
Endoscopic resection for calcifying fibrous tumors of the gastrointestinal tract
2024-03-07 04:29ZiHanGengYanZhuPeiYaoFuYiFanQuShiYaoChenYunShiZhongYiQunZhangWeiFengChenWenZhengQinJianWeiHuMingYanCaiLiQingYaoQuanLinLiPingHongZhou
Zi-Han Geng,Yan Zhu,Pei-Yao Fu,Yi-Fan Qu,Shi-Yao Chen,Yun-Shi Zhong,Yi-Qun Zhang,Wei-Feng Chen,Wen-Zheng Qin,Jian-Wei Hu,Ming-Yan Cai,Li-Qing Yao,Quan-Lin Li,Ping-Hong Zhou
Abstract BACKGROUND Calcifying fibrous tumors (CFTs) are rare mesenchymal lesions that can occur in various sites throughout the body,including the tubular gastrointestinal (GI)tract.AIM To analyze the clinical findings of 36 patients with GI tract CFTs to provide guidance for diagnosis and treatment.METHODS This retrospective study included 36 patients diagnosed with CFTs of the GI tract.We collected demographic and clinical information and conducted regular followups to assess for local recurrence.RESULTS The stomach was the most commonly involved site,accounting for 72.2% of the 36 CFTs.Endoscopic mucosal resection (n=1,2.8%),endoscopic submucosal dissection (n=14,38.9%),endoscopic full-thickness resection (n=16,44.4%),and submucosal tunneling endoscopic resection (n=5,13.9%) were used to resect calcifying fibrous tumors.Overall,34 (94.4%) CFTs underwent complete endoscopic resections with a mean procedure time of 39.8 ± 29.8 min.The average maximum diameter of the tumors was 10.6 ± 4.3 cm.No complications,such as bleeding or perforation,occurred during an average hospital stay of 2.9 ± 1.2 d.In addition,two patients developed new growth of CFTs near the primary tumor sites,and none of the patients developed distant metastases during the follow-up period.CONCLUSION GI tract CFTs are rare and typically benign tumors that can be effectively managed with endoscopic procedures.
Key Words: Endoscopic resection;Calcifying fibrous tumor;Gastrointestinal tract
lNTRODUCTlON
Calcifying fibrous tumors (CFTs) are rare and benign lesions that were first identified as pediatric soft-tissue lesions by Rosenthal and Abdul-Karim in 1988[1].In 1993,CFTs were also recognized as calcifying fibrous pseudotumors[2].These tumors have been documented in various anatomical sites,including serosal surfaces,solid and tubular organs,and soft tissue.Most gastrointestinal (GI) CFTs have been described in single-case reports.Previous studies have shown that CFTs are commonly found in the stomach,small bowel,and large bowel[3,4].The first case report of a gastric CFT was discovered during a routine health screening using endoscopy and was completely resected by endoscopic submucosal dissection (ESD)[5].Although most CFTs are clinically silent and are found incidentally during endoscopy,some patients may present with abdominal pain,intussusception,or obstructive symptoms.
CFTs are benign mesenchymal neoplasms with a low risk of recurrence and can be cured by local excision.The primary treatment goal for CFTs is to alleviate symptoms such as intussusception and obstruction.However,no cases of metastasis have been documented.To the best of our knowledge,limited research has been conducted on GI CFTs,which is the main focus of this study.Our study included a long-term follow-up period to assess prognosis and adopted followup strategies based on the results of histopathological evaluations.
MATERlALS AND METHODS
Patients
We carried out a single-center retrospective study involving 36 consecutive patients diagnosed with CFTs who underwent endoscopic resection -specifically,ESD,endoscopic full-thickness resection (EFTR),or submucosal tunneling endoscopic resection (STER) -at Zhongshan Hospital Fudan University,Shanghai,China,from December 2016 to September 2021.Only patients with available follow-up data and complete demographic and clinical information were included in the study.Preoperative assessments were based on endoscopy,computed tomography (CT),or endoscopic ultrasonography (EUS) results Tumor characteristics,endoscopic methods,complications,en blocresection rate,complete resection rate,local recurrence,and distant metastases were evaluated for all patients.This study was approved by the Ethics Committee of Zhongshan Hospital,in accordance with the Declaration of Helsinki (B-2018-222).Informed consent was obtained from all participants.
Procedures
To excise the tumor,a standard endoscope (GIF-Q260J;Olympus,Tokyo,Japan) equipped with a transparent cap (D-201-11804;Olympus,Tokyo,Japan),an I-type hybrid knife (ERBE;Erbe Elektromedizin GmbH,Tübingen,Germany),a hook knife (KD-620LR;Olympus,Tokyo,Japan),and an IT knife (KD-611L;Olympus,Tokyo,Japan).Additional accessories comprised an argon plasma coagulation unit (APC300;Erbe),hot biopsy forceps (FD-410LR;Olympus,Tokyo,Japan),and a polypectomy snare.
The patients underwent endotracheal intubation under general anesthesia.Prophylactic intravenous antibiotics were administered routinely 30 min before the procedure,and CO2was utilized to minimize gas-related complications during the procedure.Additionally,when necessary,a 20-gauge needle filled with normal saline was inserted into the right lower quadrant to mitigate intraoperative pneumoperitoneum.
Endoscopic mucosal resection procedures
Endoscopic mucosal resection (EMR) was indicated for GI lesions less than 20 mm in size that can be easily lifted and have a low risk of submucosal invasion[6].The main steps of EMR were as follows: (1) After locating the lesion,a mixture of normal saline and indigo carmine was injected into the submucosa;(2) The lesion was removed using a snare;(3)Argon plasma coagulation or hot biopsy forceps were used to prevent delayed bleeding;and (4) The defect was closed with metal clips.
ESD procedures
ESD has been used to resect lesions originating from the superficial muscularis propria (MP) with an intraluminal growth pattern[7].The main steps were as follows: (1) A margin of 5 mm away from the edge of the lesion was marked for orientation using an endoscopic knife;(2) A mixture of normal saline and indigo carmine was injected into the submucosa;(3) The mucosal and submucosal layers were precut along the tumor base with an I-type hybrid knife;(4) The tumor was gradually dissected using an IT knife,extending as deep as the bottom around the lesion;(5) The tumor was removed with a snare;(6) Argon plasma coagulation or hot biopsy forceps were used to prevent delayed bleeding;and(7) The defect was closed with metal clips.
EFTR procedures
EFTR has been used to resect lesions originating from the deep MP or serosa with an extraluminal growth pattern[8].The main steps of EFTR were similar to those of ESD,except that intentional perforations were performed to achieve complete tumor removal.However,the serosa was preserved whenever possible to prevent gas extravasation and intra-abdominal contamination.Closure of the defect following EFTR required advanced endoscopic skills.When the defect was smaller or slightly larger than the width of the open clip,metal clips were used for defect management.For defects larger than 15-20 mm,a combination of metal clips and nylon rope or the omental-patch method was necessary.
STER procedures
STER has a lower risk of leakage;however,its application is limited by the anatomical location of the lesion.The most suitable sites for STER are the esophagus and cardia.The main steps are as follows: (1) A mixture of normal saline and indigo carmine is injected into the submucosa 2-4 cm proximal to the lesion,and a mucosal incision is made to serve as the tunnel entry;(2) Injection and dissection are carried out between the submucosal and muscular layers to create a tunnel toward the lesion;(3) The tumor is dissected in a manner similar to that of ESD or EFTR;(4) The tumor is removed using a snare;(5) Argon plasma coagulation or hot biopsy forceps are used to prevent delayed bleeding;and (6) The mucosal entry is closed with metal clips.
After endoscopic resection,a nasogastric or rectal tube was placed to decompress and monitor the wound for delayed bleeding.Additionally,we monitored for postoperative symptoms,including fever,hematemesis,melena,dyspnea,chest pain,and signs of pneumothorax.If a patient had persistent fever,hematemesis,melena,or pain,emergent endoscopy and CT would be performed.Furthermore,proton pump inhibitors,antibiotics,and hemocoagulase were administered.
Outcome assessments
Assessments of the primary outcomes included: (1) The procedure duration,which began with the mucosal incision for STER or the marking of several dots around the lesion for ESD and EFTR,and concluded with the closure of the wound;(2)En blocresection,defined as the excision of the tumor in one piece without fragmentation;and complete resection,defined on the basis ofen blocresection,excision without apparent residual tumors assessed macroscopically by the endoscopist at the resection site and with negative margins (both lateral and basal resection margins) on pathological examination;(3) Complications and the duration of the hospital stay;and (4) Local recurrence and distant metastases.
Follow-up
Patients underwent regular follow-up to evaluate wound healing,local recurrence,and distant metastases through endoscopy or telephone interviews at 3 and 6 months after resection.Detailed telephone interviews were conducted by trained physicians for patients who were unwilling to return for follow-up visits.These interviews included questions about any examinations and treatments received at other hospitals.The final follow-up was conducted in March 2022.For patients who experienced relapses,endoscopy and EUS were performed to check for recurrent tumors,while abdominal EUS and CT were conducted to assess for distant metastases.
Statistical analysis
Continuous variables were presented as means ± SD,N~ (μ,σ2),while categorical variables were presented as numbers and percentages of the total.Statistical analysis was performed using SPSS software version 26.0.
RESULTS
Clinical characteristics of the patients
A total of 36 consecutive patients (19 women and 17 men) aged 46.4 ± 12.6 years,were diagnosed with CFTs and underwent endoscopic resection at Zhongshan Hospital,Fudan University,Shanghai,China.The majority of patients were asymptomatic (n=21,58.3%),while 12 experienced abdominal discomfort.Symptoms such as dysphagia,vomiting,and diarrhea were also observed (Table 1).
Table 1 Clinical characteristics and procedural outcomes of patients with calcifying fibrous tumors
Characteristics of tumors
The most commonly affected sites were the stomach (n=26,72.2%),which included 20 cases in the gastric body,four in the gastric fundus,and two in the gastric antrum.This was followed by the large intestine (n=6,16.7%),the esophagus (n=3,8.3%),and the small intestine (terminal ileum,n=1,2.8%).Within the large intestine,the rectum was the most frequent location (n=4).During preoperative endoscopy,all CFTs showed a tenacious texture and broad pedicles with smooth mucosa.Most CFTs presented with an intraluminal growth pattern (n=32,88.9%).The gross morphology revealed that the well-defined CFTs were either round (n=34,94.4%) or dumbbell-shaped (n=2,5.6%),with a gray surface.The maximum diameter of the CFTs ranged from 10.6 ± 4.3 cm.The MP was the most commonly involved layer (n=29,80.6%),followed by the submucosa (n=7,19.4%).None of the patients had mucosal involvement or accompanying CFTs in other parts of the body (Supplementary Table 1).
Endoscopic methods and outcomes
Endoscopic resection is the primary treatment method for CFTs.In this study,all 36 patients underwent endoscopic resections,including STER (n=5,13.9%) (Figure 1),EMR (n=1,2.8%),ESD (n=14,38.9%),and EFTR (n=16,44.4%)(Figures 2 and 3).Sixteen (44.4%) CFTs were resected using EFTR.The suture method included metal clips (n=25,69.4%)(Figure 1),a combination of metal clips and nylon rope (n=8,22.2%) (Figure 2),and fully covered removable nitinol selfexpandable metal stents (SEMS) (n=1,2.8%) (Figure 3).Postoperative GI decompression was performed for 16 patients(44.4%).The mean duration of the procedures ranged from 39.8 ± 29.8 min.Minor bleeding occurred in all cases during resection,but there were no intraoperative complications.Overall,en blocresection was performed for 34 CFTs (94.4%),and complete resection was achieved in 34 cases (94.4%).
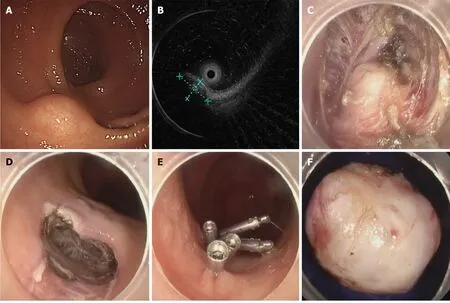
Figure 1 Submucosal tunneling endoscopic resection for a calcifying fibrous tumor of the rectum originating from the muscularis propria. A: Calcifying fibrous tumor of the rectum;B: The mass as observed under the endoscopic ultrasonography;C: The mass within the submucosal tunnel;D:Entrance to the submucosal tunnel;E: Metal clip used to suture the wound;F: Gross appearance of the resected mass.
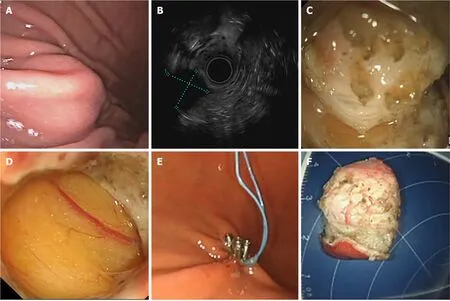
Figure 2 Endoscopic full-thickness resection for a calcifying fibrous tumor of the stomach originating in the muscularis propria. A:Calcifying fibrous tumor of the stomach body;B: The mass as observed under the endoscopic ultrasonography;C: The mass originating from the muscularis propria;D: Omentum visible through the wound;E: Combination of nylon rope and metal clips to suture the wound;F: Gross appearance of the resected mass.
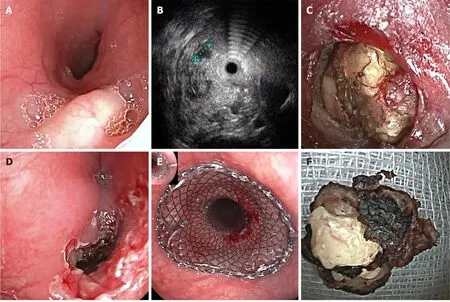
Figure 3 Endoscopic full-thickness resection for a calcifying fibrous tumor of the esophagus originating from the muscularis propria. A:Calcifying fibrous tumor in the esophagus;B: The mass as observed under endoscopic ultrasonography;C: The mass originating from the muscularis propria;D: The large wound;E: Metal stent used to seal the wound;F: Gross appearance of the resected mass.
For the 16 CFTs that underwent full-thickness resection,they were located in the MP of the esophagus (n=1,6.2%),stomach (n=13,81.2%),colon (n=1,6.2%),and rectum (n=1,6.2%).Furthermore,the wounds were sutured using metal clips (n=7,43.7%),purse-string sutures combined with metal clips and nylon rope (n=8,50.0%),and SEMS (n=1,6.2%).The majority of patients (n=12,75%) underwent GI decompression following resection.A CFT located in the deep layer of the esophageal MP was excised using EFTR,with a stent employed intraoperatively to repair the large wound defect in the esophagus (Figure 3).
The average duration of hospital stay post-surgery was 2.9 ± 1.2 d.None of the patients experienced delayed wound bleeding,GI tract leakage,secondary peritoneal infection,or abdominal infection.Additionally,two patients developednew growths of CFTs near the sites of the primary tumors that had been completely resected.No patient developed distant metastases during the follow-up period (Supplementary Table 1).The two patients with new growths underwent re-treatment with ESD,and no recurrences were observed during follow-up.
DlSCUSSlON
Prior to the resection,CFTs in the GI tract are easily misdiagnosed as GI stromal tumors[9].A clear identification of CFTs is essential to distinguish benign tumors from other mesenchymal GI lesions,given their rarity in the GI tract.Based on our findings,it could be inferred that CFTs were most frequently found in the stomach,followed by the large intestine.GI tract CFTs were usually asymptomatic and recognized during endoscopic examination.Moreover,some patients with CFTs might suffer from non-specific GI symptoms such as abdominal discomfort,dysphagia,vomiting,and diarrhea.
To date,there have been few studies on the treatment of GI CFTs.A previous meta-analysis indicated that more than half of the patients received treatments other than endoscopy[9].We reviewed all GI CFT cases from the same period at our hospital and found that all patients underwent endoscopic treatment rather than surgical resection.Given that CFTs are predominantly located in the MP of the GI tract,ESD,EFTR,and STER constituted the majority of the endoscopic resections.The choice of resection method depends on the characteristics of the CFTs,including the growth pattern,tumor size,location,and depth.In our study,all patients underwent endoscopic resection without any complications.Therefore,endoscopic resection is a viable treatment option for CFTs.
Some studies have reported that endoscopic resection is a feasible and safe option for GI submucosal tumors (SMTs)because it can achieve radical excision with clear margins.Similarly,endoscopic resection was successfully performed on our patients with a short procedure duration,and all patients recovered quickly without severe complications.Additionally,short hospital stays and quick recovery from dietary restrictions can alleviate economic pressure and mental burden of the patients.Therefore,endoscopic resection is expected to become the first-line treatment choice for endoscopists managing patients with CFTs.
It has been observed that metal clips can be used to manage general active bleeding (acute non-variceal GI bleeding).However,the combination of nylon rope and metal clips is more effective for large and deep ulcerated lesions at specific sites.Our study found that CFTs were primarily located in the MP with significant depth;thus,most were removed using EFTR,and metal clips combined with nylon rope were utilized for suturing in this context to reduce the risk of delayed bleeding and perforation.Postoperative GI decompression was also performed.
In our study,33.3% of CFTs were removed using EFTR.EFTR has been most frequently used for SMTs originating from the MP of the GI tract.It allows complete resection of tumors,thereby reducing the risk of residual tumor and improving the accuracy of pathologic diagnosis.SMTs resected by EFTR are usually located in the deep layer.To expose the lesion and assess the tumor margin,the mucosa and submucosa covering the lesion are sometimes resected with a snare.Active perforation of the GI wall is often created due to the close relationship between SMTs and the serosa.Therefore,the closure of GI wall defects is essential.Minor full-thickness defects can be managed through standard endoscopic clips after air suction.Metal clips combined with the nylon rope or the omental-patch method can be used for large defects.
Furthermore,five cases (13.9%) were treated with STER.This technique builds a submucosal tunnel to serve as an operating space for resecting SMTs.STER offers a significant advantage in preserving the integrity of the overlying mucosa,thereby reducing the risk of postoperative GI tract leakage and secondary infection.However,STER is not recommended for SMTs with ulceration as it is not possible to maintain mucosal integrity in such cases.It is critical to avoid perforating the mucosa while establishing the submucosal tunnel.Frequent injections of a solution into the submucosal space can be particularly beneficial in distinguishing the mucosal layer and minimizing unintended mucosal injuries.
In our study,postoperative pathology revealed no residual tumors at the resection margins,and no recurrences were observed.However,2 patients showed new growth of CFTs during the median follow-up period of two years,with no recurrences after subsequent re-resection.Therefore,regular endoscopic surveillance is recommended.
Our study had several limitations.Firstly,the sample size was relatively small due to the rarity of GI CFTs in the population.Secondly,this was a retrospective study,which may have introduced potential biases.Therefore,further research is warranted in the future.
CONCLUSlON
In conclusion,GI CFTs are rare benign tumors that can be successfully removedviaendoscopic procedures.
ARTlCLE HlGHLlGHTS
Research background
Calcifying fibrous tumors (CFTs) are rare mesenchymal lesions found in various body sites,including the tubular gastrointestinal (GI) tract.
Research motivation
To the best of our knowledge,limited research has been conducted on GI CFTs,which is the main focus of this study.
Research objectives
Analyze clinical findings in 36 patients with GI tract CFTs to guide diagnosis and treatment.
Research methods
Retrospective study of 36 GI tract CFT patients,collecting demographic and clinical data,with regular follow-ups for local recurrence assessment.
Research results
Stomach involvement was most common (72.2% of 36 CFTs).Various endoscopic resection techniques were employed,with 94.4% achieving complete resection in 39.8 ± 29.8 min.Average tumor diameter was 10.6 ± 4.3 cm.No complications occurred during a 2.9 ± 1.2 d hospital stay.Two patients had new CFT growth near primary sites,and no distant metastases occurred in follow-up.
Research conclusions
GI tract CFTs,rare and mostly benign,can be effectively managed through endoscopic procedures.
Research perspectives
In the future,we need to carry out studies with prospective large samples.
FOOTNOTES
Co-first authors:Zi-Han Geng and Yan Zhu.
Co-corresponding authors:Quan-Lin Li and Ping-Hong Zhou.
Author contributions:Geng ZH contributed to conceptualization,data curation,formal analysis,investigation,methodology,software,validation,visualization,took the lead in writing -original draft and writing -review and editing;Zhu Y contributed to conceptualization,software,writing -original draft,writing -review and editing;Fu PY contributed to conceptualization,software,writing -original draft,took the lead in writing -review and editing;Qu YF contributed to conceptualization and data curation;Chen SY,Zhong YS,Zhang YQ,Chen WF,Qin WZ,Hu JW,Cai MY,and Yao LQ contributed equally to conceptualization;Li QL and Zhou PH contributed equally to conceptualization and supervision.
Supported bythe National Key R&D Program of China,No.2019YFC1 315800;National Natural Science Foundation of China,No.82 170555;Shanghai Rising-Star Program,No.19QA1 401900;Major Project of Shanghai Municipal Science and Technology Committee,No.19441 905200;Shanghai Sailing Program of the Shanghai Municipal Science and Technology Committee,No.19YF1 406400;and the 74th General Support of China Postdoctoral Science Foundation,No.2023M740675.
lnstitutional review board statement:This study was approved by the Ethics Committee of the Zhongshan Hospital,in accordance with the Declaration of Helsinki (B-2018-222).
lnformed consent statement:Informed consent was obtained from all patients.
Conflict-of-interest statement:All authors have no conflicts of interest or financial ties to disclose.
Data sharing statement:The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Pei-Yao Fu 0000-0002-8816-651X;Shi-Yao Chen 0000-0002-0873-9198;Yun-Shi Zhong 0000-0001-8382-3747;Yi-Qun Zhang 0000-0001-5584-6503;Wei-Feng Chen 0000-0002-4485-9461;Wen-Zheng Qin 0000-0001-8617-5810;Jian-Wei Hu 0000-0002-7564-6979;Ming-Yan Cai 0000-0002-8155-3154;Li-Qing Yao 0000-0001-6900-6791;Quan-Lin Li 0000-0002-9108-8786;Ping-Hong Zhou 0000-0002-5434-0540.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Yu HG
 World Journal of Clinical Oncology2024年2期
World Journal of Clinical Oncology2024年2期
- World Journal of Clinical Oncology的其它文章
- Unlocking the potential-vitamin D in prostate cancer prevention
- Updates on management of gliomas in the molecular age
- Deregulation of interferon-gamma receptor 1 expression and its implications for lung adenocarcinoma progression
- Elucidating the molecular basis of ATP-induced cell death in breast cancer: Construction of a robust prognostic model
- ldentification of immune cell-related prognostic genes characterized by a distinct microenvironment in hepatocellular carcinoma
- Population-based X-ray gastric cancer screening in Hiroshima prefecture,Japan