Differential diagnosis of benign and malignant breast lesions using quantitative synthetic magnetic resonance imaging
2022-05-06 07:19:32ZHANGLiyingZHAOXinYINXing
南方医科大学学报 2022年4期
INTRODUCTION
According to the GLOBOCAN 2018 estimates,breast cancer is the most frequently diagnosed cancer in women globally and shows an increasing trend annually.Early detection of breast cancer is the basis of standardized treatment and mortality burden reduction.Magnetic resonance imaging (MRI) is an important diagnostic modality for evaluating breast lesions and screening of high-risk patients,but the results based on visual evaluation sometimes remain subjective.In spite of its high sensitivity,MRI has only a moderate specificity for distinguishing between benign and malignant breast lesions,and its heterogeneous imaging findings for non-specific breast lesions often lead to misdiagnosis and subsequent unnecessary surgical treatment or treatment delays.
So one Sunday the White Bear came and said that they could now set out to see her father and mother, and they journeyed thither5, she sitting on his back, and they went a long, long way, and it took a long, long time; but at last they came to a large white farmhouse6, and her brothers and sisters were running about outside it, playing, and it was so pretty that it was a pleasure to look at it.
Synthetic MRI (SyMRI) is a compilation pulse sequence using a multi-echo and multi-delay acquisition method for simultaneous quantification of the quantitative values such as T1 and T2 relaxation times and proton density (PD) image map from a single acquisition.So far only a few reports have been available to document the use of SyMRI for evaluating breast lesions with inconsistent results.
The purpose of this study was to assess the feasibility of using the quantitative parameters generated by SyMRI for differential diagnoses of benign and malignant breast lesions and to build an effective diagnostic model for breast cancer based on multiparametric MRI.
No, as soon as the light shone in the evening from the attic it seemed to him as though its beams were strong ropes dragging him up, and he had to go and peep through the key-hole
METHODS
Patients
One Friday evening I came home from work to find a big beautiful German shepherd on our doorstep. This wonderful strong animal gave every indication that he intended to enter the house and make it his home. I, however, was wary4. Where did this obviously well-cared-for dog come from? Was it safe to let the children play with a strange dog? Even though he seemed gentle, he still was powerful and commanded respect. The children took an instant liking5 to German and begged me to let him in. I agreed to let him sleep in the basement until the next day, when we could inquire around the neighborhood for his owner. That night I slept peacefully for the first time in many weeks.
All the imaging data were processed using Advantage Workstation (ADW 4.7 version,GE,US).Two radiologists with more than 7 years of diagnostic experience with breast MRI independently reviewed the films.Both readers were blinded to the patients' clinical and pathological results.
MRI protocol
All the breast MR images were acquired using a 3.0 T MR scanner (SiGNAPioneer,GE Healthcare,USA)and an 8-channel phased-array breast coil.Before the scan,the patients lay in a prone position with their feet going in first.The scan was performed with an initial SyMRI sequence after routine plain scan followed by the DCE-MRI sequence and then by a second SyMRI sequence after contrast agent administration.
As a mature and important modality for detecting breast masses,MRI remains insufficient to fully characterize the lesions.Our study showed that among all SyMRI-generated quantitative parameters,T2p combined with T1e had a better performance than ΔT1% alone for differentiation of benign and malignant breast lesions,and they both can be used to increase the diagnostic efficiency of DCE-MRI.
Image analysis
In one hand she held a sceptre, and in the other the imperial globe, and on either side of her stood two rows of halberdiers, each smaller than the other, from a seven-foot giant to the tiniest little dwarf25 no higher than my little finger
Of the 95 breast lesions,27(28.4%)were categorized as benign and 68 (71.6%) as malignant lesions.The mean sizes of the benign and malignant lesions were 21.6±6.3 mm and 23.3±6.3 mm,respectively.The benign group consisted of 19 fibroadenomas,4 adenosis,2 sclerosing adenosis,1 intraductal papilloma,and 1 phyllodes tumor.The 68 malignant lesions included 5 ductal carcinomas,61 invasive ductal carcinomas,1 mucinous carcinoma,and 1 metaplastic carcinoma.
Statistical analysis
Statistical analyses were performed using MedCalc for Windows (version 20.0;MedCalc Software,Ostend,Belgium) and R version 4.1.0 (R Foundation for Statistical Computing,Vienna,Austria).R packages MASS and leaps were used.The enrolled patients were divided into benign and malignant groups according to their pathological results.All the continuous variables were presented as,while the categorical variables were shown as total and proportion.Interobserver consistencies for all quantitative parameters between the two radiologists were evaluated using intraclass correlation coefficient (ICC) analysis,and the agreement was defined as good (ICC>0.75),moderate (ICC=0.5-0.75),or poor (ICC<0.5).Feature selection was based on univariate analyses and all-subset regression,and binary logistic regression was performed to build diagnostic models for differentiation of benign and malignant breast masses.Receiver operating characteristic(ROC) analyses were performed to evaluate the diagnostic performance of each group.The sensitivity,specificity,accuracy,positive predictive value (PPV),and negative predictive value(NPV)were calculated.For all the tests,avalue less than 0.05 was considered to indicate a statistically significant difference.
RESULTS
Clinicopathological data
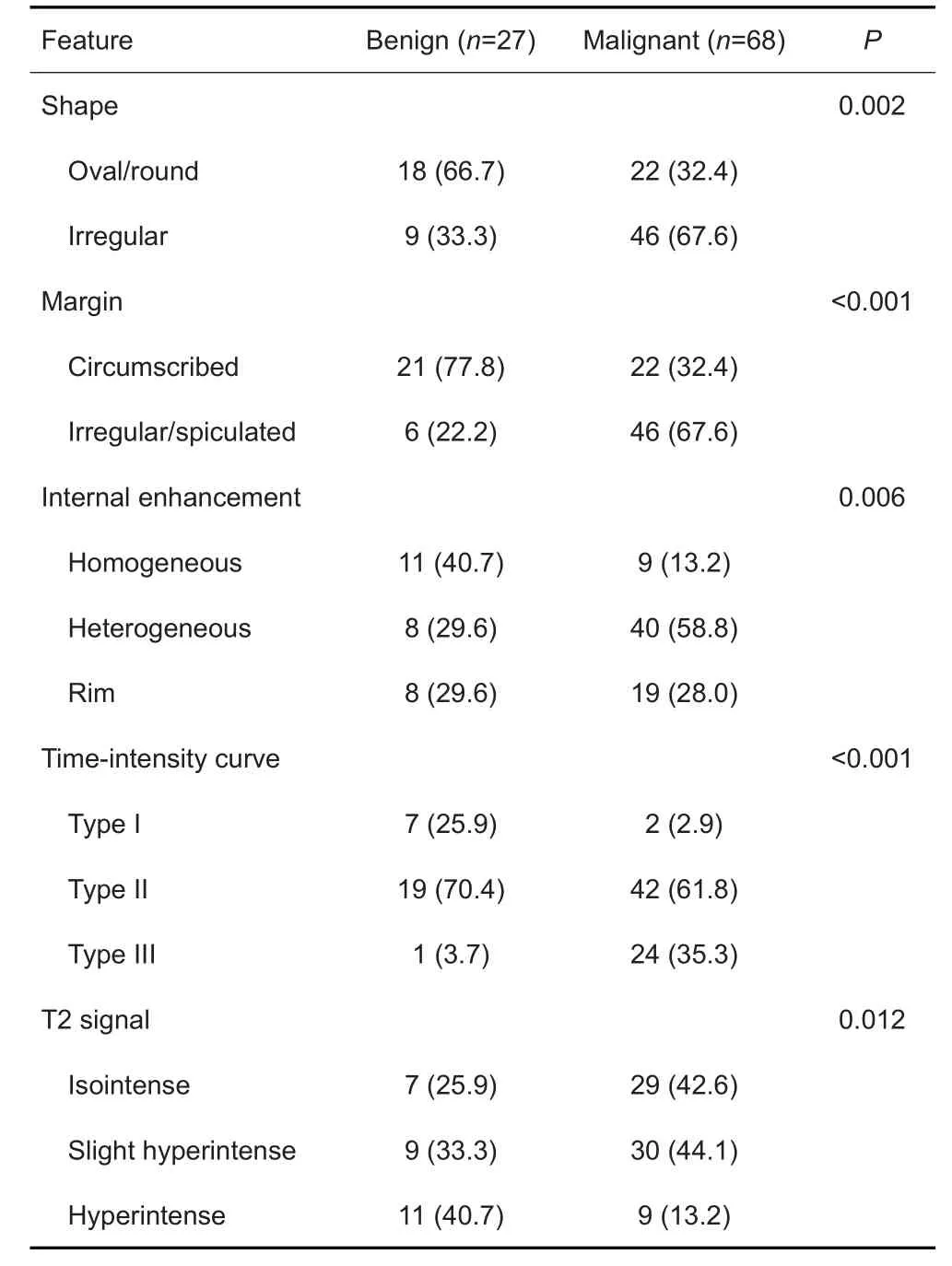
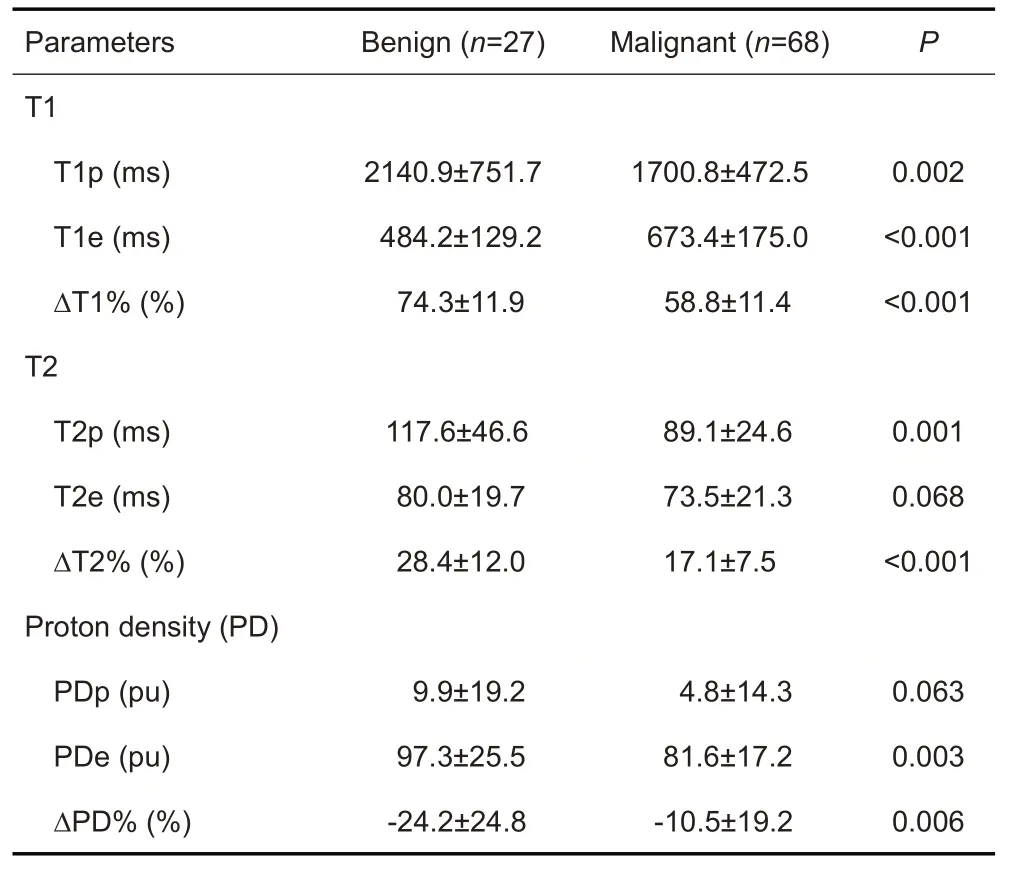
The morphological and kinetic features of the findings were described using the American College of Radiology Breast Imaging Reporting and Data System in DCE-MRI.Lesions were characterized on the basis of their shape,margin,internal enhancement,T2WI signal,and time intensity curve (TIC) pattern.SyMRI-generated quantitative parameters (T1,T2,and PD values) were automatically measured by drawing the region of interest(ROIs) on SyMRI.By comparison with DCE-MRI,the enhanced solid portion of the lesion was used to site the circular two-dimensional ROI at approximately the same slice by both radiologists,and the two measurements were averaged and used as the quantitative parameters before and after the administration of the contrast agent(recorded as T1p,T2p,PDp,and T1e,T2e,Pde,respectively).The relative change rate was calculated according to the equation(as for T1 value):ΔT1%=(T1p-T1e)/T1p×100%.
DCE-MRI features
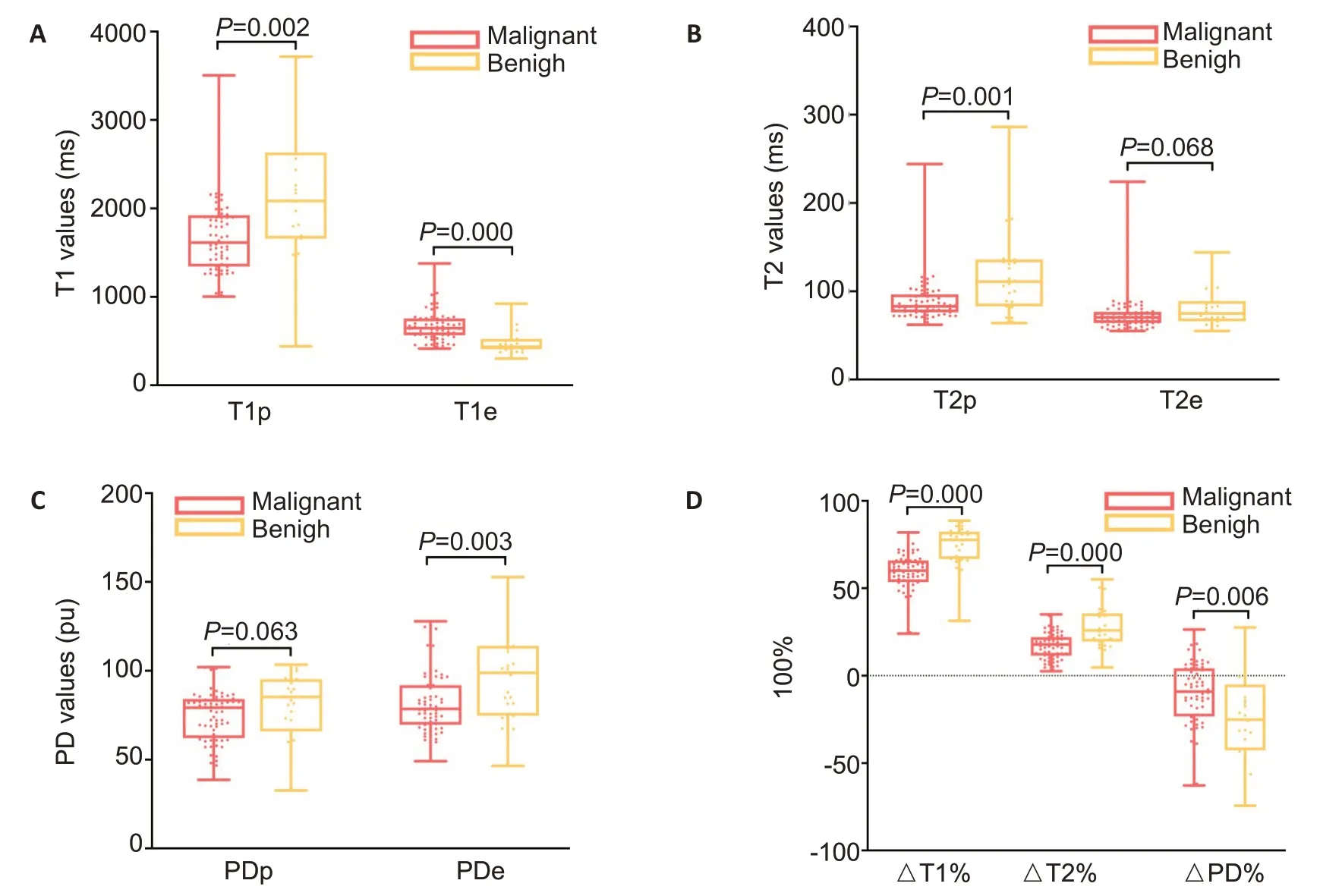
The ICCs between the two radiologists for T1,T2,and PD values before and after contrast agent administration were all greater than 0.75 (range,0.826-0.959;<0.05),indicating good agreement.On SyMRI,malignant lesions showed lower average quantitative values except for T1e before and after contrast agent administration as compared with benign lesions.Representative benign and malignant mass lesions are shown in Fig.1.Univariate analysis showed no significant differences in T2e or PDp values between benign and malignant groups(>0.05).The relative change rates (ΔT1%,ΔT2%,and ΔPD%) were all significantly lower in malignant group than in benign group(<0.05;Tab.2 and Fig.2).
This study was approved by our institutional review board and informed consent was waived due to the retrospective nature of the study.A total of 147 consecutive women with breast mass lesions admitted in our hospital between January,2020 and May,2021 were initially included.All the patients underwent preoperative examination with SyMRI.The exclusion criteria were as follows:patients who underwent surgery or neoadjuvant treatment before breast MRI examination(=20);patients with incomplete scans or those with noticeable movement artifacts affecting the diagnosis(=13);patients with non-mass enhancement lesions on dynamic contrast-enhanced MRI (DCE-MRI) (=9);patients with lesions not visible on SyMRI or smaller than 10 mm (=6);and patients without follow-up data or histopathologic confirmation of the lesions (=4).Therefore,the study included a total of 95 women(mean age of 42±9.2 years,range 30-66 years) with 95 lesions confirmed pathologically by core needle biopsy or surgical specimen examination.
SyMRI-generated quantitative parameters
On DCE-MRI,DCE morphological features of the breast cancer lesions presenting as masses included irregular shape,irregular/spiculated margin,heterogeneous/rim internal enhancement pattern,type II/III TIC,and isointense/slight hyperintense signal on T2WI (<0.05,Tab.1).

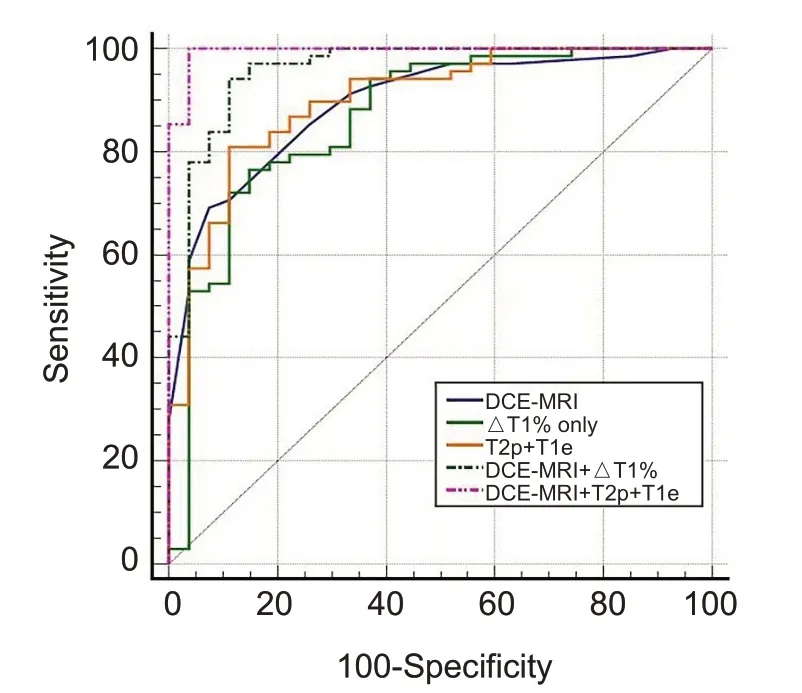
ROC curve analysis
For SyMRI,ΔT1% had the best performance as a single predictor for predicting malignancy with an area under the ROC curve (AUC) of 0.866 (95%:0.778-0.954).We subsequently examined all the possible combinations of the parameters based on all-subset regression and determined that the combination of all parameters from the conventional DCE-MRI with T2p and T1e from SyMRI was optimal for constructing the diagnostic models.In the combined DCE-MRI+SyMRI model,DCE-MRI+T2p+T1e had a good discriminatory power with an AUC of 0.995 (95%:0.985-1.000).The AUCs and ROC curves for these models are listed in Tab.3 and Fig.3.

DISCUSSION
The MRI parameters were as follows:for conventional non-contrast scan with axial T1WI sequence without fat saturation,the recovery time (TR)=750 ms,echo time(TE)=6.8 ms,and slice thickness=5 mm;for axial T2WI fat-saturated sequence,TR=6980 ms,TE=78 ms,and slice thickness=5 mm;for axial DWI sequence,TR=3000 ms,TE=50 ms,slice thickness=5 mm,and b value=0/1000 s/mm.Axial T1-weighted DCE-MRI sequences were obtained using threedimensional differential subsampling with Cartesian ordering technology for the breast.Of the 35 ultrafast phases (first phase,22 s;subsequent single-phase scanning time,8 s;total scan time,4 min 9 s),the first phase was acquired prior to contrast agent injection,and the following 34 phases were acquired immediately after and during contrast agent injection.The imaging parameters were:TR=5.2 ms,a dual TE=1.1 ms,2.2 ms,slice thickness=1.2 mm,and field of view(FOV)=360 mm×360 mm.Gd-DTPA was intravenously injected using a power injector at a dose of 0.1 mmol/kg at the rate of 3.0 mL/s,followed by 20 mL of saline flush at the same rate.SyMRI was performed before and after contrast injection using a multiple-dynamic,multiple-echo (MDME)sequence with the following parameters:TR=7097 ms,dual TE=21.4 ms/106.8 ms,slice thickness=5 mm,FOV=360 × 360 mm,bandwidth=156.2 Hz/pixel,and scan time=5 min.
3.Betrothed: To betroth1 or become betrothed is to contract to any one for a marriage; to engage or promise in order to marriage; to affiance (Webster s 1990).
Relaxation times are important tissue properties related with the physiological state,and studies have shown the clinical value of T2-mapping for differentiating benign and malignant lesions of the uterus and prostateand T1-mapping for evaluating myocardial and liver fibrosis.But these sequences require separate collection and long imaging time,and the reported studies failed to use a unified setting of the scanning parameters and yielded inconsistent findings.So far studies of SyMRI for differential diagnosis of malignancies remain limited,and their findings concerning the changes in T1,T2 and PD in malignant tissues are inconsistent.In this study,we found that both T1p and T2p in the benign breast lesions were significantly higher than those in malignant lesions.The inconsistency of the results from different studies may arise from the selection of ROI and the morphology of lesions and needs to be solved by further verification with a larger sample size.Previous studies have shown that free water contents is reduced in malignant lesions due to the presence of densely arranged proliferating cells and infiltration of lymphocytes into the extracellular space,which results in lower native T2 and T1 values in malignant than in benign lesions.This is consistent with the fact that most breast cancers show an isointense or slightly hyperintense signal on T2WI.We found that PDp value of malignant lesions was lower than that of benign lesions,but this difference was not statistically significant,possibly due to the inferior image quality of SyMRI compared with conventional plain scan sequencesand the irregular and fuzzy boundaries of the malignant lesions,which cause the inclusion of a small amount of normal breast tissue in the ROI.
We noted significant changes in the quantitative SyMRI values and their relative change rates (ΔT1%,ΔT2%,and ΔPD%) in enhanced breast cancer lesions.The larger T1e value and smaller Pde value of malignant lesions suggest the presence of massive new capillaries and incomplete vascular basement membrane,which leads to increased cell permeabilityand hence an increased contrast agent exchange;consequently,while there is a gradual recovery in T1 value of the malignant lesions,the contrast agent in benign lesions remain concentrated at 4 min after injection.Malignant lesions also showed significantly lower change rate of the quantitative values than benign lesions,which further confirms the above inferences.In addition,GTPA used for enhancement has a minor T2 effect,which was also observed in our study.
This study has some limitations.First,we only selected mass lesions with benign and malignant pathological types,and the non-mass-like breast lesions interspersed with normal glandular and lipid tissues were not studied.Second,small lesions that could not be accurately located based on SyMRI were excluded from the analysis,which may cause a sampling bias.Third,we did not use automatic image registration before and after enhancement to correct for the offset position between SyMRI and DCE-MRI,which may affect the stability of the analyzed data.Fourth,quantitative SyMRI values after the administration of GTPA may constantly change during image data collection.We only examined the effect of drug administration at one time point,and it can be possible that drug administration at an earlier or later time point may produce different results.
In conclusion,the quantitative parameters of the SyMRI sequence can reflect the intrinsic histological characteristics of breast cancer lesions and allows for differential diagnosis of benign and malignant breast masses.However,it is still necessary to combine morphological features and DCE-MRI findings for a comprehensive diagnostic analysis of the lesions.