
Prevalence,risk factors,and BRAF mutation of colorectal sessile serrated lesions among Vietnamese patients
2024-03-07 04:29NhuThiHanhVuHuyMinhLeDiemThiNgocVoHoangAnhVuNhanQuangLeDungDangQuyHoDucTrongQuach
Nhu Thi Hanh Vu,Huy Minh Le,Diem Thi-Ngoc Vo,Hoang Anh Vu,Nhan Quang Le,Dung Dang Quy Ho,Duc Trong Quach
Abstract BACKGROUND Sessile serrated lesions (SSLs) are considered precancerous colorectal lesions that should be detected and removed to prevent colorectal cancer.Previous studies in Vietnam mainly investigated the adenoma pathway,with limited data on the serrated pathway.AIM To evaluate the prevalence,risk factors,and BRAF mutations of SSLs in the Vietnamese population.METHODS This is a cross-sectional study conducted on patients with lower gastrointestinal symptoms who underwent colonoscopy at a tertiary hospital in Vietnam.SSLs were diagnosed on histopathology according to the 2019 World Health Organization classification.BRAF mutation analysis was performed using the Sanger DNA sequencing method.The multivariate logistic regression model was used to determine SSL-associated factors.RESULTS There were 2489 patients,with a mean age of 52.1 ± 13.1 and a female-to-male ratio of 1:1.1.The prevalence of SSLs was 4.2% [95% confidence interval (CI): 3.5-5.1].In the multivariate analysis,factors significantly associated with SSLs were age ≥ 40 [odds ratio (OR): 3.303;95%CI: 1.607-6.790],male sex (OR: 2.032;95%CI: 1.204-3.429),diabetes mellitus (OR: 2.721;95%CI: 1.551-4.772),and hypertension (OR: 1.650,95%CI: 1.045-2.605).The rate of BRAF mutations in SSLs was 35.5%.CONCLUSION The prevalence of SSLs was 4.2%.BRAF mutations were present in one-third of SSLs.Significant risk factors for SSLs included age ≥ 40,male sex,diabetes mellitus,and hypertension.
Key Words: Colorectal cancer;Sessile serrated lesion;BRAF mutation;Risk factors;Diabetes mellitus;Hypertension
lNTRODUCTlON
Colorectal cancer (CRC) remains the third most prevalent cancer and the second cause of cancer-related mortality worldwide[1].More than 182000 new cases were diagnosed in Vietnam,and 122000 deaths were recorded in 2020[1].For a long time,it was considered that colorectal adenomas were the only precursor lesions for CRC.However,recent studies have indicated that despite a high adenoma detection rate,postcolonoscopy CRC still occurs,with serrated lesions being the most likely cause[2].There is mounting evidence that 15%-30% of all CRCs develop from serrated lesionsviathe serrated neoplasia pathway[3].Furthermore,proximal serrated lesions pose a higher risk of metachronous neoplasia than tubular adenomas,emphasizing the significance of screening and surveillance[4].According to the World Health Organization (WHO) classification 2019,serrated lesions were divided into hyperplastic polyps,sessile serrated lesions(SSLs),SSLs with dysplasia,traditional serrated adenomas,and unclassified serrated adenomas[5].SSLs are the most common and significant precancerous serrated lesions due to their rapid growth and high potential for malignant transformation[6].Nevertheless,SSLs are challenging to detect by colonoscopy due to their typically subtle appearance as flat or sessile lesions and having an overlying mucous cap[7].Moreover,they are often incompletely resected because of the indistinct borders,thus related to interval and synchronous CRC[8].The histopathological identification of SSLs also tends to be difficult for both expert and non-expert pathologists[9].Consequently,the reported prevalence of SSLs varies widely across studies,leading to an underestimation of their prevalence and subsequent biased analysis[10,11].
Studies analyzing risk factors for SSLs have been limited and controversial,primarily due to obstacles posed by their evolving histological definition and the relatively low prevalence of these polyps.In addition,most published data have included all histopathological types of serrated lesions with different malignant progression risks[12].As a result,there were inconsistent findings,and the risk factors for SSLs could not be accurately evaluated.Moreover,existing studies have shown that serrated lesions and adenomas share common risk factors[12,13].Nonetheless,several factors correlated with serrated lesions differently than conventional adenomas[13,14].
In contrast to the conventional pathway,the serrated pathway is characterized by BRAF mutations and a CpG island methylator phenotype with or without microsatellite instability (MSI)[15].Most BRAF mutations in CRC and other tumors are a thymidine-to-adenine transversion at nucleotide 1796,converting a valine at amino acid 600 to glutamic acid(V600E)[16].It has been demonstrated that proximal serrated lesions with BRAF mutations have a considerably high risk for malignant progression[17].Hence,detecting BRAF mutations as an adjunct diagnostic tool in clinical pathology may reliably identify proximal serrated lesions with cancer risk,which require more aggressive therapy and attentive clinical surveillance.Additionally,BRAF mutations may serve as a potential therapeutic target for serrated colorectal neoplasia[18].
In Vietnam,previous research on colorectal polyps has focused heavily on the adenoma pathway,with limited data on the serrated pathway.Despite the importance of SSLs,there remains a paucity of evidence on their prevalence,risk factors,and molecular characteristics.Thus,this study aimed to evaluate the prevalence,risk factors,and BRAF mutations of SSLs in Vietnamese patients.These findings may provide valuable insights into the prevention,early detection,enhancement of treatment,and surveillance approaches for SSLs in the Vietnamese population.
MATERlALS AND METHODS
Study participants
From March 2022 to July 2023,a cross-sectional study was carried out on outpatients over 18 who presented with lower gastrointestinal symptoms and underwent colonoscopy at the University Medical Center at Hochiminh City,Vietnam.Only the first colonoscopy was included if patients received multiple colonoscopies during the study period to ensure a per-patient analysis.Exclusion criteria comprised a history of CRC or colorectal surgery,inflammatory bowel disease,inherited cancer syndromes,coagulation disorders,unqualified bowel preparation according to the Boston Bowel Preparation Scale (BBPS) with a total score of < 6 and each region score of < 2,incomplete colonoscopy,withdrawal time of less than 6 minutes,and not willing to participate in the research.
This study's sample size was determined by applying the following formula:
ThePvalues were chosen based on the prevalence of SSLs and BRAF mutations in previous Asian studies,with 2.6%and 82%,respectively[19,20].The estimated loss of samples would be 10% during the study.Thus,the minimum sample size was 2411 patients.
The demographic,clinical,endoscopic,pathologic,and BRAF mutation data were recorded and evaluated.Smoking conditions were classified as "never," "former," and "current" users.Obesity was defined as having a body mass index equal to or greater than 25.0 kg/m2.Nonalcohol consumption was identified as either never drinking or drinking alcohol once per month or less.Hypertension was diagnosed when systolic blood pressure was ≥ 140 mmHg and/or their diastolic blood pressure was ≥ 90 mmHg or when they were on antihypertensive medication.Patients were classified as having diabetes mellitus (DM) if they fulfilled any of the following criteria: (1) A random venous plasma glucose concentration ≥ 11.1 mmol/L;(2) a fasting plasma glucose concentration ≥ 7.0 mmol/L;(3) HbA1C ≥ 6.5%;and (4) on medication for hyperglycemia with a history of DM.The definition of a family history of CRC was the presence of at least one affected first-degree relative.
All eligible patients signed a written informed consent form.The study protocol was approved by the Board of Ethics in Biomedical Research of the University of Medicine and Pharmacy at Ho Chi Minh City (ID number: 615/HDDDDHYD,signed on November 19,2021).
Colonoscopic procedure
Precolonoscopy bowel preparations were obtained with three liters of polyethylene glycol-based (Fortrans®,Beaufour Ipsen Industrie,France).The colonoscopies were carried out by experienced endoscopists using the Olympus Evis Exera III High Definition CV-190 (Olympus Co.,Ltd,Tokyo,Japan).All participating endoscopists had performed at least 3000 colonoscopic procedures over the last five years and had an adenoma detection rate of over 25%,resulting in highperformance colonoscopies.Moreover,all endoscopists had attended the web-based educational program (CATCH project) to detect flat and depressed colorectal lesions before the commencement of the study[21].In addition,they also participated in a local training session to standardize the examination process and the interpretation of colon lesions suspected as SSLs.
The assessment of bowel preparation quality was conducted utilizing the BBPS.The colon was divided into three sections,including the right colon,transverse colon,and left colon,and each section was scored from 0 to 3.Qualified bowel preparation was defined as a total score of ≥ 6 and each region score of ≥ 2[22].Confirmation of cecal intubation was achieved by identifying the appendiceal orifice,cecal valve,or intubation of the ileum.Stopwatches were used to record withdrawal times,which were mandated at least six minutes after excluding the time required for polypectomies.
The Paris classification was utilized to classify the macroscopic type,including three categories: type 0-I: polypoid (0-Is:sessile,0-Ip: pedunculated),type 0-II: nonpolypoid (0-IIa: slightly elevated,0-IIb: flat,0-IIc: slightly depressed),and type 0-III: excavated[23].The Japan NBI Expert Team (JNET) classification was used to categorize the colorectal lesions by magnifying narrow-band imaging endoscopic findings[24].Type 1 is identified by an invisible vascular pattern and a surface pattern with dark and white spots,resembling the surrounding normal mucosa.Type 2A is defined by its regular surface pattern and vessel pattern,including a regular caliber or distribution.Type 2B is characterized by vessels with variable caliber,irregular distribution,and an irregular or obscure surface pattern.Type 3 is recognized by loose vessel regions,thick vessel disruptions and/or a surface pattern of amorphous areas.The proximal colon included the cecum,ascending colon,hepatic flexure,and transverse colon.The distal colon included the splenic flexure,descending colon,sigmoid colon,and rectum.The size of the lesions was measured by comparing them with open (with a width of 7 mm)or closed (equivalent to 3 mm) biopsy forceps or polypectomy snares of known diameters.Multiple polyps were identified as having at least two lesions.The most advanced or largest lesion was considered for the primary diagnosis in subjects with multiple lesions.All detected polyps were removed and obtained for histopathological evaluation.
Histopathological analysis
All resected lesions were collected in distinct jars and preserved in 10% formalin.Sections were cut at 4 μm thickness and stained with hematoxylin-eosin.Serrated lesions were classified in accordance with the updated WHO 2019 criteria[5].The presence of a single unequivocally distorted crypt was regarded as a diagnostic criterion for SSL.An obviously distorted serrated crypt had at least one of the following histologic characteristics: (1) Horizontally growing crypt along the muscularis mucosa (L-shaped or inverted T-shaped crypt);(2) crypt base dilation,comprising the basal one-third of the crypt;(3) serrations that extend into the crypt base;and (4) asymmetrical expansion of the crypts.SSLs with dysplasia were subclassified into SSLs with dysplasia.The dysplastic component is identified as clearly separated from the SSL with architectural modifications,including the presence of villous architecture,elongated crypts,crowded crypts with complicated branching,cribriforming,and excessive or diminished luminal serration compared with the background SSL[5].Cells may exhibit intestinal dysplasia similar to that observed in conventional adenomas;serrated dysplasia with round atypical nuclei,large nucleoli,multiple mitoses,and eosinophilic cytoplasm;or (less frequently) subtle cytological atypia,including hypermucinous alterations.Stratification of dysplasia into low-grade and high-grade is not applicable in this study.All histopathological diagnoses were made by two experienced gastrointestinal pathologists.Any disagreements were discussed to achieve a consensus.
BRAF mutation analysis
BRAF mutation analysis was conducted on all specimens diagnosed with SSLs using Sanger sequencing at the Center for Molecular Biomedicine,University of Medicine and Pharmacy at Ho Chi Minh City.The ReliaPrep FFPE gDNA Miniprep System Kit (Promega,Madison,WI,USA) was used to extract genomic DNA from formalin-fixed paraffin-embedded tissues according to the manufacturer's protocol.Exon 15 of BRAF was amplified utilising TaKaRa Taq HotStart Polymerase (Takara Bio,Shiga,Japan) with a primer pair (forward: 5’-ACTCTTCATAATGCTTGCTC-3’ and reverse: 5’-CCACAAAATGGATCCAGACA-3’).Following purification with ExoSAP-IT reagent (Thermo Fisher,Scientific,Waltham,MA,United States),the products of the polymerase chain reaction were sequenced in both the sense and antisense directions using an ABI 3500 Genetic Analyser (Applied Biosystems,Foster City,CA,United States) and the BigDye Terminator v3.1 Kit.SeqScape Software version 2.6 (Thermo Fisher,Scientific,Waltham,MA,USA) was utilised to analyse mutations.
Statistical analysis
All statistical analyses were performed using SPSS software version 23 (SPSS Inc.,Chicago,IL).The Kolmogorov-Smirnov test was used to determine the normality of continuous variables.The t-test was utilized to compare variables that followed a normal distribution and were presented as the mean and standard deviation (SD).Those with a nonnormal distribution were reported as the median (upper and lower quartiles) and compared using the Mann-Whitney U test.The categorical variables were compared using Pearson's chi-squared test and presented as numbers and percentages.The prevalence was estimated by dividing the proportion of colonoscopies containing at least one SSL by the total number of performed colonoscopies.The prevalence and risk factors for SSLs were determined on a per-patient basis.In addition,the data were analyzed per lesion to determine the characteristics of SSLs and BRAF mutations.The SSL patient group was compared to the control group,with no polyps detected.Univariate analyses were conducted in order to evaluate the factors correlated with SSLs.Variables with aPvalue of 0.2 or less were included in a multivariate logistic regression model.AllPvalues of less than 0.05 were considered statistically significant.
RESULTS
Characteristics of participants
There were 2706 patients with lower gastrointestinal symptoms who were referred for colonoscopy.Among them,2590 participants met the inclusion criteria and underwent colonoscopy.We excluded 101 cases due to incomplete colonoscopy,unqualified bowel preparation,and withdrawal time of less than 6 min.As a result,a total of 2489 patients were included in the analysis (Figure 1).
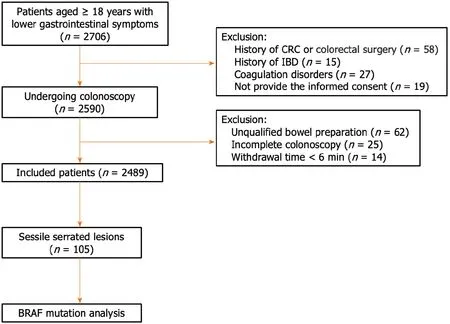
Figure 1 Flow chart of participant recruitment. CRC: Colorectal cancer;IBD: Inflammatory bowel disease.
The main indications for colonoscopy were abdominal pain (62.4%),diarrhea (51%),constipation (29.2%),and hematochezia (13.8%).The mean age of the participants was 52.1 ± 13.1 (range: 19-87 years).The female-to-male ratio was 1:1.1.
Prevalence and risk factors for SSLs
There were 1009 participants with at least one colorectal polyp (40.5%).A total of 121 specimens from 105 patients were histopathologically confirmed to have SSLs,with a prevalence of 4.2% [95% confidence interval (CI): 3.5-5.1].The demographic and clinical features of the SSL patients are presented in Table 1.The mean age of the SSL patients was 57.6± 12 years,ranging from 21 to 84 years,and 91.4% were over 40 years.Male patients accounted for a larger proportion,with 61% of all cases.There was a remarkable trend in the prevalence of SSLs with increasing age.The SSL prevalence in patients under 40 was only 8.6%;meanwhile,this prevalence increased to 33.3% and 44.8% in those aged 50 to 59 years and those aged ≥ 60,respectively.
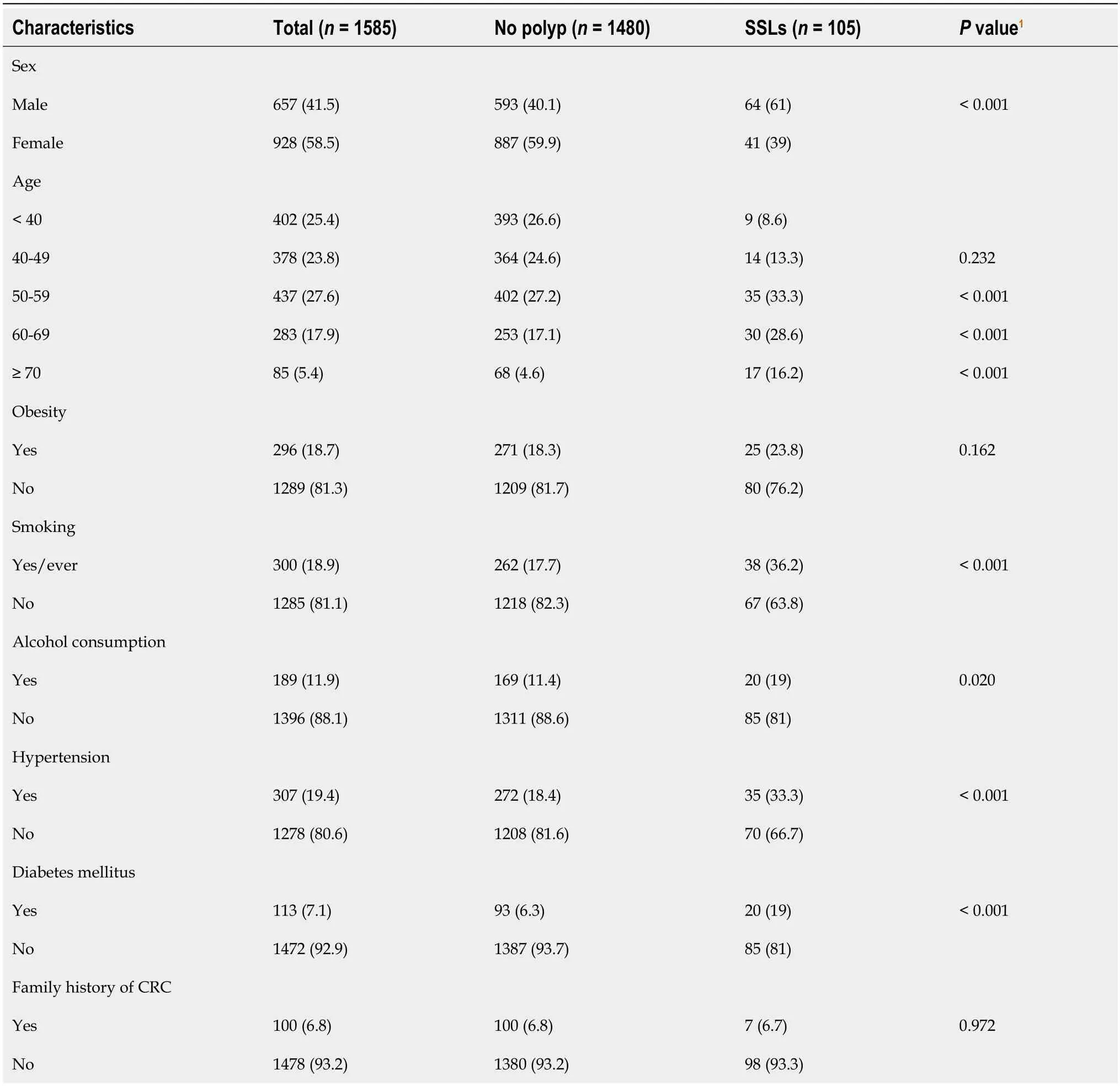
Table 1 Characteristics of participants,n (%)
In the per-patient univariate analysis,age ≥ 40,male sex,current or ex-smokers,DM,and hypertension were significantly related to SSLs (Table 1).Table 2 displays the results of the multivariate logistic regression models.The factors significantly associated with SSLs in the multivariate model were age ≥ 40 (odds ratio [OR]: 3.303;95%CI: 1.607-6.790;P=0.001),male sex (OR: 2.032;95%CI: 1.204-3.429;P=0.008),DM (OR: 2.721;95%CI: 1.551-4.772;P< 0.001),and hypertension (OR: 1.650;95%CI: 1.045-2.605;P=0.031).

Table 2 Univariable and multivariable logistic regression analysis of factors associated with sessile serrated lesions
Characteristics of SSLs
A total of 121 Lesions from 105 patients were diagnosed with SSLs.There were 90 patients (85.7%) who had one SSL,and 15 patients had two SSLs (14.3%).The mean size of the SSLs was 8.8 ± 4.8 mm.Endoscopic features of SSLs are described in Table 3.
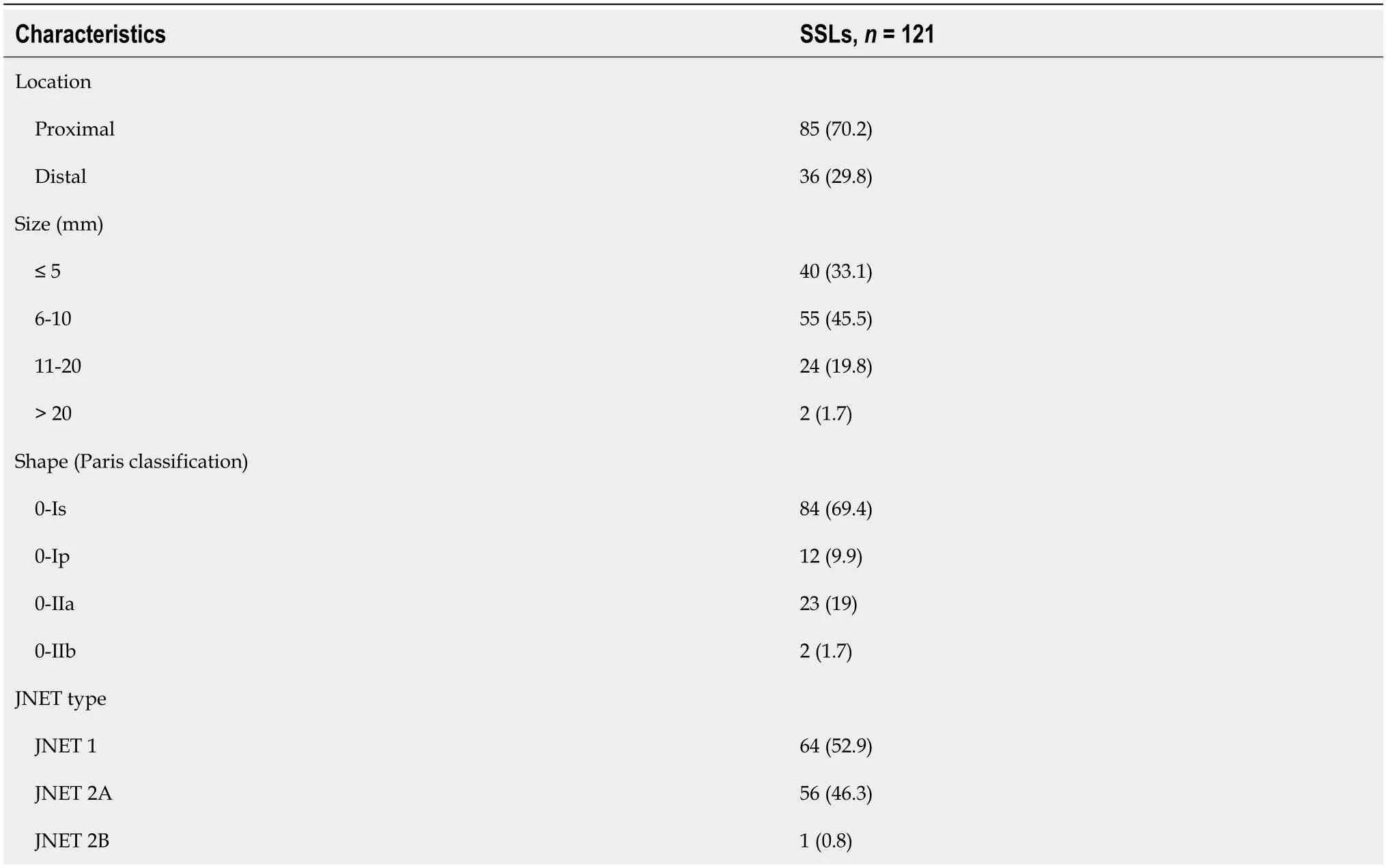
Table 3 Endoscopic characteristics of sessile serrated lesions,n (%)
BRAF mutations and related factors in SSLs
BRAF mutations were observed in 43 (35.5%) out of 121 Lesions from patients diagnosed with SSLs.The majority were V600E,amounting to 95.3%,while the others were D594N and K601E.Risk factors correlated with BRAF mutations are described in Table 4.Male patients comprised 55.1% of the SSL group without BRAF mutations and 62.8% of those with BRAF mutations;this difference was not statistically significant (P=0.410).In univariate analysis,age less than 60 years old and SSLs without dysplasia were correlated with BRAF mutations (P< 0.05).However,multivariate analysis indicated no risk factors with statistically significant differences.

Table 4 Univariable and multivariable logistic regression analysis of factors associated with BRAF mutation in sessile serrated lesions
DlSCUSSlON
To the best of our knowledge,this is the first study evaluating the prevalence,related factors,and BRAF mutations for SSLs among Vietnamese individuals.The prevalence of SSLs has shown considerable heterogeneity across various investigations,with reported rates ranging from 1% to 14%[25-27].According to a recent systematic analysis,SSL prevalence varied by region,with rates of 2.6% in Asia,3.9% in Europe,5.1% in the United States,and 10.5% in Australia[19].The differences in patient demographics,ethnicity,colonoscopy qualities,pathology criteria,and interobserver variability among endoscopists and pathologists may explain these discrepancies[19,28,29].Our findings indicated that the prevalence rate of SSLs was 4.2%,which was higher than that in most previous studies conducted in Asia.This discrepancy can be partly explained by several reasons.First,the research subjects in most previous studies in Asia screened asymptomatic participants,while our study was on patients with lower gastrointestinal symptoms.Second,pathological diagnostic criteria for SSLs in other Asian studies applied the old WHO classification,which might lower the prevalence of SSLs.The old WHO classification for the diagnosis of SSLs necessitated the presence of two to threedistorted serrated crypts[30].In contrast,the recent WHO criteria 2019 have been revised to require just one distorted serrated crypt for SSL diagnosis[5].Third,in some studies,only one pathologist was responsible for interpreting the results.In our study,all lesions were assessed by two experienced gastrointestinal pathologists using the WHO criteria 2019 to minimize interobserver variation and increase diagnostic accuracy.Fourth,the participating endoscopists in our study also received training in recognizing SSLs prior to the commencement of the investigation.It is anticipated that the elements mentioned above might contribute to our investigation's enhanced precision of SSL prevalence.
Our data revealed that age ≥ 40,male sex,DM,and hypertension were independent risk factors for SSLs.Prior studies also concluded that older age was a risk factor for SSLs.However,the age cutoff in these studies was higher than in our analysis,with cutoffs over 50 or 60 years old[13,25,31].These observed disparities could be attributed to our study participants having a lower mean age and gastrointestinal symptoms.As early-onset CRC (i.e.,< 50 years of age) is prevalent in Vietnam,colonoscopy is generally considered in Vietnamese patients with lower gastrointestinal symptoms at a lower threshold of age,as recommended by the Asia-Pacific consensus recommendations for CRC screening[32].One previous study in Vietnamese reported a significantly high proportion of early-onset CRC (i.e.,< 50 years of age) of 28%,of which 11% of patients were under 40[33].Nonetheless,it remains controversial that several studies have found no association between age and SSLs[26,34,35].Meesteret al[19] conducted a systematic review and reported that SSL prevalence increased with age.Nevertheless,the relationship was smaller than that for adenomas and did not reach statistical significance.Therefore,additional research is needed to ascertain the connection between age and the formation of SSLs,especially in the Vietnamese population.
There have been conflicting results about the relationship between gender and SSLs.Some research revealed no differences based on sex[12,27,35],whereas others showed an association between SSLs and female sex[36].In our study,male sex increased the odds of SSLs.In a recent meta-analysis,males also had a higher rate of serrated lesions than females,and estrogen or hormone replacement therapy may reduce the risk of CRC and serrated lesions[37].One clinical trial found a reduction of 40% in the risk of CRC in postmenopausal women receiving hormone replacement therapy,which may contribute to a decreased risk of serrated lesions[38].
The association between DM and the development of CRC and conventional adenomas has been established in previous research[39,40].In addition,there is a correlation between the usage of diabetes drugs and CRC.Metformin use has been shown in recent meta-analyses to significantly reduce the incidence of CRC,and improve CRC outcomes[41,42].Conversely,hyperinsulinemia is hypothesized to stimulate the development and proliferation of cells[43].The relationship between insulin therapy and cancer growth is biologically connectedviahyperinsulinemia.One metaanalysis of observational studies suggested that insulin therapy might increase the risk of CRC[44].However,additional prospective cohort studies with extended follow-up periods are necessary to validate this correlation.Regarding the relationship between DM and SSLs,limited data have addressed this matter.Luiet al[13] provided evidence that DM increased the risk of developing SSLs in the screening population aged 50-70.Burnett-Hartmanet al[45] included symptomatic patients,and DM was considered a risk factor for SSLs.These findings were consistent with our results.Nevertheless,Macarieet al[46] demonstrated that DM was unrelated to SSLs,although hypertension and obesity were statistically associated with SSL development.Hence,the association between DM and SSLs remains unclear.Further investigations should be carried out to clarify this issue.
Limited studies have evaluated the relationship between hypertension and SSL patients,and the results were inconsistent.Our results indicated that hypertension was statistically associated with SSLs.This finding was also reported by a case-control study conducted in Romania[46].One study in Korea also showed that SSLs with dysplasia/carcinoma were significantly associated with metabolic diseases,including hypertension,type 2 DM,and dyslipidemia[47].In contrast,two studies in the Chinese population found no association between hypertension and SSLs[13].Therefore,this is a crucial issue that needs to be further investigated.
The most prominent critical feature in the initial phase of the serrated neoplastic pathway is a mutation in the BRAF proto-oncogene,which activates the mitogen-activated protein kinase (MAPK) cascade.This BRAF mutation leads to uncontrolled cell proliferation,similar to the KRAS mutation in adenomas[17].The incidence of BRAF mutations has been reported in 50%-72% of microvesicular hyperplastic polyps,70%-80% of SSLs,and only 1% of tubular adenomas[48].However,there have been differences in BRAF mutation rates in Eastern and Western countries.Based on data from Western countries,the prevalence of BRAF mutations in SSLs ranges from 63% to 100%[17,49-53],which is higher than that in East Asian nations,with reported rates ranging from 14% to 86%[54-58].In our study,the percentage of BRAF mutations was 35.5%.These dissimilarities indicated that BRAF mutations in SSLs may depend on ethnicity,lifestyle,and diet.Moreover,BRAF mutations may not be a significant molecular feature of the serrated neoplasia pathway in a subset of Eastern populations,as in Western populations.The low frequency of BRAF mutations in SSLs in Asia may also partially explain the low prevalence of SSLs compared to Western countries.Furthermore,our results reported no statistically significant association with age,sex,endoscopic,or pathologic factors.More future studies will be needed to better investigate the molecular characteristics of SSLs in the Vietnamese population.
This study has several limitations.First,this is a single-center study.Second,some potential risk factors,such as dietary habits,dyslipidemia,and medication histories,have not been investigated.Third,the study participants were symptomatic patients undergoing colonoscopy.These limitations could limit the generalizability of the study findings.Fourth,the available data about diabetes duration and therapy used in the patients with DM in our study are insufficient and constrained.Therefore,we could not analyze these data in our manuscript.
CONCLUSlON
In conclusion,we reported for the first time a prevalence of SSLs of 4.2% in Vietnamese patients with lower gastrointestinal symptoms undergoing colonoscopy.Male sex,age ≥ 40,DM,and hypertension were independent factors associated with SSLs.The rate of BRAF mutations in patients with SSLs was 35.5%.Further investigations are needed to identify the role of BRAF mutations in the Vietnamese population.
ARTlCLE HlGHLlGHTS
Research background
Sessile serrated lesions (SSLs) are precancerous colorectal lesions that should be identified and removed to prevent colorectal cancer.However,previous research in Vietnam mainly focused on the adenoma pathway,with limited information on the serrated pathway.
Research motivation
The reported prevalence of SSLs varies widely across studies,leading to underestimating their prevalence and biased analysis.Moreover,studies analyzing risk factors for SSLs have been limited and controversial.Furthermore,BRAF mutations may be a potential therapeutic target in serrated colorectal neoplasia.
Research objectives
Our study aimed to evaluate the prevalence,risk factors,and BRAF mutations of SSLs in Vietnamese patients.These findings may provide valuable insights into the prevention,early detection,treatment improvement,and surveillance approaches for SSLs in the Vietnamese population.
Research methods
This is a cross-sectional study carried out on patients with lower gastrointestinal symptoms who underwent colonoscopy at the University Medical Center at Ho Chi Minh City,Vietnam.SSLs were diagnosed on histopathology according to the updated 2019 WHO classification.BRAF mutation analysis was performed using the Sanger DNA sequencing method.Univariate and multivariate logistic regression analyses were used to determine SSL-associated factors.
Research results
There were 2489 patients were included in the analysis,with a mean age of 52.1 ± 13.1 and a female-to-male ratio of 1:1.1.A total of 121 specimens from 105 patients were histopathologically confirmed to have SSLs,with a prevalence of 4.2%[95% confidence interval (CI): 3.5-5.1].The factors significantly associated with SSLs in the multivariate model were age ≥40 [odds ratio (OR): 3.303;95%CI: 1.607-6.790;P=0.001],male sex (OR: 2.032;95%CI: 1.204-3.429;P=0.008),diabetes mellitus (OR: 2.721;95%CI: 1.551-4.772;P< 0.001),and hypertension (OR: 1.650;95%CI: 1.045-2.605;P=0.031).The rate of BRAF mutations in SSLs was 35.5%.
Research conclusions
We reported for the first time a prevalence of SSLs in Vietnamese patients with lower gastrointestinal symptoms.Our data revealed that age ≥ 40,male sex,diabetes mellitus,and hypertension were independent risk factors for SSLs.Additional investigations are needed to ascertain the connection between these risk factors and SSLs,especially in the Vietnamese population.
Research perspectives
It is crucial to conduct multicenter,prospective,and follow-up studies to determine the prevalence,risk factors,and molecular characteristics of SSLs,especially in the Vietnamese population.
ACKNOWLEDGEMENTS
The authors would like to thank Drs.Truc Le Thanh Tran,Mai Ngoc Luu,Quang Dinh Le,Doan Thi Nha Nguyen,and Vy Ly Thao Tran at the University of Medicine and Pharmacy at Ho Chi Minh City and the University Medical Center at Ho Chi Minh City for their support.
FOOTNOTES
Author contributions:Quach DT contributed to the study’s conception;Vu NTH,Le NQ,Le HM,Vo DTN,and Vu HA conducted data curation;Vu NTH,and Quach DT performed data analysis;Ho DDQ,Quach DT,Le NQ,and Le HM provided supervision for the study;Vu NTH,Quach DT,and Vu HA drafted the initial manuscript;Ho DDQ,Vo DTN,Quach DT,Le HM,Le NQ,and Vu HA reviewed and edited the manuscript.
lnstitutional review board statement:The study was approved by the Board of Ethics in Biomedical Research of the University of Medicine and Pharmacy at Ho Chi Minh City (ID number: 615/HDDD-DHYD,signed on November 19,2021).
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:We have no financial relationships to disclose.
Data sharing statement:No additional data are available.
STROBE statement:The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Viet Nam
ORClD number:Nhu Thi Hanh Vu 0000-0003-4208-7813;Duc Trong Quach 0000-0003-0141-921X.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Zhang XD
 World Journal of Clinical Oncology2024年2期
World Journal of Clinical Oncology2024年2期
- World Journal of Clinical Oncology的其它文章
- Unlocking the potential-vitamin D in prostate cancer prevention
- Updates on management of gliomas in the molecular age
- Deregulation of interferon-gamma receptor 1 expression and its implications for lung adenocarcinoma progression
- Elucidating the molecular basis of ATP-induced cell death in breast cancer: Construction of a robust prognostic model
- ldentification of immune cell-related prognostic genes characterized by a distinct microenvironment in hepatocellular carcinoma
- Population-based X-ray gastric cancer screening in Hiroshima prefecture,Japan