
Evaluation of bacterial contamination and medium-term oncological outcomes of intracorporeal anastomosis for colon cancer: A propensity score matching analysis
2024-05-07 13:20HajimeKayanoNanaMamuroYutaroKameiTakashiOgimiHiroshiMiyakitaToshioNakagohriKazuoKoyanagiMasakiMoriSeiichiroYamamoto
Hajime Kayano,Nana Mamuro,Yutaro Kamei,Takashi Ogimi,Hiroshi Miyakita,Toshio Nakagohri,Kazuo Koyanagi,Masaki Mori,Seiichiro Yamamoto
Abstract BACKGROUND Although intracorporeal anastomosis (IA) for colon cancer requires longer operative time than extracorporeal anastomosis (EA),its short-term postoperative results,such as early recovery of bowel movement,have been reported to be equal or better.As IA requires opening the intestinal tract in the abdominal cavity under pneumoperitoneum,there are concerns about intraperitoneal bacterial infection and recurrence of peritoneal dissemination due to the spread of bacteria and tumor cells.However,intraperitoneal bacterial contamination and mediumterm oncological outcomes have not been clarified.AIM To clarify the effects of bacterial and tumor cell contamination of the intraabdominal cavity in IA.METHODS Of 127 patients who underwent laparoscopic colon resection for colon cancer from April 2015 to December 2020,75 underwent EA (EA group),and 52 underwent IA (IA group).After propensity score matching,the primary endpoint was 3-year disease-free survival rates,and secondary endpoints were 3-year overall survival rates,type of recurrence,surgical site infection (SSI) incidence,number of days on antibiotics,and postoperative biological responses.RESULTS Three-year disease-free survival rates did not significantly differ between the IA and EA groups (87.2% and 82.7%,respectively,P=0.4473).The 3-year overall survival rates also did not significantly differ between the IA and EA groups (94.7% and 94.7%,respectively;P=0.9891).There was no difference in the type of recurrence between the two groups.In addition,there were no significant differences in SSI incidence or the number of days on antibiotics;however,postoperative biological responses,such as the white blood cell count (10200 vs 8650/mm3,P=0.0068),C-reactive protein (6.8 vs 4.5 mg/dL,P=0.0011),and body temperature (37.7 vs 37.5 °C,P=0.0079),were significantly higher in the IA group.CONCLUSION IA is an anastomotic technique that should be widely performed because its risk of intraperitoneal bacterial contamination and medium-term oncological outcomes are comparable to those of EA.
Key Words: Colon cancer;Ⅰntracorporeal anastomosis;3-year disease-free survival;Recurrence;Surgical site infection;Postoperative biological response
lNTRODUCTlON
For the surgical treatment of colorectal cancer,laparoscopic surgery,as a minimally invasive treatment method,has become one of the standard treatments based on the results of trials to confirm short-and long-term outcomes in comparisons of open surgery and laparoscopic surgery[1-4].As a further development of minimally invasive treatment methods,robot-assisted surgery is now being performed for colon cancer as well as rectal cancer.On the other hand,in the anastomosis method for gastrointestinal reconstruction,the intracorporeal anastomosis (IA) method has been used since the dawn of laparoscopic surgery for gastric cancer,which is also a type of gastrointestinal cancer.However,although laparoscopic surgery was more rapidly adopted for colorectal cancer than for gastric cancer,the use of IA for colorectal cancer has not spread as fast as for gastric cancer.In the case of IA for colorectal cancer,a randomized,controlled trial reported early recovery of intestinal peristalsis and reduction of complications[5,6] in terms of short-term outcomes,and in a site-specific study of colon cancer,there were no differences in survival and recurrence-free survival rates between IA and extracorporeal anastomosis (EA) for right-sided colon cancer[7,8].In addition,IA for left-sided colon cancer was reported to result in early recovery of intestinal peristalsis and a low complication rate[9,10].Numerous reports have documented the benefits of IA.However,because IA involves opening the intestinal tract in the abdominal cavity under pneumoperitoneum,there are still some concerns about bacterial infection and the spread of tumor cells,and the number of facilities performing IA is limited.Therefore,the purpose of this study was to clarify the effects of bacterial and tumor cell contamination by comparing IA and EA methods,with the primary endpoint of 3-year diseasefree survival (DFS) rate and secondary endpoints of 3-year overall survival (OS) rate,type of recurrence,surgical site infection (SSI) incidence rate,number of days on antibiotics,and postoperative biological responses.
MATERlALS AND METHODS
Patient selection
This retrospective,cohort study investigated 195 laparoscopic colon resections performed from April 2015 to December 2020 for colon cancer.Data for a total of 127 patients,75 in the EA group and 52 in the IA group,who underwent laparoscopic colon resection for first colon cancer were analyzed after excluding 4 cases of multiple colon cancer,2 cases of simultaneous double cancer,2 cases of resection with other organs,11 cases with distant metastasis,and 49 cases in which double-stapling technique anastomosis was performed (Figure 1).This study was designed in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the Research Ethics Committee,Tokai University School of Medicine (23RC011),with a waiver of informed consent.The choice of IA or EA was left entirely to the surgeon.
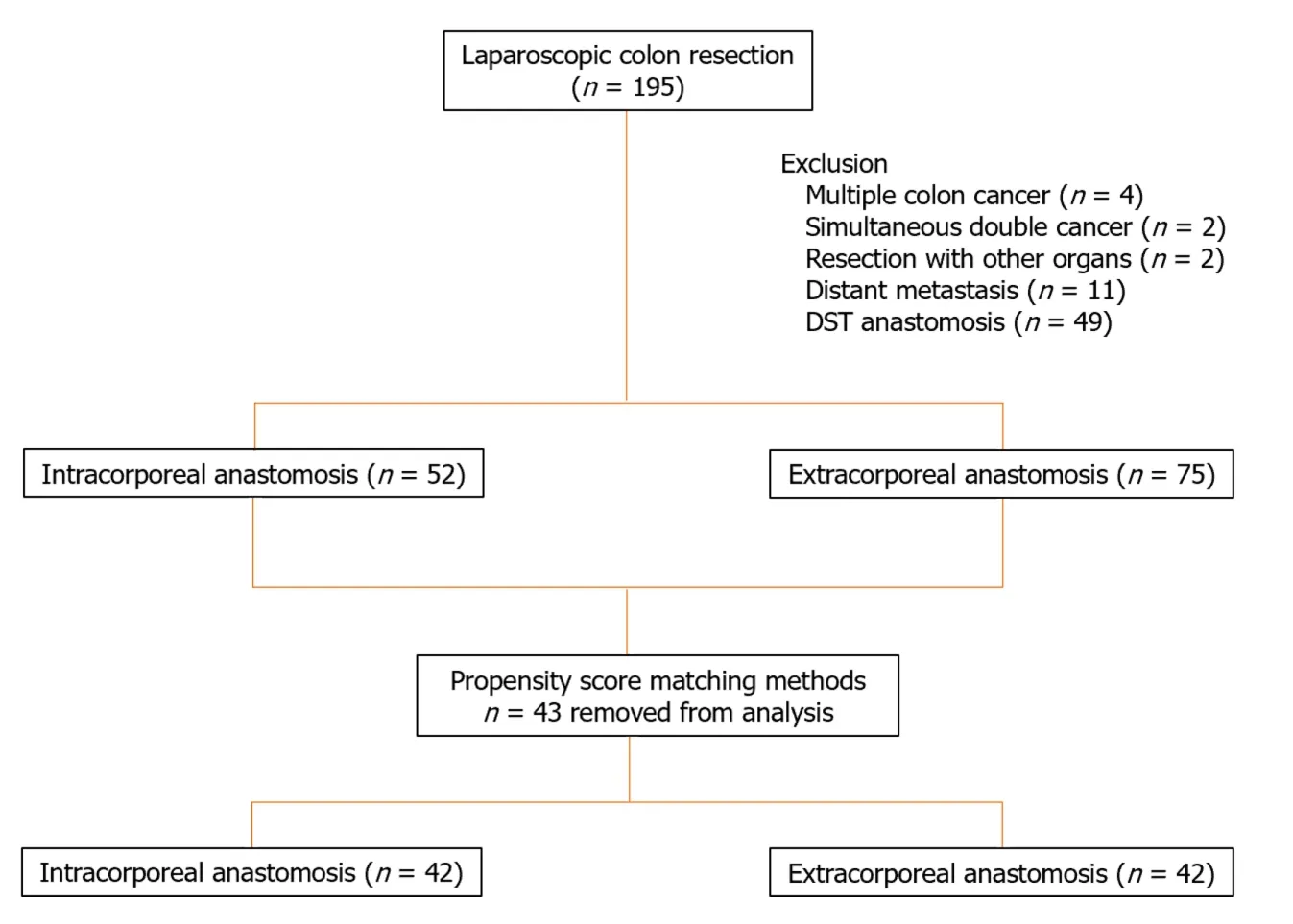
Figure 1 Flowchart of clinical data selection in this study. DST: Double-stapling technique.
Data collection
Information on patient-related factors,surgery-related factors,tumor-related factors,surgical outcomes,and short-and medium-term postoperative outcomes is held in a database.Patient-related factors included age,sex,body mass index (BMI),American Society of Anesthesiologists physical status (ASA-PS),Charlson comorbidity index (CCI),previous abdominal surgery,and carcinoembryonic antigen (CEA) levels.Surgery-related factors included bowel preparation,surgical procedure,and lymph node dissection area[11].Tumor-related factors included tumor location,maximum tumor diameter,differentiation,histopathologic T stage,histopathologic N stage (American Joint Committee on Cancer/International Union for Cancer Control),lymphatic invasion,venous invasion,and perineural invasion,as well as TNM stage classification.Surgical outcomes included operative time,blood loss,conversion to open surgery,intraoperative complications,incision length,number of harvested lymph nodes,proximal margin,distal margin,and results of peritoneal fluid bacterial culture and cytology after peritoneal lavage with 3000 mL of saline solution after anastomosis.Bacterial culture and cytology of peritoneal lavage were performed in 73 patients (36 in the EA group and 37 in the IA group) who underwent surgery since April 2016.Short-term postoperative outcomes were times to first pass gas and first stool,time to resumption of oral intake,number of analgesics used,number of days on antibiotics,duration of postoperative hospitalization,time from surgery to adjuvant chemotherapy,completion of adjuvant chemotherapy,and duration of adjuvant chemotherapy.Postoperative complications were defined as total complications,SSI,and anastomotic leakage.Postoperative complications were classified according to the Clavien-Dindo (CD) classification[12].The medium-term postoperative outcomes were defined as 3-year OS,3-year DFS,and type of recurrence.
Operative procedure
For EA,the intestinal tract was guided out of the body,and the oral and anal sides of the intestinal tract were separated by linear staplers.Then,a small hole was created on the transected side of the oral and anal intestinal tracts,and a linear stapler was inserted through the small holes to perform the anastomosis.The small hole was then closed with a linear stapler to create a functional end-to-end anastomosis.For IA,the oral and anal sides of the intestinal tract were separated by a linear stapler under laparoscopy.Small holes were made at a site 3 cm from the transected side of the oral intestinal tract and at a site 7 cm from the transected side of the anal intestine,and a stapler was inserted for lateral anastomosis with sequential peristalsis.The small hole was closed either by suture closure with a stapler or by suture closure with an A-L anastomosis using a 3-0 V-Loc (Medtronic,Minneapolis,MN,United States).Both anastomoses were performed using an ECHELON FLEXTMPowered ENDOPATH Stapler®60 mm (blue cartridge) (Ethicon Endo-Surgery Inc.,Cincinnati,OH,United States).Specimens were removed by extending the umbilical port wound.
Postoperative surveillance
In accordance with the colorectal cancer treatment guidelines prepared and published by the Japanese Society for Cancer of the Colon and Rectum,tumor markers were measured every 3 months,contrast-enhanced thoracoabdominal computed tomography (CT) was performed every 6 months,and the patients were examined.Positron emission tomography (PET)-CT was performed in all cases in which recurrence or metastasis was suspected on contrast-enhanced thoracoabdominal CT,and only when metastasis was diagnosed by PET-CT was the diagnosis confirmed as recurrence or metastasis.All imaging findings were diagnosed by a radiologist.
Statistical analysis
Propensity score matching was performed using a logistic regression model.One-to-one matching between the two groups was performed using the nearest neighbor matching method without replacement and with a caliper width of 0.2 standard deviations of the estimated propensity score logit.In the comparison between the two groups,the Mann-Whitney test was used for continuous variables,and the Chi-square test or Fisher’s exact test (for small sample sizes) was used for categorical variables,withP< 0.05 considered significant.OS and DFS were analyzed using the Kaplan-Meier method.Differences in survival curves were analyzed by the log-rank test.The index date for survival rate calculation was the date of surgery.The software used for this statistical analysis was JMP for Windows,version 13.0 (SAS Institute,Cary,NC,United States).
RESULTS
Patient characteristics before and after matching
The patient characteristics of each group before and after propensity score adjustment are shown in Table 1.Of the 127 patients analyzed,52 were in the IA group,and 75 were in the EA group.There were significant differences between the IA and EA groups in surgical procedure (P=0.0249) and extent of lymph node dissection (P=0.0133).Propensity score matching was performed using surgical procedure,lymph node dissection area,and TNM stage classification as covariates.No differences between the two groups were observed after matching.
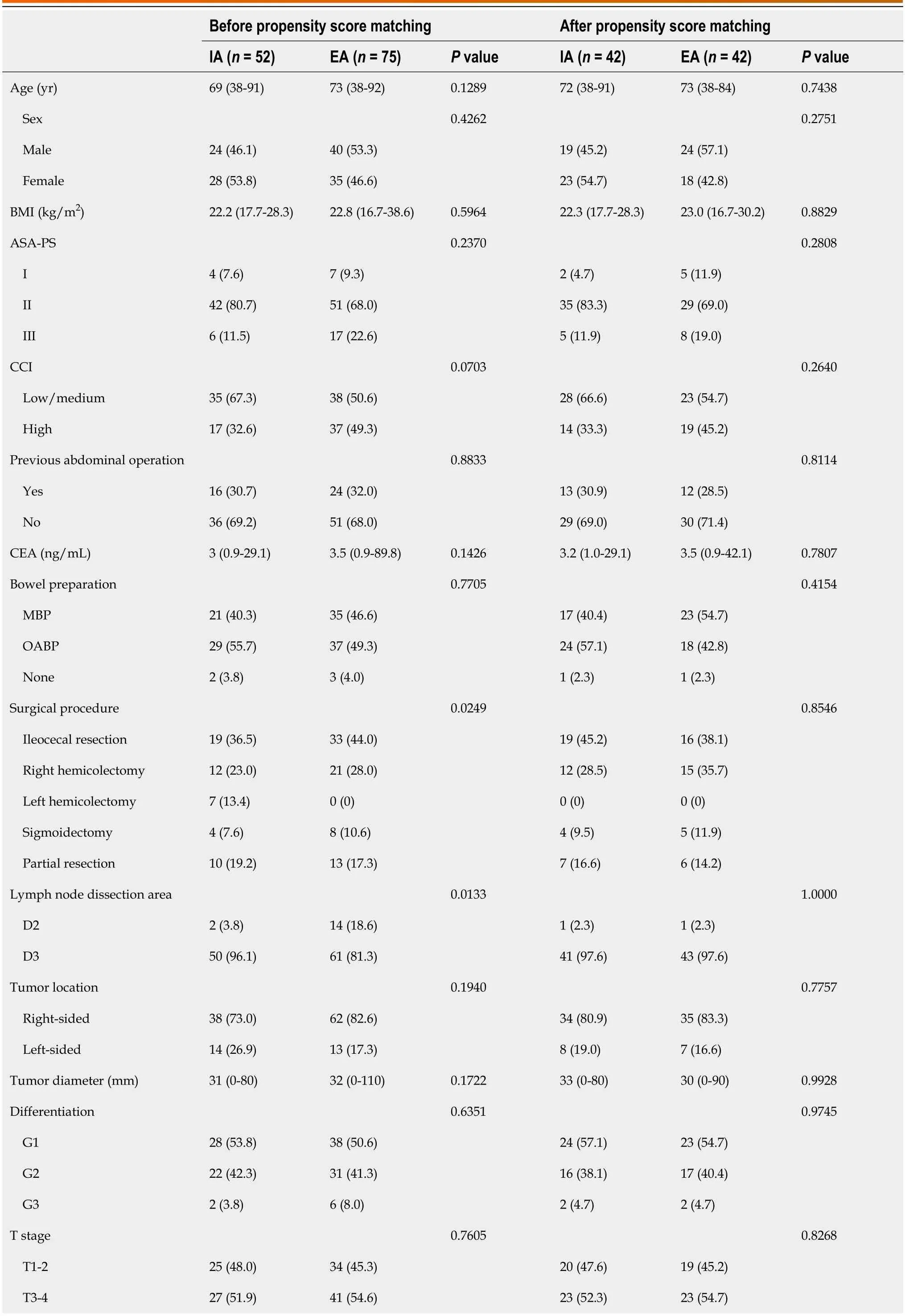
Table 1 Patients’ characteristics before and after propensity score matching,n (%)
Surgical outcomes
There was no difference between the IA and EA groups in operative time,but the IA group had significantly less blood loss (14vs42 mL,P=0.0087),shorter incision length (3vs4 cm,P=0.0001),and longer distal margin length (100vs80 mm,P=0.0071) than the EA group (Table 2).Bacterial culture and cytology of peritoneal lavage were performed for 39 patients in the IA group and 24 patients in the EA group.The results of bacterial culture of peritoneal lavage showed that the percentage of positive bacterial cultures was higher in the IA group,but the difference was not significant.Cytology results showed no difference between the two groups (Table 3).
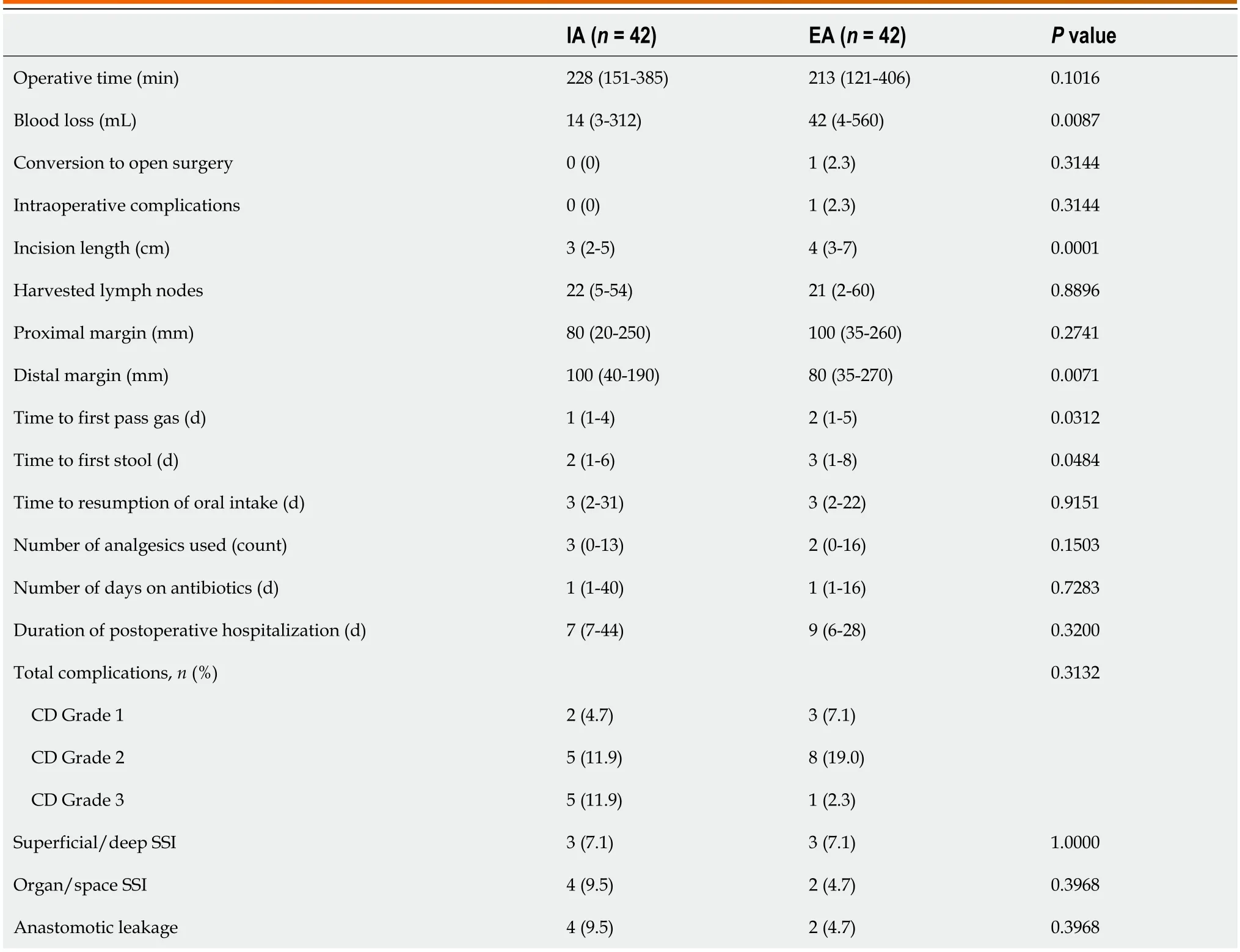
Table 2 Surgical outcomes and short-term postoperative outcomes

Table 3 Evaluation of peritoneal lavage fluid bacterial culture and cytology,n (%)
Short-term postoperative outcomes
The IA group had a significantly faster time to first pass gas (1vs2 d,P=0.0312) and time to first stool (2vs3 d,P=0.0484) than the EA group.The number of days on antibiotics did not differ between the two groups.Postoperative complications,including total complications,superficial/deep SSI,organ/space SSI,and anastomotic leakage,did not differ between the two groups.Postoperative biological responses are shown in Table 4.On the first postoperative day,the WBC count (10200vs8650/mm3,P=0.0068),C-reactive protein (6.8vs4.5 mg/dL,P=0.0011),and body temperature (37.7vs37.5 °C,P=0.0079) were all significantly higher in the IA group than in the EA group.No difference was observed between the two groups after the fourth and seventh days.There was no difference in the percentage of patients receiving adjuvant chemotherapy between the two groups (33.3%vs40.4%,P=0.5634).Fourteen patients (33.3%) in the IA group and 17 patients (40.4%) in the EA group received adjuvant chemotherapy.No differences between the groups were observed for time from surgery to adjuvant chemotherapy and completion rate or duration of adjuvant chemotherapy (Table 5).
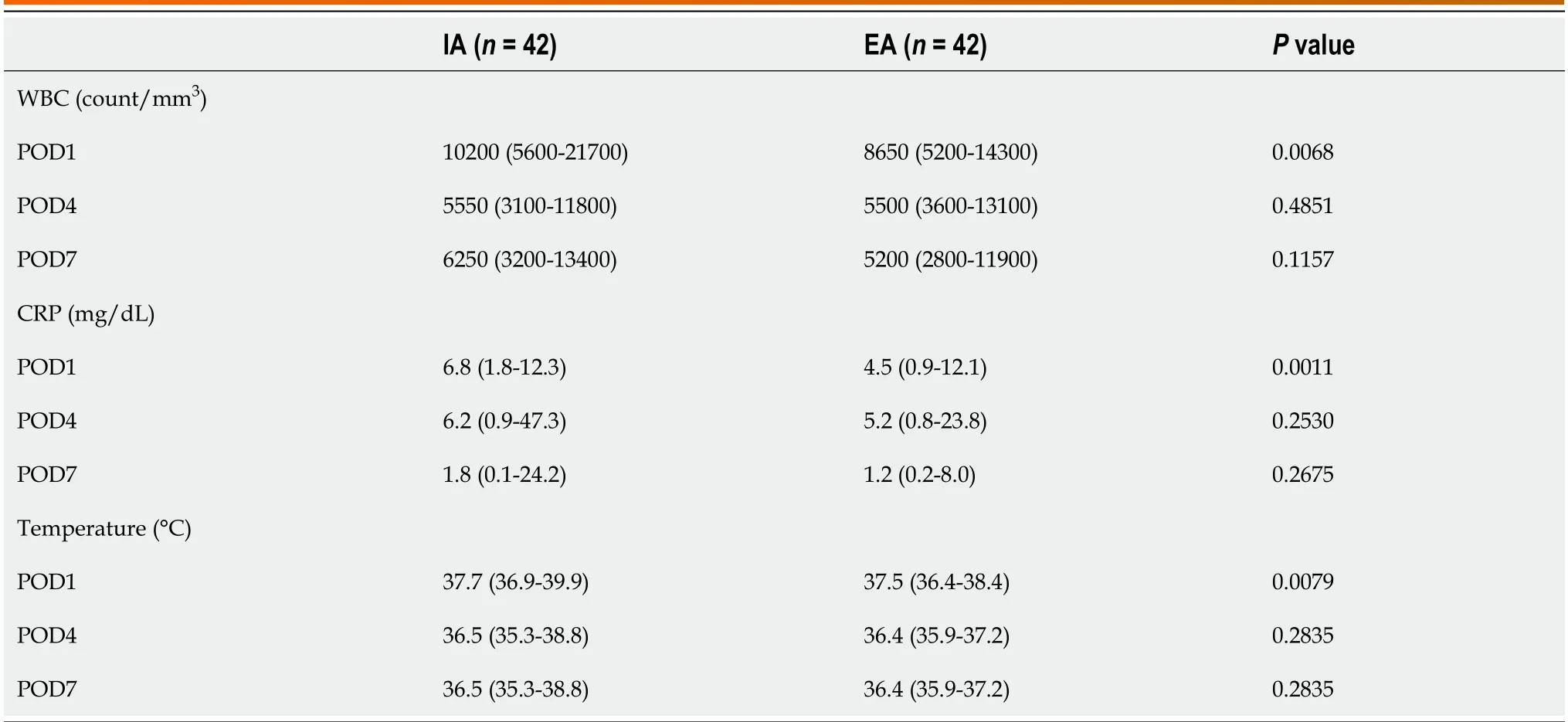
Table 4 Comparison of perioperative systemic inflammatory responses

Table 5 Comparison of adjuvant chemotherapy
Medium-term postoperative outcomes
The medium-term outcomes are shown in Table 6.The median follow-up time was 31.9 months in the IA group and 36.7 months in the EA group.The 3-year OS and 3-year DFS periods for each anastomosis method are shown in Figure 2.

Table 6 Comparison of type of recurrence,n (%)
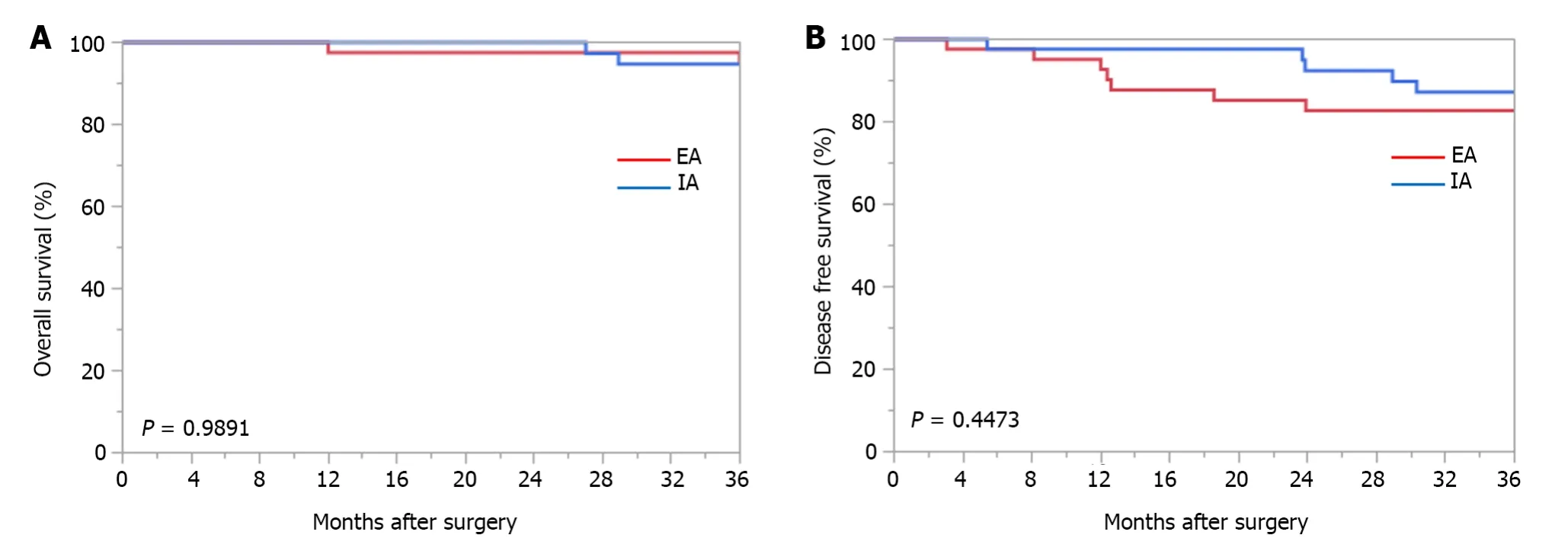
Figure 2 Kaplan-Meier survival curves comparing intracorporeal anastomosis and extracorporeal anastomosis. A: Kaplan-Meier curves comparing 3-year overall survival;B: 3-year disease-free survival.EA: Extracorporeal anastomosis;IA: Intracorporeal anastomosis.
Three-year OS rates were not significantly different between the IA and EA groups (94.7%vs94.7%,respectively;P=0.9891).DFS at 3 years was also not significantly different between the IA and EA groups (87.2%vs82.7%,respectively,P=0.4473).There was no difference between the two groups in the type of recurrence.
DlSCUSSlON
Compared to EA,IA is somewhat more difficult to perform,and the technique of opening the intestinal tract in the abdominal cavity under insufflation may result in bacterial infection and dissemination of tumor cells;therefore,the number of facilities that have introduced IA is limited.
Why dost thou weep, Tsarevitch Ivan? asked the Wolf, and Ivan answered: Gray Wolf, my friend! Why should I not weep and be desolate37? I myself have begun to love Helen the Beautiful, yet now I must give her up to Tsar Afron for the Horse with the Golden Mane. For if I do not, then Tsar Afron will dishonor my name in all countries.
This retrospective study using propensity score matching was performed to examine the two biggest problems in IA for colon cancer with opening the intestinal tract under pneumoperitoneum: (1) Bacterial contamination by spreading stool juices;and (2) peritoneal dissemination by spreading cancer cells.In a comparative study after propensity score matching,there was no difference in operative time as a surgical outcome for IA compared to EA in the present study.Previous studies have not reported a reduction in operative time.Some reports indicate that IA and EA are comparable in terms of operative time[13],but in most reports,IA is longer than EA[14,15],and this applies to robotic surgery[16,17].On the other hand,the amount of bleeding was significantly lower in IA.This means that,in EA,there is bleeding from the mesentery due to forced traction when the intestine is guided out of the body and unintentional bleeding when the mesentery is processed,whereas in IA,there is no forced traction on the mesentery,and the mesentery is processed by energy devices in a qualified manner,resulting in less bleeding.IA also shortened the length of the incision wound.
However,the degree of wound pain remained the same.In the present study,it is assumed that both IA and EA were performed with an open umbilical port wound when removing the diseased intestinal tract,which did not result in a difference in the number of analgesic medications used.Currently,the Pfannenstiel incision is often used in IA to remove the diseased intestinal tract,and this incision causes less wound pain.This incision also results in fewer incisional hernias[18,19].The number of lymph nodes dissected did not differ between IA and EA,but the length of the resected intestine on the anal side was long enough for IA.This indicates that IA is not inferior to EA as a surgical technique for lymph node dissection in cancer treatment because the same number of lymph nodes can be dissected.Furthermore,IA allows for adequate length of the distal resection margin and proper dissection of paracolic lymph nodes,which are prone to lymph node metastasis.In the transverse colon,descending colon,and sigmoid colon,it is difficult to guide the intestinal tract outside the body in EA,so the length of the resected intestinal tract on the anal side tends to be shorter.However,IA has the advantage that the intestinal tract can be separated while maintaining an appropriate distance from the tumor,and the anastomosis can be performed safely.Therefore,in cases involving the left side of the transverse colon to the sigmoid colon,IA may be superior from an oncological standpoint and in terms of the safety of the surgical procedure.
Short-term postoperative results have generally shown that IA is associated with faster recovery of postoperative bowel motility than EA,and the results of the present study were similar[20].IA is a less invasive treatment with theadvantages of less blood loss,shorter incision length,and earlier recovery of bowel motility compared to EA.In terms of postoperative complications,the incidences of anastomotic leakage and SSI did not differ significantly.
The first problem with IA is the degree of bacterial contamination in the abdominal cavity.In the present study,although the difference was not significant,the percentage of positive bacterial cultures was higher for IA than for EA,suggesting that IA has a higher risk for bacterial contamination and that great care should be taken in surgical procedures.Although it has been reported that IA results in lower levels of inflammatory mediators,which are endogenous substances that cause and maintain inflammatory responses in the body,compared to EA[21],as the present study showed,IA generally results in higher postoperative body temperature and blood inflammatory responses.However,there was no difference in organ/space SSIs such as intra-abdominal abscesses,and there was no difference in the number of days on antibiotics to treat infections,indicating that,though bacterial contamination was higher than withEA,no treatment was required.The second problem,the dispersal of cancer cells in the abdominal cavity,is discussed in terms of: (1) The presence of cancer cells in the anastomotic intestinal tract;and (2) the prognostic value of a positive cytological diagnosis.First,it has been previously reported that,in colon cancer,the presence of free cancer cells in the intestinal tract to be anastomosed is as high as 30%-50%[22,23].It has also been reported that the positive rate is higher for open surgery than for laparoscopic surgery.However,it has been reported that free cancer cells were not observed in intestinal tracts longer than 10 cm[23],and if an appropriate length of intestinal tract is taken,it is safe to open the intestinal tract without free cancer cells when performing IA.The presence of free cancer cells may cause anastomotic recurrence and peritoneal dissemination,and IA,which ensures intestinal length compared to EA,may have an oncological advantage.Second,the 5-year survival rate is reported to be worse for patients with cytology-positive colorectal cancer than for patients with cytology-negative colorectal cancer[24,25],and peritoneal recurrence is the most common form of recurrence.In a study of gastric cancer patients,there were reports that the prognosis was better in cases with a high volume of intraperitoneal lavage than in cases with a normal volume of intraperitoneal lavage after radical resection[26],whereas there were also reports that there was no improvement at all[27,28],making it difficult to eliminate the effects of disseminated cancer cells by intraperitoneal lavage.In the present study,ascitic fluid cytology was negative in all cases,and there was no evidence of shedding of free cancer cells from the intestinal tract.In addition,the timing of chemotherapy initiation and completion rates were the same for IA and EA,and the recurrence rate and type of recurrence were the same for IA;thus,the technique of IA is comparable oncologically to that of EA and is not problematic.From the above,the advantages and disadvantages of IA in clinical practice shown in the present study are as follows.In terms of surgical outcomes,the advantages are reduced blood loss,shortened wound length,and the ability to resect anal side intestine while maintaining an accurate anal bowel distance from the tumor and to anastomose safely.The disadvantage,in terms of surgical outcomes,is a longer operative time.In the short-term postoperative results,the advantage is early recovery of postoperative bowel movements,and the disadvantage is an increased inflammatory response.
The limitations of this study are that it was a retrospective study,although propensity score matching was used in the statistical analysis;second,it was a single-center study with a small number of patients;and third,the follow-up period was short (3 years).To overcome these limitations,a multicenter,prospective,observational study should be conducted.
CONCLUSlON
The short-term postoperative results of IA are comparable or superior to those of EA.The medium-term results were oncologically comparable to those of EA,and peritoneal recurrence,which is a concern,was also comparable.The ability to accurately obtain the appropriate length of the resected intestine may be an advantage of IA from an oncological point of view.
ARTlCLE HlGHLlGHTS
Research background
Research motivation
The intraperitoneal bacterial contamination of the abdominal cavity by IA and the resulting perioperative biological reactions,as well as the medium-term oncological outcomes of IA,have not been clarified.
Research objectives
The purpose of this study was to clarify the effects of bacterial and tumor cell contamination of the abdominal cavity in IA.
Research methods
Intracorporeal and extracorporeal anastomoses performed for colon cancer were compared after propensity score matching.
Research results
The 3-year disease-free survival rates did not significantly differ between the IA and extracorporeal anastomosis (EA) groups (87.2%vs82.7%,respectively,P=0.4473).The recurrence rate and type of recurrence also did not differ between the two groups.Furthermore,no significant differences were observed in the incidence of surgical site infection or the number of days on antibiotics,but the postoperative biological response was significantly higher in the IA group.
Research conclusions
The IA method showed the same medium-term results as the conventional EA method;no obvious effects of bacterial or tumor cell dispersal were observed.
Research perspectives
IA is not oncologically problematic and may be a less invasive anastomosis than EA.
ACKNOWLEDGEMENTS
The authors would like to thank Deputy Chief of Medical Clinic,Keitaro Tanaka,Otsu City Hospital,for advice on laparoscopic surgery techniques and study design;and Professor Yasuhiro Kanatani,Department of Clinical Pharmacology,Tokai University School of Medicine,for assistance with statistical analysis of the data.
FOOTNOTES
Author contributions:Kayano H designed the study,analyzed the data,and wrote the paper;Mamuro N,Kamei Y,Ogimi T,and Miyakita H collected the data;Mori M,Nakagohri T,and Koyanagi K supervised this study;and Yamamoto S designed the study and supervised writing of the paper.
lnstitutional review board statement:This study was reviewed and approved by the Ethics Review Committee of the Research Ethics Committee,Tokai University School of Medicine (23RC011).
Conflict-of-interest statement:All authors have no conflict of interest related to the manuscript.
Data sharing statement:The datasets analyzed during the current study are available from the corresponding author on reasonable request.
STROBE statement:The authors have read the STROBE Statement-checklist of items,and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Japan
ORClD number:Hajime Kayano 0000-0002-8304-1136;Hiroshi Miyakita 0000-0001-6541-2944;Toshio Nakagohri 0000-0001-6843-8891;Kazuo Koyanagi 0000-0002-8010-8630.
S-Editor:Yan JP
L-Editor:A
P-Editor:Cai YX
 World Journal of Gastrointestinal Surgery2024年3期
World Journal of Gastrointestinal Surgery2024年3期
- World Journal of Gastrointestinal Surgery的其它文章
- Alcohol associated liver disease and bariatric surgery: Current perspectives and future directions
- Applications of gastric peroral endoscopic myotomy in the treatment of upper gastrointestinal tract disease
- Ex vivo liver resection and auto-transplantation and special systemic therapy in perihilar cholangiocarcinoma treatment
- Rescue from complications after pancreaticoduodenectomies at a low-volume Caribbean center: Value of tailored peri-pancreatectomy protocols
- Comparison of prognosis and postoperative morbidities between standard pancreaticoduodenectomy and the TRlANGLE technique for resectable pancreatic ductal adenocarcinoma
- Analysis of the impact of immunotherapy efficacy and safety in patients with gastric cancer and liver metastasis