREF scores were analyzed by using multiple linear regression.AllPvalues less than 0.05 were considered to be statistically significant.
RESULTS
A total of 164 patients were included in this study.The basic patient information is shown in Table 1.

Table 1 Basic characteristics of 164 patients,n (%)
The distribution of the VAS-based pain scores of all patients at 3,7,14 and 28 d after surgery are shown in Table 2.Post-surgery pain was significantly reduced with the passage of time.Fourteen days after the operation,the pain had completely disappeared in some patients.Twenty-eight days after the surgery,none of the patients experienced any pain.

Table 2 Distribution of pain scores at 3,7,14 and 28 d after surgery

Table 3 Comparison of World Health Organization Quality of Life -BREF score between 14 and 28 d after surgery

Table 4 Multiple linear regression analysis of the factors that impact the postoperative pain scores
Comparing the WHOQOL-BREF scores of patients at 14 and 28 d after surgery,we used one-way repeated measures analysis of variance and determined whether there is a significant improvement in the QoL of patients at 14 and 28 d after surgery.According to the boxplot,there were no outliers in the data.According to the Shapiro-Wilk test,the data of each group followed a normal distribution (P> 0.05);According to the Mauchly spherical hypothesis test,the variance-covariance matrix of the dependent variable was equal.The data was presented in the form of mean ± SD.There were six items that were compared at 14-and 28-d post-surgery.The difference in scores in each group had statistically significant.QoL score:F=629.368,P< 0.001;health condition score:F=294.936,P< 0.001;physical health score:F=6190.930,P< 0.001;psychological health score:F=6168.725,P< 0.001;social relations score:F=6719.581,P< 0.001;surrounding environment score:F=6414.756,P< 0.001.The mean QoL score 28 d after surgery (4.79 ± 0.46) was higher than that at 14 d post-surgery (3.79 ± 0.57).The mean health condition score 28 d after surgery (4.80 ± 0.41) was also higher than that at 14 d post-surgery (4.01 ± 0.62).The mean physical health score 28 d after surgery (32.10 ± 2.96) was significantly higher than that at 14 d post-surgery (23.41 ± 2.85).The mean psychological health score 28 d after surgery (27.22 ± 1.62) was significantly higher than that at 14 d post-surgery (21.37 ± 1.70).The mean social relations score 28 d after surgery (12.21 ± 1.59) was significantly higher than that at 14 d post-surgery (6.32 ± 1.66).The mean surrounding environment score 28 d after surgery (37.13 ± 2.88) was significantly higher than that at 14 d post-surgery (28.42 ± 2.86).The differences in QoL scores at day 14 and day 28 post-surgery were observed to be statistically significant (P< 0.001) (Tables 3 and 4).
Multiple linear regression analysis of the WHOQOL-BREF scores at 14 and 28 d after mixed hemorrhoid surgery showed that age and sex,but not anesthesia mode and number of surgical resections (P> 0.05),were the factors influencing mixed hemorrhoid surgery outcomes (P< 0.05) (Table 5).
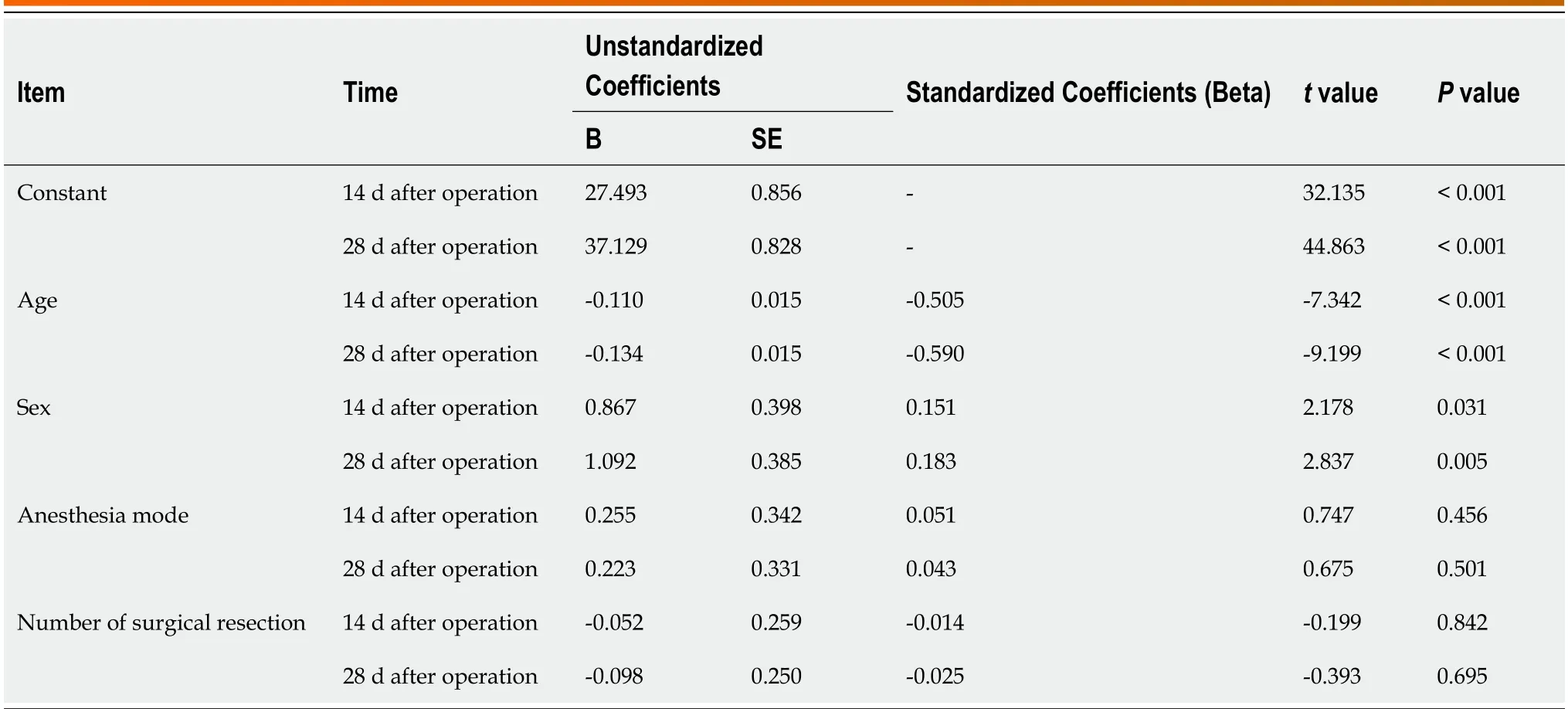
Table 5 Multiple linear regression analysis of the factors that impact postoperative World Health Organization Quality of Life -BREF scores
DlSCUSSlON
Hemorrhoids is a benign but commonly occurring chronic disease that can disrupt the daily lives and well-being of patients[11].The overall prevalence of hemorrhoids among the study participants was 14.4% and was higher among women (15.7%) than among men (13.0%).A nationwide cross-sectional study of Korean adults suggested that obesity,abdominal obesity,depression,and past pregnancy may be risk factors for hemorrhoids that negatively affect the QoL[12].Hemorrhoidectomy is one of the most common procedures performed during anorectal surgery[13].Patients who underwent surgery showed significant differences in activities of daily living before and after surgery.The patients were satisfied with their lives after surgery[14].
One of the major purposes of our study was to assess the factors influencing the QoL of patients after hemorrhoidectomy using the Milligan-Morgan procedure.In our study,most improvements in hemorrhoid-specific QoL and severe symptoms occurred 2 wk after surgery.Most patients did not report taking other medications during this period,and none returned to the hospital because of worsening symptoms.
In a longitudinal observational study,bleeding and soiling showed significant improvements in symptom severity from weeks 4 to 8 post-surgery,whereas pain,itching,and swelling/prolapse did not[15].This difference in the improvement of specific symptoms may be attributed to the surgical techniques used.Xiaet al[16] suggested that the male sex and surgical techniques are associated with an increased risk of readmission.
Keonget al[15] found pain,bleeding,soiling,itching,and swelling/prolapse to be the factors that affect the QoL of patients.In the present study,we found that age,sex,and number of resections were factors affecting the QoL of patients.We also found that age,sex,and number of resections were risk factors for postoperative pain after hemorrhoidectomy using the Milligan-Morgan procedure.The subjective feelings of patients were used as the main option in this study.Postoperative pain after Milligan-Morgan hemorrhoidectomy remains a problem for colorectal surgery teams[17].Patients experience prolonged,intractable anal pain that adversely affects their QoL.However,in the present study,the patients experienced minimal pain.The patients experienced excruciating pain during and half an hour after defecation.
Effective analgesic therapy plays an important role in improving QoL for them.Therefore,laxatives were administered to all patients.In our study,the symptoms improved 2 wk after surgery.We therefore selected 3-and 7-d post-surgery as appropriate observation time-points.
A retrospective cohort association study[18] has indicated that postoperative pain decreases with increasing age.A total of 11510 patients from 26 countries (59% women;mean age 62 years) underwent one of the aforementioned types of surgery.These results are consistent with those of the present study.
In our study,we found that men experienced pain more intensely than women.Psychological factors such as anxiety,distress,and pain catastrophizing play relevant roles in the development of pain after surgery[19].Hormones may possibly mediate the role of sex differences in post-surgical pain by contributing to fluctuations in pain sensitivity across the menstrual cycle in women[20].Furthermore,in 58 studies (published between September 2013 and March 2015) assessing sex differences in patients undergoing various surgical procedures,women seemed to be at a higher risk of developing severe postoperative pain[21].
As the number of excisions increased,pain increased.Hemorrhoidectomy may partially injure the submucosal plexus along with the underlying muscles and alter the neuroregulation of the rectal muscles,leading to rectal hyperactivity and spasms.We found that the more tissue was removed,the more likely the anus was to develop swelling.
Our study found that neither QoL nor postoperative pain was affected by the mode of anesthesia.In a report from Nigeria[22],22 (18.3%) patients consented to undergo ligation and excisional hemorrhoidectomy under local anesthesia.As many as 88 (73.3%) patients were managed conservatively,eight (6.7%) had surgery under spinal anesthesia and two(1.7%) patients had surgery under general anesthesia.Surgeries done under local anesthetic have some important advantages that include early ambulation and subsequent discharge from the hospital,and a reduction in the total cost of the procedure[22].As regards local anesthetic infiltration for the rubber band ligation of early symptomatic hemorrhoids,a systematic review and meta-analysis found that the post-procedure pain score (SMD: -5.19;95%CI: -9.08 to -1.30;Z=2.62;P< 0.009) was significantly lower in the group of patients undergoing rubber band ligation of hemorrhoids under local anesthetic injection[23].
CONCLUSlON
This study demonstrated that Milligan-Morgan hemorrhoidectomy can significantly improve the postoperative QoL of patients.Age,sex,and the number of surgical resections were the factors that influenced postoperative pain but were not related to the anesthesia mode.With an increase in illness duration,the number of mixed hemorrhoids gradually increased.With an increase in the number of resections,the degree of postoperative pain and the QoL of patients also worsened.The findings of this study are directly applicable to clinical practice,providing valuable insights for healthcare professionals.Therefore,we suggest that once a diagnosis of mixed hemorrhoids (grades III and IV) is made,surgery should be performed as soon as possible,regardless of the presence or absence of obvious symptoms.The study's con-clusions are relevant and applicable to other similar populations or settings,suggesting their generalizability across different contexts.However,this study still has limitations.Firstly,the influence of anesthesia on postoperative pain is unclear.In addition,the number of local anesthesia cases was relatively small.The costs of intrathecal and general anesthesia are much higher than that of local anesthesia.Meanwhile,we did not count the time required for anesthesia recovery and the adverse reactions caused by anesthesia.Also,we did not conduct detailed statistics on the length of hospital stay for patients,which is also one of the issues that patients are very concerned about.In future research,we will pay more attention to the above-mentioned issues and include a larger number of such local anesthesia cases with hopes of reducing medical expenses for patients while improving the quality of research in this area.The study's conclusions should be viewed within the context of its limitations,which should be further addressed in future research.It is a single-center study with a small sample size,and further multi-center large-sample studies are needed to confirm its feasibility.
ARTlCLE HlGHLlGHTS
Research background
Hemorrhoids are a common chronic anorectal disease characterized by the formation of venous clusters in the lower part of the rectum.Mixed hemorrhoids,in particular,often cause recurrent bleeding and can lead to severe anemia,negatively impacting the patient's health.Surgical treatment,such as Milligan-Morgan hemorrhoidectomy,is often necessary.However,postoperative pain is a common concern for patients undergoing this procedure,which can cause anxiety and affect their quality of life (QoL).
Research motivation
This study provides valuable information on improving surgical outcomes and postoperative care for patients with mixed hemorrhoids.
Research objectives
This study aimed to assess the factors influencing pain scores and QoL in patients with mixed hemorrhoids post-surgery.
Research methods
This retrospective study collected clinical data from patients with mixed hemorrhoids who underwent Milligan-Morgan hemorrhoidectomy.The basic characteristics of the enrolled patients with mixed hemorrhoids were recorded,and based on the Goligher clinical grading system,the hemorrhoids were classified as grades III or IV.
Research results
The results showed a significant reduction in postoperative pain over time,with some patients experiencing complete pain relief at 14 d and none reporting any pain at 28 d after surgery.Comparing the QoL scores between 14 and 28 d postsurgery,significant improvements were observed in various domains including overall QoL,health condition,physical health,psychological health,social relations,and surrounding environment.Milligan-Morgan hemorrhoidectomy was found to significantly improve the postoperative QoL for patients.
Research conclusions
Milligan-Morgan hemorrhoidectomy offers a promising approach for alleviating the negative impact of mixed hemorrhoids on patients' health and QoL.
Research perspectives
Several perspectives can be considered for future studies on mixed hemorrhoids and Milligan-Morgan hemorrhoidectomy.Firstly,further investigations could focus on optimizing pain management strategies post-surgery to minimize discomfort and anxiety in patients.Exploring alternative analgesic approaches or combination therapies may contribute to even better pain relief outcomes.Secondly,the impact of Milligan-Morgan hemorrhoidectomy on long-term QoL could be explored to assess whether the observed improvements are sustained over an extended period.Longitudinal studies could provide valuable insights into the durability of the procedure's benefits.Additionally,future research could delve deeper into the specific factors that influence the outcomes of Milligan-Morgan hemorrhoidectomy,such as age,sex,and the number of surgical resections.Understanding how these variables interact and affect surgical success could aid in tailoring treatment strategies for individual patients.Lastly,comparative studies could be conducted to evaluate the effectiveness and safety of Milligan-Morgan hemorrhoidectomy in comparison to other surgical techniques or emerging minimally invasive procedures.Such comparative analyses would help guide clinical decisionmaking and provide a comprehensive understanding of the available treatment options for mixed hemorrhoids.Overall,these research perspectives aim to further enhance the surgical management and overall well-being of patients with mixed hemorrhoids.
FOOTNOTES
Co-first authors:Xiao-Wen Sun and Jing-Yi Xu.
Author contributions:Sun XW,Xu JY,and Zhu ZD proposed the concept of this study,Zhu CZ participated in the data collection work,and Sun XW and Xu JY drafted the initial draft;Li SJ and Jin LJ contributed to the formal analysis of this study,while Zhu ZD conducted guiding research,methodology,and visualization;Xu JY validated the study,and all authors participated in the study and jointly reviewed and edited the manuscript;Sun XW and Xu JY have made equal contributions to this work as co-first authors.
lnstitutional review board statement:This study has been reviewed and approved by the Medical Ethics Committee of Tsinghua University Affiliated Beijing Tsinghua Changgeng Hospital.
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:We declare that there is no disclosure of any interest relationship.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Xiao-Wen Sun 0009-0007-1258-8103;Jing-Yi Xu 0009-0000-8464-2315;Zhi-Dong Zhu 0009-0009-8434-3257.
S-Editor:Wang JL
L-Editor:A
P-Editor:Xu ZH
 World Journal of Gastrointestinal Surgery2024年3期
World Journal of Gastrointestinal Surgery2024年3期
- World Journal of Gastrointestinal Surgery的其它文章
- Alcohol associated liver disease and bariatric surgery: Current perspectives and future directions
- Applications of gastric peroral endoscopic myotomy in the treatment of upper gastrointestinal tract disease
- Ex vivo liver resection and auto-transplantation and special systemic therapy in perihilar cholangiocarcinoma treatment
- Evaluation of bacterial contamination and medium-term oncological outcomes of intracorporeal anastomosis for colon cancer: A propensity score matching analysis
- Rescue from complications after pancreaticoduodenectomies at a low-volume Caribbean center: Value of tailored peri-pancreatectomy protocols
- Comparison of prognosis and postoperative morbidities between standard pancreaticoduodenectomy and the TRlANGLE technique for resectable pancreatic ductal adenocarcinoma