
Pregnancy and fetal outcomes of chronic hepatitis C mothers with viremia in China
2022-09-26 12:26CalvinPanBaoShenZhuJianPingXuJianXiaLiLiJuanSunHongXiaTianXiHongZhangSuWenLiErHeiDai
World Journal of Gastroenterology 2022年34期
Calvin Q Pan, Bao-Shen Zhu, Jian-Ping Xu, Jian-Xia Li, Li-Juan Sun, Hong-Xia Tian, Xi-Hong Zhang, Su-Wen Li, Er-Hei Dai
Abstract
Key Words: Hepatitis C virus viremia; Mother-to-child transmission; Pregnancy complications; Maternal health; Infant hepatitis C virus infection
lNTRODUCTlON
Hepatitis C virus (HCV) infection is a common infectious disease that affects the liver and remains a significant global health burden[1]. Although spontaneous viral clearance may occur in approximately 15% of patients who have acute HCV infection, the majority develop a chronic HCV infection. Among patients who have chronic hepatitis C, approximately 10%-15% will progress to cirrhosis within the first 20 years of infection, which eventually becomes decompensated without appropriate therapy and places them at high risk of developing liver cancer[2]. The prevalence of antibodies to HCV (HCV-Ab) in pregnant women is 0.1% to 2.4%, although it is much higher in some endemic areas[3]. The proportion of pregnant women with HCV-Ab positivity and active infection with viremia is approximately 60% to 70%[3].
Globally, up to 8% of pregnant women are infected with HCV in highly endemic areas[4]. In the United States, surveillance published in 2017 revealed a nationwide increase in HCV infection among pregnant women, which is an increasing but potentially modifiable threat to maternal and child health[5]. The proportion of infants born to HCV-infected women is also increasing in the United States[6]. It has been reported that vertical transmission is the most common mechanism of HCV infection in children, occurring in approximately 6% of infants born to women with HCV infection[7]. The risk of HCV vertical transmission increases if the maternal serum HCV viral load is above 105copies/mL[8,9].In addition, published studies have suggested that vertical transmission encompasses several potential transmission routes from an infected woman to her newborn, including intrauterine, intrapartum, and postnatal routes[10-13]. According to the American Association for the Study of Liver Diseases guidelines, all pregnant women should be tested for HCV infections, ideally at the time of initiation of prenatal care[14].
Although HCV affects a significant number of pregnant women, there are limited data regarding the impact of HCV active infection on pregnancy and infant outcomes. Prior studies of HCV and pregnancy have focused on the vertical transmission rates of HCV infection using limited assessments of the effects of chronic HCV infections on maternal health, complications during delivery, and fetal complications[15]. Therefore, there are data gaps in supporting strategies for the clinical management of mothers with HCV infections during pregnancy. Additionally, the identification of adverse consequences could improve current perinatal care and monitoring recommendations. With that in mind, we conducted a retrospective cohort study to compare the frequency and severity of adverse maternal outcomes during pregnancy, as well as fetal and infant outcomes, between mothers with HCV viremia and healthy mothers.
MATERlALS AND METHODS
Study design, setting, and patient selection
This is a single-center retrospective observational cohort study conducted at a tertiary referral university hospital located in Shijiazhuang city of Hebei province in China, which receives referrals from different levels of community medical clinics and health facilities in the city. The study site mainly included mothers with infectious diseases, including hepatitis B, hepatitis C, and human immunodeficiency virus(HIV). The Institutional Review Board approved the study, and the need for informed consent was waived. Local standards of care for prenatal care include regular clinic visits approximately every 4 to 6 wk during pregnancy for mothers who are infected with chronic viral hepatitis. Mothers received a symptom-directed physical exam, blood tests, and ultrasonography exams from the early second trimester to delivery. Viral hepatitis and HIV screening were performed at the first prenatal visit (often during the first or early second trimester), and hospital delivery was mandated in the entire province except in an emergency event.
In the current study, patients who attended the services in the prenatal care clinic from November 1,2011 to May 31, 2020 were screened for eligibility. Adult patients (age > 18 years old) who had a diagnosis of HCV-Ab positivity for at least six months and detectable levels of HCV RNA (> 15 IU/mL)during prenatal screening were eligible for enrollment. Major exclusion criteria were the following:Coinfection with hepatitis B virus, hepatitis D virus, or HIV; current or history of intravenous drug use or sexually transmitted diseases; liver cancer; autoimmune liver disease; primary biliary cirrhosis; and alcohol-related liver diseases (consumption of more than 20 g/day of alcohol for > 5 years). Patients with other liver diseases, including inherited liver diseases and drug-induced liver injury, were also excluded. For each patient included in the HCV group, a healthy mother was identified and selected from the Delivery Suite Registry at random. The selection was based on their infants' date of birth (± 30 d) matched to those of the HCV mothers with similar baseline values (matched for gestational days and parity). Based on the ratio of approximately 1:1 to match the number of subjects enrolled in the HCV group, a similar number of subjects was included in the healthy mother group. All patients included in the study were not smoking, drinking alcohol, or using any recreational drugs since these variables may affect the infants' outcomes.
Laboratory measurements for subjects in the study were all performed by the central laboratory in the medical center. HCV-Ab was tested by a chemiluminescent microparticle immunoassay (Autobio,Zhengzhou, China). Serum HCV RNA levels were measured with the real-time quantitative polymerase chain reaction method by using the Cobas TaqMan polymerase chain reaction assay according to the laboratory manuals (Roche Diagnostics, United States). An undetectable level was defined as below the lowest level of quantitation = 15 IU/mL. The comprehensive chemistry panel was tested using a HITACHI 7600 fully automatic biochemical analyzer, with the ULN of alanine aminotransferase (ALT)set at 40 U/L (Wako Pure Chemical Industries, Ltd. Japan).
Patient data collection and outcome assessment
Using an electronic medical record system and paper charts, we collected the following maternal data:Patients’ demographic information and pertinent clinical data, including a history of liver disease or hepatocellular carcinoma, pregnancy or obstetric complications; medication lists; positive physical findings, including pelvimetry, labor outcomes, and modes of delivery; laboratory results of completed blood count, coagulation tests, chemistry panels with ALT, and virological tests; and imaging results if available. Pertinent data were assessed at all visits starting from gestational week 12 with a four-week interval before delivery, at delivery, and at postpartum weeks 12, 24, and 36. Perinatal information for fetal development, including birth weight, height, Apgar scores, gestational age, and perinatal complications such as birth trauma and neonatal jaundice, was extracted from the neonatal records. Infant outcomes, such as intrauterine growth restriction, birth defects, macrosomia, low birth weight, and meconium staining stool, were collected.
The primary assessment was to analyze the frequency of maternal complications (both pregnancy and obstetrics complications) and negative fetal outcomes in HCV-infected mothers with viremiavsthose in healthy mothers. In addition, vertical transmission rates were analyzed among mothers with HCV infection. Secondary assessments were the association between demographic or clinical features and negative maternal or fetal outcomes in a multivariable logistic regression analysis. The current study used the following criteria to define the vertical transmission of HCV and considered the transmission confirmed if any of the following occurred: (1) Detection of HCV RNA in an infant who is 3 to 6 months old; (2) Detection of HCV RNA in the infant on at least 2 occasions; (3) Finding elevated serum aminotransferase levels in an HCV-Ab positive child (ULN = 40 U/mL); or (4) Confirming an identical viral genotype between mother and child[3].
Statistical analysis
Data analyses were performed using the Statistical Package for Social Science for Windows, Version 25.0(SPSS Inc., IBM, New York, United States). Frequencies and percentages were used to summarize the categorical variables. Fisher’s exact tests or chi-squared tests were used when comparing data between and within groups. Depending on the underlying distribution of the data, descriptive values are expressed as the means ± SD or medians and interquartile ranges. The student's t-test was used to assess continuous variables between groups. The maternal outcomes or infant outcomes were calculatedperpregnant mother and/orperinfant when appropriate. The baseline demographic or characteristic variables were analyzed as independent variables, whereas the negative maternal or infant outcomes were considered dependent variables. Risk factors identified from the univariate analysis (Pvalue <0.05) were further analyzed in the multivariate logistic regression model. The aforementioned risk factors associated with negative outcomes are presented with crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs). All tests were two-tailed with a 95%CI, and aPvalue < 0.05 was considered significant.
RESULTS
Patient characteristics
Among the 122 consecutive HCV antibody-positive pregnant women screened, 30 were not eligible due to undetectable levels of HCV RNA throughout the pregnancy. In addition, 13 patients were excluded because they were coinfected with HIV (n= 6) or hepatitis B virus (n= 7). As a result, seventy-nine patients who had HCV viremia during pregnancy were eligible for the HCV group. In addition, 115 healthy mothers were identified and selected from the Delivery Suite Registry at random (delivery date± 30 d matched to those cases in the HCV-infected group with similar baseline variables). As a result,our cohort consisted of 194 pregnant women with 79 and 115 mothers in the HCV group and a healthy mother (noninfected) group, respectively. The patient selection process is shown in Figure 1. All patients in the HCV group had no clinical indicator for liver decompensation. The clinical characteristics of the study patients are presented in Table 1. The demographic characteristics were well matched between the two groups in the majority of variables, including pre-pregnancy mean BMI, the number of parities or pluralities, mean gestational days, and mean ALT at delivery. However, mothers in the healthy group had a significantly older mean age (29.4 ± 4.9vs25.8 ± 4.7 years,P< 0.001), a low frequency of intertuberous diameter < 8.5 cm (29.6%vs48.1%,P= 0.009) and were taller (160.9 ± 4.0vs159.6 ± 3.8 cm,P< 0.001) than those in the HCV group.
Maternal outcomes
Data from gestational week 12 to delivery about pregnancy or obstetric complications and maternal laboratory abnormalities were analyzed. The following pregnancy and obstetric complications were identified in both groups (Table 2): Preterm labor, preeclampsia, eclampsia, gestational hypertension,anemia, abnormal renal or thyroid function, oligohydramnios, gestational diabetes, nuchal cord,umbilical cord prolapses, postpartum hemorrhage, premature rupture of membranes, and cesarean section due to medical needs. When comparing the aforementioned outcomes or laboratory abnormalities between the HCV-infected and healthy individuals, a significantly higher frequency of anemia during pregnancy was observed in the HCV group [19.0% (15/79)vs2.6% (3/115),P< 0.001]. In addition, a significantly higher frequency of nuchal cords [34.2% (27/79)vs9.6% (11/115);P< 0.001]and cesarean sections due to medical needs [48.1% (38/79)vs27.8% (32/115);P= 0.004] was reported in the HCV group. The frequencies of other pregnancy or obstetric complications did not differ between the two groups (Table 2).
Fetal and infant outcomes
When comparing the fetal and infant outcomes between the HCV-infected and healthy mother groups(Table 3), we observed a significantly lower mean ± SD body weight in neonates who were born to HCV-infected mothers (3105.1 ± 459.4vs3278.3 ± 462.0 gms;P= 0.006). However, the frequency of lowbirth weight (< 2500 g) did not differ between the two groups [8.9% (7/79)vs3.5% (4/115);P= 0.20].The other variables did not differ between the two groups. In addition, neonates in the HCV group had a significantly smaller mean head circumference (33.1 ± 0.7vs33.3 ± 0.6 cm;P= 0.03). The other measurements did not differ between the two groups, which included gestational weeks, the percentage of neonates that reached full-term or small for gestational age at delivery, and the mean height at birth.There were no miscarriages, stillbirths, birth defects, or Apgar scores < 7 at 5 min after birth in the entire cohort.

Table 2 Maternal outcomes in the hepatitis C virus viremic group vs the control group
Among infants who were born to HCV-infected mothers, all were tested HCV-Ab positive at birth,and one had a detectable level of HCV RNA (2165 IU/mL). All infants in the study cohort were breastfed. Their HCV-Ab became negative beyond six months, except for the one who had HCV viremia at birth. This infant continued to have HCV antibodies and detectable levels of HCV RNA measured at the ages of three months and nine months, meeting the criteria of chronic hepatitis C infection. The HCV transmission rate in our study was 1.3% (n= 1/79). In the review of maternal characteristics, the mother was 25 years old with a maternal HCV RNA level of 2.58 × 5 Log10IU/mL at delivery. She had a history of blood transfusion and was diagnosed with chronic HCV infection during prenatal screening. Her pregnancy was uneventful, with normal levels of ALT throughout the entire pregnancy. She delivered a girl with normal physical development at gestational week 39 plus 5 d.
Risk factors associated with negative outcomes
When comparing the pregnancy and obstetric complications between the two groups, we found that a significantly higher frequency of anemia, nuchal cord, and cesarean section due to medical needs occurred among HCV-infected mothers. The crude and adjusted ORs with 95%CIs of each risk factor are presented in Table 4. The analyses indicated that HCV infection was the only factor associated with anemia (adjusted OR: 18.1, 95%CI: 4.3-76.6), increased numbers of C sections due to medical needs(adjusted OR: 2.6, 95%CI: 1.4-4.9), and nuchal cords during pregnancies (adjusted OR: 5.6, 95%CI: 2.4-13.0). Since a significantly smaller head circumference and lower mean birth weight were the only two negative fetal outcomes identified in infants from HCV-infected mothers, we analyzed the maternal risk factors (Table 5) and found that maternal HCV infection was associated with these negative outcomes.The adjusted ORs of maternal HCV infection associated with a smaller head circumference and birth weight ≤ 3250 gms were 2.1 (95%CI: 1.1-4.3) and 2.2 (95%CI: 1.2-4.0), respectively.
DlSCUSSlON
Although HCV vertical transmission can occur in up to 5.8% of mother-infant pairs[16], many children can clear HCV infection spontaneously[17]. The disease can also be cured with oral antiviral therapy starting at the age of 3[17]. Therefore, the clinical landscape of managing HCV-infected mothers has recently shifted from addressing HCV vertical transmission to the assessment and management of negative pregnancy or neonatal outcomes. Published studies have linked several negative pregnancy outcomes to maternal HCV infection, including intrahepatic cholestasis[18-20], gestational diabetes[21-23], the premature rupture of the membranes[24,25], the requirement for cesarean delivery[24,25],preterm delivery[23], small for gestational age[26], and low birth weight[26]. However, its effect on restriction or disturbance of intrauterine fetal growth remains inconclusive[21,23,26-28].

Table 3 The fetal and infant outcomes in the two study groups

Figure 1 Flow Chart for patients enrolled in the study. Data analyses included 194 patients. Among the 122 patients with hepatitis C antibody positive evaluated, 79 were eligible and enrolled. A control group with healthy uninfected patients (n = 115) was selected to match the infected patients. Patients were divided into two groups: a hepatitis C patient group and a healthy control group comparison. HCV: Hepatitis C virus; HBV: Hepatitis B virus; HIV: Human immunodeficiency virus.
Our study assessed both maternal and fetal outcomes in viremic mothers with HCV infections. To our knowledge, this is the first study from China to assess pregnancy outcomes in HCV viremic mothers.We found that HCV might be associated with a higher frequency of nuchal cords and a smaller neonatalhead circumference, which has not been reported in the literature before. We also found that HCV viremia was linked to pregnancy anemia, cesarean sections due to medical needs, and low gestational weight in neonates. In addition, we observed that lower birth weight was associated with maternal infection, which was consistent with published data from the United States and Europe[23,26]. In the context of all infants in our study being breastfed, the HCV vertical transmission rate was 1.27%, which was within the range (0.2%-6%) of the already published studies[16,29].

Table 4 Risk factors associated with obstetric complications
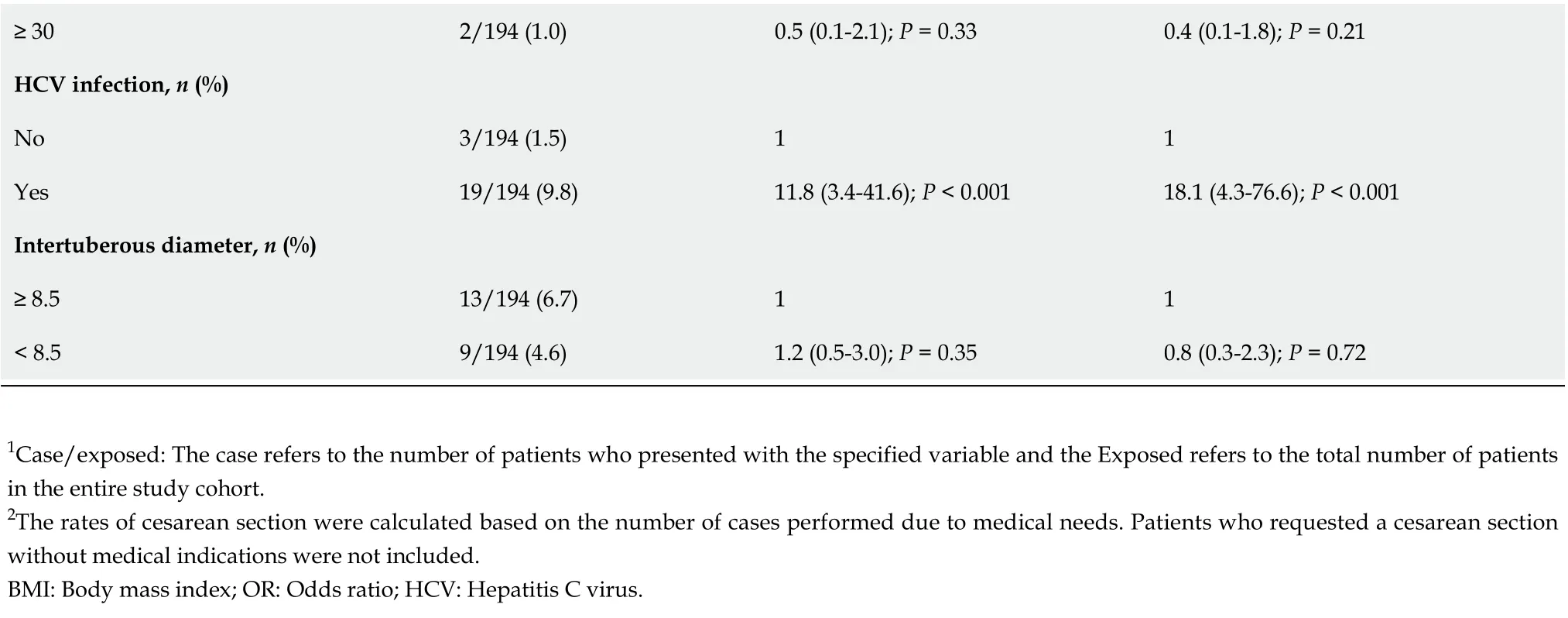
≥ 302/194 (1.0)0.5 (0.1-2.1); P = 0.330.4 (0.1-1.8); P = 0.21 HCV infection, n (%)No 3/194 (1.5)11 Yes 19/194 (9.8)11.8 (3.4-41.6); P < 0.00118.1 (4.3-76.6); P < 0.001 Intertuberous diameter, n (%)≥ 8.513/194 (6.7)11< 8.59/194 (4.6)1.2 (0.5-3.0); P = 0.350.8 (0.3-2.3); P = 0.72 1Case/exposed: The case refers to the number of patients who presented with the specified variable and the Exposed refers to the total number of patients in the entire study cohort.2The rates of cesarean section were calculated based on the number of cases performed due to medical needs. Patients who requested a cesarean section without medical indications were not included.BMI: Body mass index; OR: Odds ratio; HCV: Hepatitis C virus.
Early studies by Jafferyet al[30] and Bohmanet al[31] found that fetal outcomes did not differ between HCV-positive mothers and healthy controls[30,31]. However, in a study by Salemiet al[29], the risk of an adverse neurological outcome was higher in infants born to HCV mothers, including feeding difficulties (OR: 1.32, 95%CI: 1.06-1.64) and neonatal seizures (OR: 1.74, 95%CI: 0.98-3.10)[29]. The aforementioned studies have limitations of lacking a well-defined study population because the diagnosis of HCV was based on the HCV antibody, and HCV RNA was not always tested. Paternosteret al[24] observed that intrahepatic cholestasis was more common in HCV-RNA-positive mothers than in HCV-RNA-negative mothers, suggesting that HCV viremia may lead to different outcomes[19]. In addition, cofounders such as intravenous drug use or sexually transmitted diseases may not be adjusted in studies based on pregnancy registries[26,32]. These factors could contribute to the discrepancies among the study findings. In the context of the paucity of data and infrequency of fetal negative events,Huanget al[33] performed a meta-analysis and found that low birth weight was linked to maternal HCV infection (OR: 1.97, 95%CI: 1.43-2.71)[33].
In our study, birth weight ≤ 3250 gms was associated with HCV exposure. There was also a trend of HCV-exposed neonates with a birth weight of < 2500 gms. More importantly, our cohort demonstrates a previously unreported association between maternal HCV viremia and a smaller neonatal head circumference. Our findings provide new evidence supporting the intrauterine restriction of fetal growth in a well-defined HCV population, which enrolled only HCV-infected mothers with detectable levels of HCV RNA who had no history of intravenous drug use or sexually transmitted diseases.
Although the mechanism of fetal growth restriction is not fully understood, several studies have suggested that HCV-induced inflammation in the placenta may cause fetal development restriction. In anin vitrostudy, HCV infected a human cytotrophoblast and changed its ultrastructure dramatically upon infection[33]. In addition, Hurtadoet al[34] observed that the cytotoxicity of natural killer cells and natural killer T cells was enhanced in the placenta, and placental natural killer T-cell cytotoxicity was further increased by HCV infections[34]. Several population-based retrospective cohort studies reported higher rates of gestational diabetes in HCV-infected mothers than in noninfected mothers[35,36], but the association was limited to women with excessive weight gain during pregnancy. Our study did not show such complications, which is likely because our patients are Asians with a much lower body mass index than those in other studies[21,24,26].
In this cohort study, some limitations should be addressed. Being a single-center retrospective design,this study has a limited capacity when adjusting or balancing all covariates between the HCV-exposed and HCV nonexposed groups. Additionally, we did not have HCV genotype data. However, published studies in China indicated that the majority of Chinese patients with HCV had genotype 1[36]. Second,cohort data about HCV antibody-positive but nonviremic mothers are limited: These mothers were not enrolled in our study due to the small number of patients in our center (n= 30, Figure 1). Further studies in this subgroup will add to the understanding of pregnancy outcomes. Third, the liver fibrosis stages for patients with HCV infection were not assessed in this study, although all patients had no clinical indications of liver decompensation. Therefore, future studies might be needed to investigate whether HCV-infected patients with advanced fibrosis have negative maternal and fetal outcomes. Last, the frequency of negative events in HCV-infected mothers could be underestimated due to the maternal mean age being younger than that of healthy mothers.

Table 5 Risk factors associated with fetal negative outcomes
CONCLUSlON
In conclusion, our study demonstrates a previously unreported association between maternal HCV viremia and a smaller neonatal head circumference. Given our new findings on the intrauterine restriction of fetal growth from HCV exposure, screening all mothers during pregnancy for HCV should be a mandatory practice. More importantly, our findings indicate a need for close antenatal surveillance for maternal complications and delayed fetal development in HCV mothers with viremia. Last, our data support that preconception health management should include HCV screening, so HCV infection can be treated before pregnancy to improve the health of both the mothers and infants.
ARTlCLE HlGHLlGHTS
Research background
Hepatitis C virus (HCV) infection remains a significant global health burden, and there is a high proportion of women with antibodies to HCV positive whose active infection with viremia. In addition,HCV infection among pregnant women is an increasing but potentially modifiable threat to maternal and child health.
Research motivation
Although HCV affects a significant number of pregnant women, there is limited data regarding the impact of HCV active infection on pregnancy and infant outcomes. Therefore, there are data gaps in supporting strategies for clinical management of mothers with HCV infections during pregnancy.
Research objectives
We conducted a retrospective cohort study to compare the frequency and severity of adverse maternal outcomes during pregnancy, as well as fetal and infant outcomes between mothers with HCV viremia and healthy mothers.
Research methods
A retrospective observational cohort study was conducted to compare pregnancy and fetal outcomes of HCV-viremic mothers with those of healthy mothers. After HCV mothers with viremia and healthy mothers were enrolled, we collected their demographic information and pertinent clinical data using an electronic medical record system and paper charts. Perinatal information for fetal development and infant outcomes were extracted from the neonatal records. Data analyses were performed using the Statistical Package for Social Science for Windows, Version 25.0 (SPSS Inc., IBM, New York, United States).
Research results
Our study enrolled 79 viremic mothers and 115 healthy mothers. Compared to healthy mothers, HCV mothers had a significantly higher frequency of anemia, caesarian section, and nuchal cords during pregnancy. In addition, the mean neonatal weight and head circumference in the HCV group was significantly lower. In a multivariate model, similar results were found.
Research conclusions
Our study demonstrates the association between maternal HCV viremia and a smaller neonate head circumference. We also confirmed the high frequency of pregnancy and obstetric complications in HCV viremic mothers.
Research perspectives
Multi-center and large sample studies are needed to verify these results in the future and to investigate if HCV-infected patients with advanced fibrosis have negative maternal and fetal outcomes.
ACKNOWLEDGEMENTS
We thank the medical staff in the Department of Obstetrics and Gynecology, The Fifth Hospital of Shijiazhuang, for their support and assistance during our study. We also like to thank Mr. Andrew Park(Northern Valley Regional High School at Old Tappan, United States) for proofreading the manuscript.
FOOTNOTES
Author contributions:Pan CQ provided the concept and designed the study, wrote the manuscript, communicated with the journal, and addressed comments from reviewers; Dai EH and Zhu BS obtained the funding and supervised the study; Pan CQ, Zhang XH, and Dai EH performed data analyses; All other authors contributed to the data collection.
Supported byThe Ministry of Science and Technology of China for the National Five-Year Key Projects in Infectious Diseases, No. 2015ZX10004801.
lnstitutional review board statement:The study was reviewed and approved by the Institutional Review Board of the Fifth Hospital of Shijiazhuang in China.
lnformed consent statement:The informed consent was waived.
Conflict-of-interest statement:Dr. Pan received grants from Gilead. He also serves as a speaker for Gilead and Abbvie. Other authors have nothing to be disclosed.
Data sharing statement:The authors agree to share anonymized Individual Patient Data (IPD) upon request or as required by law and/or regulation with qualified external researchers. Approval of such requests is at the authors’discretion and is dependent on the nature of the request, the merit of the research proposed, the availability of the data, and the intended use of the data. Data requests should be sent to Erhei Dai MD at email: daieh2008@126.com
STROBE statement:The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Calvin Q Pan 0000-0002-3723-6688; Er-Hei Dai 0000-0001-8835-6199.
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
 World Journal of Gastroenterology2022年34期
World Journal of Gastroenterology2022年34期
- World Journal of Gastroenterology的其它文章
- Therapeutic strategies for post-transplant recurrence of hepatocellular carcinoma
- Spontaneous expulsion of a duodenal lipoma after endoscopic biopsy: A case report
- Trends in hospitalization for alcoholic hepatitis from 2011 to 2017: A USA nationwide study
- Analysis of invasiveness and tumor-associated macrophages infiltration in solid pseudopapillary tumors of pancreas
- lmpact of adalimumab on disease burden in moderate-to-severe ulcerative colitis patients: The one-year, real-world UCanADA study
- Diagnosis, treatment, and current concepts in the endoscopic management of gastroenteropancreatic neuroendocrine neoplasms