
Updates on management of gliomas in the molecular age
2024-03-07 04:29AliAhmedMohamedRakanAlshaibiStevenFaragallaYoussefMohamedBrandonLuckeWold
Ali Ahmed Mohamed,Rakan Alshaibi,Steven Faragalla,Youssef Mohamed,Brandon Lucke-Wold
Abstract Gliomas are primary brain tumors derived from glial cells of the central nervous system,afflicting both adults and children with distinct characteristics and therapeutic challenges.Recent developments have ushered in novel clinical and molecular prognostic factors,reshaping treatment paradigms based on classification and grading,determined by histological attributes and cellular lineage.This review article delves into the diverse treatment modalities tailored to the specific grades and molecular classifications of gliomas that are currently being discussed and used clinically in the year 2023.For adults,the therapeutic triad typically consists of surgical resection,chemotherapy,and radiotherapy.In contrast,pediatric gliomas,due to their diversity,require a more tailored approach.Although complete tumor excision can be curative based on the location and grade of the glioma,certain non-resectable cases demand a chemotherapy approach usually involving,vincristine and carboplatin.Additionally,if surgery or chemotherapy strategies are unsuccessful,Vinblastine can be used.Despite recent advancements in treatment methodologies,there remains a need of exploration in the literature,particularly concerning the efficacy of treatment regimens for isocitrate dehydrogenase type mutant astrocytomas and fine-tuned therapeutic approaches tailored for pediatric cohorts.This review article explores into the therapeutic modalities employed for both adult and pediatric gliomas in the context of their molecular classification.
Key Words: Gliomas;Chemotherapy;Radiotherapy;Isocitrate dehydrogenase type mutant;Pediatric gliomas;Astrocytoma;Oligodendroglioma;1p/19q-codeleted
lNTRODUCTlON
Gliomas,a diverse group of primary brain tumors arising from glial cells,continue to pose formidable challenges in the field of oncology.They account for the overarching majority of adult brain tumors,making it critical to achieve proper management and better prognoses.The World Health Organization (WHO) classifies gliomas based on histology,grade,and molecular information,with the primary focus being molecular markers that govern treatment plans and expected outcomes[1,2].The broad spectrum encapsulated by gliomas range from low-grade tumors with relatively favorable prognoses to highly aggressive and invariably fatal high-grade glioblastomas.In previous decades,limited therapeutic options existed,disposing patients to a bleak prognosis.However,recent years have seen a surge in academic efforts,leading to a deeper understanding of the molecular and genetic underpinnings of gliomas.
The current trident approach to glioma treatment of surgery,radiotherapy,and chemotherapy has significantly benefited from molecular diagnostic tools that provide providers with advanced tools for both diagnosis and targeted treatment of patients[3].Since recurrent gliomas can occur due to neural stem-cell regeneration of tumors after surgical resection,treatments have become geared towards the molecular suppression of such cells[4].This is increasingly important as prognosis is often highly dependent on the molecular make-up of the tumor.For instance,isocitrate dehydrogenase type (IDH) mutations and 1p/19q codeletions have been associated with lower-grade gliomas,while CDKN2A/B deletions suggest a more disadvantageous prognosis[5-7].The specific significance of molecular markers will change as a patient ages,as the aforementioned factors become more sparse in an advanced age population.Other valuable measures,such as the positive prognostic factor of O6-methylguanine-DNA methyltransferase (MGMT),are noted in this older population[8].
With an increasing ability to further identify and classify tumors,advancements in molecular genetics offer a path to better prognosis for many patients.This review article addresses the current state of management for gliomas,focusing on tailored treatment modalities which aim to maximize lifespan and quality of life.
OPERATlVE TREATMENT
In resectable tumors,surgical advancements have established a maximal safe resection model,removing more nonenhancing residual volume of gliomas rather than previous models of gross resection of contrast-enhancing areas(Figure 1)[9,10].Intra-operative ultrasound,in combination with neuronavigation,has provided better residual tumor margin control[11].The management of recurrent malignancies near the resection site has seen improvement with the approval of the surgically targeted radiation therapy GammaTile,utilizing it in combination with standard-of-care external beam radiation therapy to decrease the likelihood of recurrence[12,13].These measures,with the help of molecular identification of each tumor,have increased patient survival and developed a better algorithm for resection strategy.Not merely addressing the quantity of survival years,the quality of patient survival is at the forefront of studies using real-time brain stimulation mapping to preserve cognitive functions intra-operatively.This is done through the association of intra-operative tasks with specific brain functions.With awake craniotomies,decreased neural deficits have been observed,yielding higher preservation of motor and language functions[14,15].More advanced stimulation mapping techniques aim to maintain higher order functions post-operatively.Administration of the Stroop color-word task,related to executive function,during resections has been associated with a reduction in post-operative executive function deficits[16].
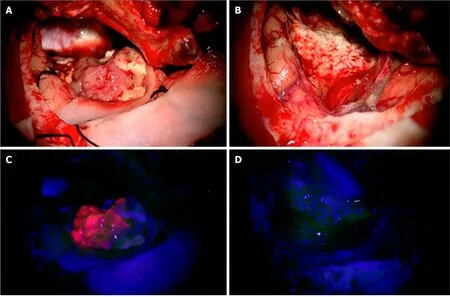
Figure 1 A 61-year-old patient with a left temporal glioblastoma. A and B: The upper row shows the operative field in white light prior to (A) and after (B)tumor resection.C and D: The lower row shows the corresponding fluorescence images.Citation: Sales AHA,Beck J,Schnell O,Fung C,Meyer B,Gempt J.Surgical Treatment of Glioblastoma: State-of-the-Art and Future Trends.J Clin Med 2022;11: 5354.Copyright ©2022 The Authors.Published by MDPI (Basel,Switzerland)[19] (Supplementary material).
The overall surgical management has shifted to rely more heavily on the molecular biomarkers of each glioma.Recommendations seeing the best outcomes suggest gross total resection with aggressive margin control of low-grade diffuse gliomas with wild-type IDH,with only subtotal resection for diffuse gliomas with mutated IDH[17].In anaplastic gliomas,wild-type IDH tumors are conservatively treated with enhancing tissue resection,while those with mutant IDH can either be treated by total gross resection if they do not possess a 1p/19q codeletion or a subtotal resection if a 1p/19q codeletion exists in a functional area[17,18,19].
ADULT GLlOMAS
Following neurosurgical intervention,radiotherapy and chemotherapy are commonly employed.These postoperative therapies are administered as appropriate based on tumor type,WHO grade,and molecular features.
WHO grade 2
WHO classified grade 2 adult gliomas are defined as slow growing tumors that are locally infiltrative in middle-aged and young adults[20,21].Referred commonly as low-grade gliomas (LGG),these tumors typically progress to more aggressive subtypes and present a poor prognosis,especially in older patients[22].The two tumors in this class include IDH-mutant astrocytomas,and IDH-mutant,1p/19q-codeleted oligodendrogliomas.
IDH-mutant astrocytoma:Following gross total resection by neurosurgical intervention,patients without a history of seizures and young patients can be cautiously managed with a watch-and-wait policy.Patients with a history or propensity to develop seizures and patients older than 40 years may benefit from early radiotherapy.Although early radiotherapy does not seem to improve overall survival in patients,it has been shown to improve seizure control and progression-free survival[23].Typical dose ranging of radiotherapy is 45 to 50 Gy.No observable improvements have been demonstrated with high doses of 60 Gy and there is a concern of radiation-induced neurological implications in patients with long-term survival expectations[24,25].The addition of chemotherapy with radiotherpay demonstrates superior progression-free survival when compared to chemotherapy alone[26].However,patients intolerant to radiotherapy can benefit from the sole administration of chemotheraoy with temozolomide (TMZ).Younger patients between the ages of 13 and 39,and older patients over the age of 40 demonstrated a 4 to 5 year increase in overall survival when treated with postoperative radiotherapy and a chemotherapy regimen consistent of procarbazine,lomustine,and vincristine (PCV) for high risk gliomas[27].
IDH-mutant,1p/19q-codeleted oligodendroglioma:Management of IDH-mutant,1p/19q-codeleted oligodendrogliomas(Figure 2) is consistent with what has been described for IDH-mutant astrocytomas with few exceptions.It is unclear if progression-free survival is impacted in patients who receive chemotherapy alone when compared to patients who receive chemotherapy in addition to radiotherapy[28].Although typical practice is to incorporate radiotherapy with chemotherapy treatment,further investigation is required to determine their independent effects on patient outcomes.
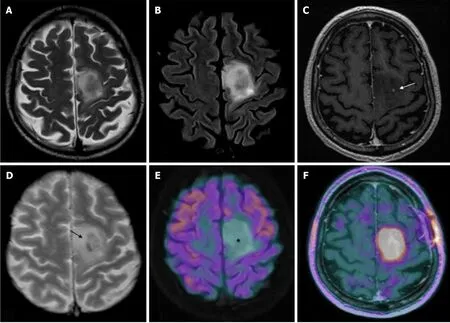
Figure 2 Magnetic resonance imaging and positron emission tomography characteristics of a diffuse isocitrate dehydrogenase mutated 1p/19q codeleted glioma (oligodendroglioma grade 2). A-F: T2w fast spin echo (A),T2w FLAIR (B),T1w fast spin echo contrast-enhanced (C),T2*-weighted gradient echo (D),18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)/magnetic resonance imaging (MRI) (E),and dihydroxyphenylalanine(DOPA)-PET/MRI (F) images are shown;C-F: Mesial frontal mass with a low mass effect and without any significant enhancements after contrast (arrow in C indicates the only spot of blood-brain barrier leakage),and some intratumoral calcifications (arrow in D;computed tomography not shown) with no significant radiotracer uptake by FDG-PET [asterisk in E,but showing a lively uptake of the PET-DOPA radiotracer (F)].Citation: Feraco P,Franciosi R,Picori L,Scalorbi F,Gagliardo C.Conventional MRI-Derived Biomarkers of Adult-Type Diffuse Glioma Molecular Subtypes: A Comprehensive Review.Biomedicines 2022;10: 2490.Copyright ©2022 The Authors.Published by MDPI (Basel,Switzerland)[28] (Supplementary material).
WHO grade 3
WHO classified grade 3 adult gliomas,also known as anaplastic gliomas,are malignant tumors that have a median age of diagnosis ranging from 35 to 55.5 years based on the displayed mutations[29].Tumors in this class include IDH-mutant astrocytomas,and IDH-mutant,1p/19q-codeleted oligodendrogliomas.
IDH-mutant astrocytoma:As described in WHO classified grade 2 gliomas,radiotherapy is a typical recommendation following gross total resection of grade 3 gliomas as well.Patients with IDH-mutant astrocytoma (Figure 3) receiving radiotherapy with adjuvant TMZ have demonstrated improved survival when compared to patients receiving concurrent TMZ with radiotherapy or radiotherapy alone[30,31].Appropriate radiotherapy dose for these tumors is 60 Gy.
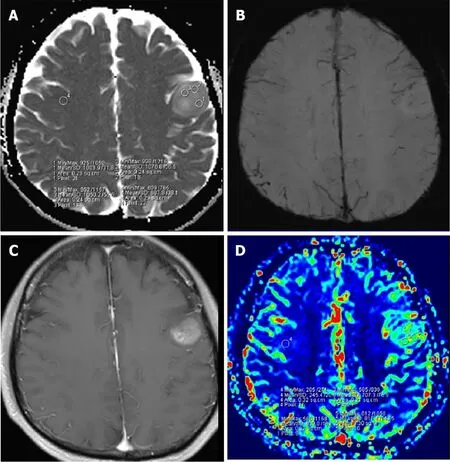
Figure 3 A 53-year-old woman with grade 3 isocitrate dehydrogenase-mutant astrocytoma. A: Apparent diffusion coefficient (ADC) map shows an increased ADC value in the lesion (ADCmin=1.016 × 10-3 mm2/s);B: Susceptibility weighted imaging shows obvious ITSS in the left parietal region;C: Post-contrast T1WI demonstrates a nonenhancing lesion;D: relative cerebral blood volume (rCBV) map shows the rCBVmax value of 1.19.Citation: Yang X,Xing Z,She D,Lin Y,Zhang H,Su Y,Cao D.Grading of IDH-mutant astrocytoma using diffusion,susceptibility and perfusion-weighted imaging.BMC Med Imaging 2022;22: 105.Copyright ©2022 The Authors.Published by BioMed Central Ltd[31] (Supplementary material).
IDH-mutant,1p/19q-codeleted oligodendroglioma:Following the response to treatment trend seen in the discussed tumors,radiotherapy remains to be highly indicated following surgery.Patients with IDH-mutant,1p/19q-codeleted oligodendrogliomas have not demonstrated an improvement in survival with the administration of PCV or TMZ without prior radiotherapy[32].However,an absolute survival benefit of 5 to 6 years has been demonstrated by postoperative radiotherapy and a chemotherapy regimen consistent of PCV[33,34].This combined therapeutic approach also demonstrated improved overall survival when compared to postoperative radiotherapy alone.As with IDH-mutant astrocytomas,a radiotherapy dose of 60 Gy is appropriate.
The response demonstrated following the administration of these different protocols suggest that the best management is achieved with gross total resection followed by radiotherapy and a chemotherapy regimen of PCV.A current trial is underway to determine if TMZ can be used to replace a chemotherapy regimen of PCV as it has demonstrated mild myelosuppression and thus,a superior safety profile[35,36].
WHO grade 4
WHO classified grade 4 adult gliomas constitue both the most aggressive and most common primary malignancies of the brain.Grade 4 gliomas are recognized as highly heterogenous because of the variability in tumor size,histopathology,and molecular characteristics[37].Tumors of this class have a 5-year survival rate of 5 to 10% and include IDH-mutant astrocytomas and IDH-wildtype glioblastoma.
IDH-mutant astrocytoma (previously: IDH-mutant glioblastoma):IDH-mutant astrocytoma constitutes a newly defined type of grade 4 glioma by the WHO in 2021[38,39].This type of glioma has a favorable diagnosis compared to IDHwildtype glioblastoma and is related to young age and dedifferentiation of a prior low grade gliomas (WHO grade 1 and 2)[40].Treatment recommendation is consistent with previous management guidelines prior to its establishment as its own type of grade 4 glioma because of a lack of independent research on treatment efficacy specific to IDH-mutant astrocytoma.Landmark studies identifying treatment options for IDH-wildtype glioblastoma included IDH-mutant astrocytoma within their investigations[36].Thus,further studies assessing independent efficacy of treatment on this newly classified type of grade 4 glioma is required to reasonably substantiate deintensification of treatment.
IDH-wildtype glioblastoma (IDH-wildtype astrocytoma):IDH-wildtype Glioblastoma is the most common and aggressive type of primary central nervous system (CNS) malignancy.This type of glioma constitutes almost half of all CNS tumors with an overall survival of 5 to 10 percent in 5 years[41-43].A widely adopted standard of treatment for IDH-wildtype glioblastoma is the Stupp regimen[36].This regimen constitutes radiotherapy with concurrent and adjuvant TMZ.
Radiotherapy dosage is 60 Gy in 30 fractions,with 1.8 to 2 Gy per fraction,for patients less than 70 years and demonstrating good performance[36].The use of radiosurgery,brachytherapy,or doses greater than 60 Gy did not demonstrate any survival benefits[44,45].In patients 70 and greater,or patients with poor performance,a hypofractionated radiotherapy dosage of 40 or 34 Gy in 15 and 10 fractions respectively can be utilized[46,47].Employing an ultrashort radiotherapy course with 5 by 5 Gy doses did not improve overall survival for these patients[48].
Concurrent TMZ with the discussed radiotherapy approach in younger patients with good performance is administered for 6 cycles at 75 mg/m2/d[36].This treatment approach demonstrated a survival gain when compared to radiotherapy alone.In addition,patients with MGMT methylation demonstrated better outcomes and responses,but a significant survival gain was still demonstrated in patients without MGMT methylation.For patients 65 years and greater and with MGMT methylation,the use of concurrent TMZ with a hypofractionated radiotherapy regimen also demonstrated benefit,with improvements in overall survival[47].Similarity,older patients or patients with poor performance demonstrated similar survival in the absence of radiotherapy and with TMZ alone[46,49,50].Conversely,older patients or patients with poor performance with MGMT unmethylated demonstrated minimal survival gain with the addition of concurrent TMZ with radiotherapy[47].Despite these findings,the minimal survival gain with the administration of concurrent TMZ may be still be of benefit to patients because severe toxicity was not found to be different between TMZ and its concurrent administration with radiotherapy.
The literature suggest that the best treatment approach is the utilization of radiotherapy with concurrent and adjuvant TMZ at the discussed dosages for younger patients or patients with good performance.The treatment approach for elder patients or patients with poor performance is hypofractionated radiotherapy with the option of TMZ based on clinical intuition and potential consequences of increased toxicity[51].Future trials are needed to definitively determine the role of concurrent TMZ with radiotherapy for these patients when treating this grade 4 glioma.
PEDlATRlC GLlOMAS
With variability in the clinical presentations of gliomas in the pediatric population,an array of treatment modalities follow.The International Consortium on Low Grade Glioma and the European Society for Paediatric Oncology Brain Tumor Group have established protocols for treatment and therapy[52].Gross total resection is commonly curative and results in high overall and progression-free survival rates[53].Following complete resection,patients should be monitored clinically for neuro-deficits and radiologically for tumor relapse.Absence of radiological tumor growth and post-operative symptoms is an indication for continued follow-up and no additional chemotherapy or radiotherapy.
In some cases,complete tumor resection is not achievable due to the neural-anatomic site and potential for permanent neurological effects[53].Unresectable or incompletely resected pediatric low-grade gliomas (pLGG) tend to progress and warrant close observation and additional treatment.The optimal timing for follow-up chemo-and radiotherapy is controversial.International pLGG trials have studied whether prognostic differences exist among immediate and delayed postoperative chemo-or radiotherapy.Subjects with early post-operative radiotherapy demonstrated longer duration to tumor progression than those with delayed radiotherapy,but no significant differences in survival[54].Indications for immediate therapy include visual and neurological symptoms or the presence of tumor growth more than 25% on imaging[55-57].
WHO grade 1 and 2: Pilocytic and diffuse astrocytoma, ganglioglioma, and dysembryolastic neuroepithelial tumors
Majority of pediatric pLGG fall under the category of grade 1 and grade 2 lesions as recognized by the 2021 WHO Classification of Tumors of the Central Nervous System[38].WHO CNS5 describes the current approach for dividing brain tumors into 6 main categories,one of which includes pediatric type diffuse low-grade glioma[38].Common tumors in this class include pilocytic (Figure 4) and diffuse astrocytoma,ganglioglioma,and dysembryolastic neuroepithelial tumors.Additionally,15%-20% of children with pLGG have neurofibromatosis type 1 (NF-1),affecting treatment options and prognosis.This class of gliomas is the most frequently diagnosed solid tumor in the pediatric population and generally has a good prognosis,usually presenting as slow growing tumors[38,55].However,factors including age of diagnosis,histological findings,and genetic mutation status distinguish pLGG and individualize the clinical impact.
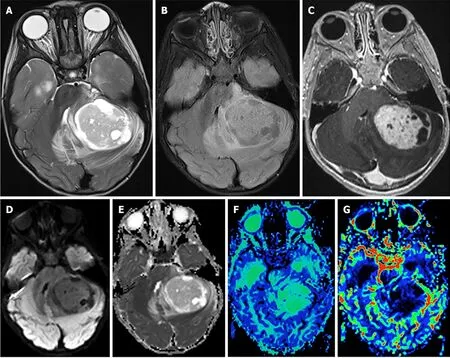
Figure 4 Pilocytic astrocytoma. A: Axial T2-weighted scan through the cerebellum demonstrating a well-defined solid-cystic mass in the left cerebellar hemisphere that is heterogeneous onT2-weighted sequence and causes mass effect to the 4th ventricle.The solid component is minimally hyperintense compared to the gray matter;B: An axial T2 FLAIR image through the same level better demonstrates the area of T2 hyperintensity beyond the tumor margin,suggestive of edema;C: An axial post-contrast T1-weighted sequence through the same level demonstrates intense enhancement of the solid component of the tumor;D and E:The axial diffusion image and ADC map (E) through the same level show no diffusion restriction;F: The mean transit time map demonstrates increased transit time within the solid component of the tumor;G: The cerebral blood volume map shows that the tumor has very low cerebral blood volume.Citation: Bag AK,Chiang J,Patay Z.Radiohistogenomics of pediatric low-grade neuroepithelial tumors.Neuroradiology 2021;63: 1185-1213.Copyright ©2021 The Authors.Published by Springer Nature[58] (Supplementary material).
First-line chemotherapy:Children with pLGG who meet the criteria for non-surgical intervention or who show tumor progression following surgical intervention are subsequently treated with chemotherapy.Chemotherapy was first introduced in the 1980s to avoid or delay pediatric exposure to therapeutic doses of radiation.The first line treatment in Europe and the United States for pLGG remains a combination of vincristine and carboplatin (V/C) as standard induction[58-62].The standard dosage of V/C may vary considering characteristics of the patient,tumor,and specific protocol.A standard induction consists of ten weekly doses of 1.5 mg/m2vincristine intravenous bolus and four total doses of 550 mg/m2carboplatin intravenous infusion at 3-wk intervals followed by 3 more cycles of V/C simultaneous doses at 4-wk intervals.Total duration of induction is 24 wk.A standard consolidation consists of ten doses of V/C at 6-wk intervals from week 25-85[55,59].
In an expanded follow-up study assessing outcomes of V/C treatment,a 56% objective response rate and 68% ± 7%progression free survival rate at 3 years post-diagnosis was seen among 78 pediatric patients diagnosed with pLGG[62].Further studies have been conducted to assess effects of additions to the standard treatment on survival and response outcomes.In a randomized trial involving 497 newly diagnosed pediatric patients across 11 countries,the addition of etoposide to vincristine and carboplatin (V/C/E) showed no difference as compared to V/C treatment arms.Overall survival for V/C and V/C/E was 46% and 45%,and progression-free survival 89% and 89%,respectively[59].It is worth mentioning that among children diagnosed with pLGG who were treated with V/C,event-free survival in children with NF-1 was significantly higher than non-NF1 patients[60].
Alternative chemotherapeutic options:Second and third-line chemotherapy strategies exist in the treatment of pLGG and may be employed in certain scenarios such as progressive tumor growth,recurrence,first-line intolerance,transformation to higher-grade,or patient choice.Patients who experience late recurrence of tumor growth following V/C regime may be re-treated with the same therapy if a positive response was demonstrated early on.Following a Common Terminology Criteria for Adverse Events Grade ≥ 2 due to a hypersensitivity reaction to carboplatin,secondline therapy is a replacement of carboplatin with cycles of 30 mg/m2cisplatin and 1500 mg/m2cyclophosphamide in combination with vincristine[55,59,63].
Alternatively,second line treatment following ineffectiveness of primary V/C therapy includes monotherapy with vinblastine.Vinblastine has shown promise in refractory pLGG and its low toxicity makes it a good option for carboplatin hypersensitivity[64,65].Treatment includes one intravenous bolus of 6 mg/m2vinblastine weekly for 70 wk[55,65-67].Among 50 children previously receiving first-line chemotherapy for pLGG,most commonly pilocytic astrocytoma and ganglioglioma,the five-year overall survival and five-year progression-free survival was 93.2% ± 3.8% and 42.3% ± 7.2%,respectively[64].In another study of 54 children with treatment naive pLGG,most commonly pilocytic astrocytoma,fiveyear overall survival and progression-free survival was 94.4% and 53.2%,respectively[65].
Additionally trialed chemotherapeutic options that have demonstrated promise with low toxicity profiles include a combination of 10 mg/kg bevacizumab and 10 mg/kg irinotecan,every 2-wk for a maximum of 2 years[68,69].Alternatively,a regimen of tioguanine,procarbazine,lomustine,and vincristine (TPCV) has been compared to standard treatment with V/C,with no significant differences in 5-year overall and progression-free survival identified[55,70].However,TPCV demonstrates a more toxic profile when compared to V/C,excluding carboplatin hypersensitivity reactions,and presents with increased risk secondary malignancy and infertility,especially in NF-1 patient groups[55,70,71].
Radiotherapy:While chemotherapy remains the primary non-surgical treatment,radiotherapy can be employed alone or as an adjuvant to chemotherapy in LGGs that cannot be resected[71].However,traditional photon radiotherapy possesses dangerous long-term cognitive,endocrine,and growth defects,most prominent in young children.Modern radiotherapy techniques such as stereotactic and proton therapy are capable of more precision and are effective in minimizing the longterm neurocognitive and endocrine sequalae associated with brain radiation in children.
No prospective studies comparing optimal radiotherapy dose-fractionation have been conducted in pediatric cohorts.In a prospective multicenter study of LGG treatment modalities,147 patients received radiotherapy with threedimensional conformal planning secondary to severe or progressive symptoms.Doses were equal or below 54 Gy in 1.8 Gy increments,and equal or below 45.2 Gy in 1.6 Gy increments for children less than five-years of age.The 10-year progression free survival was 62% with 9.2% of tumors progressing and no differences between grade 1 and grade 2 identified[72].In a retrospective study of children diagnosed with LGG treated with three-dimensional conformal radiotherapy,median doses of 54 Gy in 1.8 Gy,increments were associated with an overall survival of 94% and sevenyear progression free survival of 67%[73].
Stereotactic radiotherapy has proven effective in the management of progressive and inoperable pLGG.A mean total dose of 52.2 Gy in 1.8 Gy fractions employing a 2-mm margin to the target has shown a five-year progression-free survival rate of 82.5% and an overall survival rate of 97.8% at 5 years[74].Additionally,the use of fractionated stereotactic radiotherapy for reirradiation has been evaluated in recurrent gliomas among adult patients,but its use among the pediatric population warrants further study[75].
Proton therapy,with its precision-targeted approach,offers a promising avenue for the treatment of pLGGs,potentially minimizing radiation exposure to the surrounding healthy brain tissue.Treatment of progressive pLGG with proton therapy included radiation of gross tumor volume with a 5-mm margin and a clinical target volume dose of 54 Gy.Outcomes demonstrate a 3-year overall survival of 95% and a 3-year progression-free survival of 87%[76].In another pilot study of magnetic resonance imaging (MRI)-guided adaptive planning for pLGG treated with proton therapy,it was found that mid-treatment imaging adjustments,based on a standard dose of 52.2 Gy in 1.9 Gy fractions,led to notable reductions in doses to key organs,potentially minimizing brainstem and optic nerve toxicities[77].
Biologics:Though the use of adjuvant chemo-and radiotherapy have been historically used in the treatment of progressive LGG,these therapies are associated with toxicity and long-term sequalae.Such considerations are magnified by a good prognosis for pLGG despite a low progression-free survival.As a result,discovery of specific molecular pathways in pLGG have led to the development of effective targeted therapies with lower toxicity profiles.
First-line therapy remains a combination of BRAF and MEK inhibitorsvsBRAF inhibitor monotherapy due to combined treatment demonstrating improved progression-free survival and reduced toxicity in adults in separate studies[78,79].A multi-center Phase II clinical trial is underway in investigating the activity of dabrafenib in combination with trametinib in adolescents with BRAF V600 mutation positive LGG[80].The treatment regime under investigation in pediatric patients includes 0.5-5.25 mg/kg/d dabrafenib orally,twice daily,and 0.025-0.032 mg/kg/d trametinib,orally,once daily[80].
There is significant evidence of BRAF-targeted therapy in brain tumors harboring the BRAF gene[81,82].BRAF mutations have been identified in 5%-15% of pLGG,most prominently in pleomorphic xanthoastrocytoma and ganglioglioma[83].Approved therapies include combination therapies of BRAF inhibitors such as vemurafenib and dabrafenib,and MEK inhibitors such as selumetinib and trametinib[84].
A series of case reports have shown promising results with the use of first-generation BRAF inhibitor monotherapy in recurrent pLGGs such as pilocytic astrocytoma,hypothalamic glioma,ganglioglioma,and other low-grade brain tumors[85-90].A 2-part clinical trial explored the safety of dabrafenib treatment in pediatric patients with BRAF V600 positive refractory LGG,including pilocytic astrocytoma,ganglioglioma,pilomyxoid astrocytoma,and pleomorphic xanthoastrocytoma[91].Dabrafenib administration was started at 3.0 mg/kg,twice daily,with increments of 0.75 mg/kg,not exceeding the adult recommended dose of 300 mg/d[91,92].Results extrapolated from part I and IIa of the study demonstrated this drug was well tolerated by pediatric patients at doses that induced pharmacokinetics reported in adult trials and an overall response rate of 44% with a one-year progression free survival of 85%[91,92].
WHO grade 3 and 4
Close to 20% of all childhood gliomas are categorized as pediatric high-grade glioma (pHGG) (Figure 5)[93].The latest WHO CNS5 classification introduces a new category for high grade gliomas,pediatric type diffuse high-grade gliomas,which includes both grade 3 and grade 4 gliomas[38].In this updated classification,the high-grade glioma (HGG) family is also comprised of four tumor types with molecular nomenclature: Diffuse midline glioma,H3 K27-altered;Diffuse hemispheric glioma,H3 G34-mutant;Diffuse pediatric-type high-grade glioma,H3-wildtype and IDH-wildtype;Infanttype hemispheric glioma[38].Overlap of grade among tumor types is dependent on multiple histological and clinical factors,and grade progression of tumors is common in the pediatric population.At presentation,anaplastic astrocytoma,including IDH-wildtype and IDH-mutant astrocytoma,and IDH-mutant anaplastic oligodendroglioma are typical grade 3 pHGG.Glioblastoma,both IDH-wildtype and IDH-mutant,and diffuse hemispheric glioma,H3 G34-mutant,commonly fall under grade 4 classification[38].
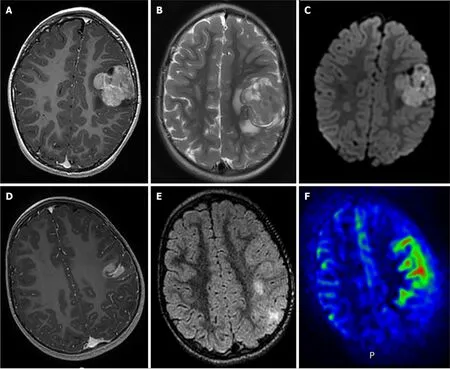
Figure 5 Radiological features of two supratentorial pediatric high-grade gliomas of the subclass MYCN. A-C: T1-weighted images after contrast media injection (A),T2-weighted images (B),and diffusion-weighted images (C): a solid lesion with peri-lesional edema,homogeneous enhancement and hypercellularity (apparent diffusion coefficient (ADC) on diffusion weighted images is restricted in the main part of the tumor) (Case 3);D-F: T1-weighted images after contrast media injection (D),FLAIR-weighted images (E) and cerebral blood flow map using arterial spin labeling (F): a solid and infiltrative lesion with homogeneous enhancement and high cerebral blood flow (Case 1).Citation: Tauziède-Espariat A,Debily MA,Castel D,Grill J,Puget S,Roux A,Saffroy R,Pagès M,Gareton A,Chrétien F,Lechapt E,Dangouloff-Ros V,Boddaert N,Varlet P.The pediatric supratentorial MYCN-amplified high-grade gliomas methylation class presents the same radiological,histopathological and molecular features as their pontine counterparts.Acta Neuropathol Commun 2020;8: 104.Copyright ©2020 The Authors.Published by BioMed Central Ltd[100] (Supplementary material).
The overall prognosis of pHGG is poor despite intensive treatment protocol,with five-year survival rates near 20% and prognosis most influenced by the extent of tumor resection[94,95].Treatment for HGG commonly includes surgical resection followed by adjuvant chemo-and radiotherapy,however more targeted molecular approaches are of interest to reduce harmful side effects of systemic therapies.
Current recommendations for postoperative treatment of anaplastic astrocytoma are dependent on the extent of excision and tumor involvement in eloquent brain regions.According to the 2023 National Comprehensive Cancer Network guidelines on HGG,a multidisciplinary approach precedes surgical intervention to assess feasibility and safety in maximal tumor resection[96].Maximal safe resection of tumor is the preferred initial approach in adults,with postoperative imaging for verification of complete resection,however no trials have been conducted in pediatric populations[97,98].Integrating positron emission tomography scanning data with MRI during navigational planning can improve tumor volume definition and surgical precision in brain tumor resections,leading to more complete removal of metabolically active tumor regions[99].
IDH-mutant anaplastic astrocytoma;WHO grade 3:The treatment of pediatric patients with IDH-mutant astrocytoma is less well-defined than the treatment protocols for adults.The rarity of IDH-mutant astrocytoma in pediatric populations compared to adults contributes to this lack of specific guidelines.General approaches to these tumors in children are informed by a combination of pHGG guidelines and the adult IDH-mutant astrocytoma literature.Anaplastic astrocytoma generally present with poor prognosis with 5 and 10-year survival rates of 23.6% and 15.1% respectively[100,101].
Following maximal safe resection and integration of histologic and molecular features,recommended treatment of anaplastic astrocytoma is standard radiotherapy by conformal techniques including three-dimensional conformal radiation therapy and intensity-modulated radiation therapy.For radiation treatment planning,pre-and post-surgery MRI can accurately determine tumor dimensions,with the suggested treatment volume being the detected tumor size plus an additional 1-2 cm,typically receiving between 45-54 Gy in fractions of 2.0 Gy,followed by a boost plan of 14 Gy in 2 Gy fractions[23,24].In the event of recurrence,reirradiation with advanced techniques such as sterotactic radiosurgery are employed for smaller tumors and proton therapy aids in protecting previously irradiated brain tissue[96,102].
In addition to standard radiotherapy,adjuvant or concurrent chemotherapy is recommended in the treatment of grade 3 IDH-mutant astrocytoma.TMZ is the primary systemic therapy recommended administered,followed by PCV[96].When administered as an adjuvant following radiotherapy,TMZ is typically started at 150 mg/m2per day for five days during the first cycle.If no hematologic toxicity is observed,the dose may be increased to 200 mg/m2per day for five days in subsequent cycles.Adjuvant TMZ is given in 12 cycles,each lasting 4 wk[50,103].When administered concurrently with standard radiotherapy,TMZ is administered 75 mg/m2per day,12 cycles each lasting 4 wk[103].No significant survival differences were identified between adjuvant TMZ and PCV,although TMZ has shown greater tolerability[104].
Recurrent high-grade astrocytoma common within 3 years of diagnosis,necessitates a thorough evaluation,potentially including biopsy or resection[105].Recommended regimens of systemic therapy still include TMZ without standard radiotherapy at 180-200 mg/m2as monthly 5-d courses for up to 12 cycles[106].Additional options include lomustine/carmustine high-dose chemotherapy and targeted therapy including VEGF inhibitor bevacizumab[107-109].Similar recommendations are in place for recurrence of anaplastic oligodendroglioma[96].
IDH-mutant,1p/19q-codeleted oligodendroglioma;WHO grade 3:Oligodendroglioma is a rare tumor subtype of diffuse glioma in the pediatric population,contributing to less than 1% of brain tumor diagnoses[110,111].Similar to anaplastic astrocytoma,the rarity of this tumor in children has led to gaps in the literature.Initial treatment is surgery,with chemotherapy and radiotherapy typically administered as adjuvant treatment[96,110,111].Prognosis for grade 3 anaplastic oligodendroglioma is generally poor,with estimated 5-year overall survival to be 53%[110].For the diagnosis of anaplastic oligodendroglioma,precise molecular and histological information is required to classify tumor grade and determine best therapies.
Adjuvant radiotherapy in WHO grade 3 oligodendroglioma is typically treated by the same conventions of grade 3 IDH-mutant astrocytoma,following maximal safe resection.Radiotherapy has shown to be effective in the management of oligodendroglioma,prolonging the duration of progression free survival among pediatric patients as compared to treatment with chemotherapy alone,but has had no significant difference in overall survival[35,112].Recommended radiotherapy fractioning differs from anaplastic astrocytoma,however,as a result of differences in tumor prognosis.As suggested in multiple clinical trials studying radiotherapy efficacy,the initial 50.4 Gy is given in 1.8 GY fractions as compared to 2.0 Gy fractions in grade 3 astrocytoma,covering the tumor volume with a 2-cm margin[34,113].
While surgical resection followed by radiotherapy is the mainstay of management,the role of adjuvant chemotherapy has come into focus due to a growing understanding of the tumor's molecular landscape and the push towards minimizing treatment-related long-term morbidity.Recommended systemic therapy includes neoadjuvant or adjuvant PCV,concurrent TMZ,or adjuvant TMZ[96].Recommendations are based on studies that have shown that chemotherapy with radiotherapy,either concurrently or sequentially,significantly improved 5-year overall survival compared to radiotherapy alone[114].For primary oligodendroglioma,recommendations of PCV are administration after radiotherapy in six,one-week cycles,started within four weeks after the end of radiotherapy.This protocol has demonstrated significant improvement in overall and progression free survival in anaplastic oligodendroglioma[33].Additionally,PCV has proven to be more effective in prolonging overall survival and 5-year progression free survival specifically in patients with 1p/19q co-deleted tumors[34,114,115].Neoadjuvant PCV as a preliminary treatment has significantly increased survival rates in patients with 1p/19q mutated oligodendroglioma,indicating that PCV may be beneficial when administered just before radiotherapy[34].
IDH-wildtype glioblastoma (IDH-wildtype astrocytoma);WHO grade 4:Pediatric glioblastoma accounts for only approximately 3% of all pediatric CNS tumors with an incidence of around 0.85 per 100000 children in the United States[116,117].As a result,much of the recommended treatment protocols are adopted from adult studies and clinical trials.Studies specific to glioblastoma are limited as well with most of the literature assessing HGG together.Maximal safe resection is recommended,when possible,followed by chemotherapeutic regimes and radiotherapy if indicated for the pediatric patient[117].These tumors typically present in the second decade of life as headaches and with mass effect symptoms.Unfortunately,prognosis is poor with a 5-year survival of less than 20%[116].
For glioblastoma treatment,recommendations for radiotherapy follow similar guidelines as for grade 3 HGG.Tumor volumes are primarily defined using MRI scans,with 1-2 cm margins recommended to address undetected tumor infiltration.Radiotherapy dosing is typically 60 Gy in 2.0 Gy fractions or 59.4 Gy in 1.8 Gy fractions[118].In certain scenarios,like extensive tumor volume or brainstem involvement,the dose may be reduced to 54-57 Gy.For initial treatment phases,45-50.4 Gy in 1.8 Gy fractions is given,followed by a "boost" phase with 9-14.4 Gy in 1.8 Gy fractions[96,119].In cases involving elderly patients and sometimes children,a hypo-fractionated course ranging from 25 Gy in 5 fractions to 40.05 Gy in 15 fractions may be considered,although no significant differences in survival have been identified in the pediatric population[48,120,121].Radiotherapy is not indicated in patients younger than three years due to adverse neurocognitive,psychosocial,and behavioral effects and an increased risk of recurrence secondary malignancy[96,116].
The integration of chemotherapy in the treatment of glioblastoma has emerged as a potential means of increasing overall survival.Current recommendations include concurrent or adjuvant TMZ,with some molecular mutations potentiating the effect of this treatment.Preliminary research contrasting the outcomes of standalone radiation therapy with combined TMZ chemoradiotherapy administered at 75 mg/m2daily and subsequently at 150-200 mg/m2postradiation demonstrated a prolonged median survival period in adults[36].However,TMZ has not been found to enhance outcomes for children with high-grade astrocytoma when compared to results from the Children's Cancer Group study CCG-945[122,123].In pediatric glioblastoma,adding 90 mg/m2lomustine to radiotherapy and concurrent 160 mg/m2TMZ per day for 5 d every 6 wk has been found to enhance progression-free survival rates as compared to TMZ alone,particularly among those overexpressing MGMT[124].
The aggressive nature of recurrent glioblastoma necessitates a multi-modal approach,with pharmacological intervention and research at the forefront.Bevacizumab,a monoclonal antibody targeting VEGF,has shown effectiveness in recurrent glioblastoma in adults and may be administered 10mg/kg every two weeks as a potential therapeutic agent in children.Though well tolerated,the response rate and prolongation of survival are not as effective as in the adult population[125,126].Among adult subjects with recurrent glioblastoma,a six-week cycle of 100-130 mg/m2lomustine has demonstrated efficacy in increasing overall survival[127].Furthermore,the combination of bevacizumab with lomustine demonstrates increased progression-free survival as compared to lomustine monotherapy[128,129].
Several therapies have been trialed for their effectiveness in improving overall survival and progression-free survival among children,including an assessment of their tolerance and toxicity profiles.Such therapies have included irinotecan,cilengitide,and sunitinib,all presenting with uncertain efficacy warranting further research[130].
CONCLUSlON
Gliomas represent a category of primary brain tumors originating from glial cells of the central nervous system that account for most brain tumors in adults.Their classification and grading,determined by histological attributes and cellular lineage,provide a foundational roadmap for therapeutic decision-making for clinicians.In adults,the treatment often comprises of surgical resection,chemotherapy,and radiotherapy,with the latter also providing benefit in the reduction of seizures and progression-free survival.Pediatric gliomas,however,present a more intricate therapeutic challenge given their variability.While total tumor resection can be curative contingent upon its size and position,some inoperable cases necessitate a structured chemotherapy regimen.This often involves vincristine,coupled with carboplatin.Should chemotherapy not be effective,Vinblastine becomes a viable alternative.Radiotherapy is another option,however,concerns of neurological and endocrinological side effects in pediatric patients must be weighed.The journey for refining treatment strategies remains ongoing,especially in exploring the optimal therapeutic approach for IDH-mutant astrocytomas and honing the precision of radiotherapy dosing for young patients.Future investigations are imperative to further our understanding and enhance outcomes.
FOOTNOTES
Author contributions:Mohamed AA,and Lucke-Wold B designed the research study;Mohamed AA,Alshaibi R,Faragalla S,Mohamed Y and Lucke-Wold B performed the research and analyzed the data and wrote the manuscript;All authors have read and approve the final manuscript.
Conflict-of-interest statement:The authors declare that they have no conflict-of-interest.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORClD number:Ali Ahmed Mohamed 0000-0002-0977-0365;Brandon Lucke-Wold 0000-0001-6577-4080.
S-Editor:Zhang H
L-Editor:A
P-Editor:Yu HG
 World Journal of Clinical Oncology2024年2期
World Journal of Clinical Oncology2024年2期
- World Journal of Clinical Oncology的其它文章
- Unlocking the potential-vitamin D in prostate cancer prevention
- Deregulation of interferon-gamma receptor 1 expression and its implications for lung adenocarcinoma progression
- Elucidating the molecular basis of ATP-induced cell death in breast cancer: Construction of a robust prognostic model
- ldentification of immune cell-related prognostic genes characterized by a distinct microenvironment in hepatocellular carcinoma
- Population-based X-ray gastric cancer screening in Hiroshima prefecture,Japan
- Endoscopic resection for calcifying fibrous tumors of the gastrointestinal tract