不同入路下切开复位钢板内固定治疗在复杂盆骨髋臼骨折中的应用价值
2022-03-24 16:01:31王子一卢洋
中国医学创新 2022年3期
王子一 卢洋




【摘要】 目的:探討不同入路下切开复位钢板内固定治疗复杂盆骨髋臼骨折的效果。方法:选取2018年1月-2019年12月佳木斯市中医院收治的82例复杂盆骨髋臼骨折患者。根据切开复位手术入路分为对照组40例和研究组42例。对照组采取Kocher-Langenbeck(K-L)入路,研究组采取改良Stoppa入路联合髂嵴前入路,两组均切开复位后行钢板内固定。比较两组骨折复位情况;比较两组术后3、6、12个月的髋关节功能Harris评分和日常生活活动能力(ADL)评分;比较两组手术时间、手术出血量、术后住院时间以及术后并发症发生情况。结果:研究组骨折复位情况优于对照组,差异有统计学意义(P<0.05)。术后3、6、12个月,研究组Harris评分和ADL评分均大于对照组(P<0.05)。两组手术时间比较,差异无统计学意义(P>0.05)。研究组手术出血量低于对照组,术后住院时间短于对照组(P<0.05)。研究组术后并发症率为9.52%,与对照组的15.00%比较,差异无统计学意义(P>0.05)。结论:相比传统K-L入路,改良Stoppa入路联合髂嵴前入路能够更好地显露骨盆髋臼解剖结构,有利于复杂盆骨髋臼骨折的复位与固定,骨折复位良好,术后髋关节功能和日常生活能力恢复更佳。
【关键词】 盆骨髋臼骨折 Kocher-Langenbeck入路 Stoppa入路 髂嵴前入路 切开复位
[Abstract] Objective: To investigate the effect of open reduction and plate internal fixation in the treatment of complex pelvic acetabular fractures with different approaches. Method: A total of 82 patients with complex pelvic acetabular fractures admitted to Jiamusi Hospital of Traditional Chinese Medicine from January 2018 to December 2019 were selected. According to the open reduction approach, 40 cases were divided into control group and 42 cases were divided into study group. Kocher-langenbeck (K-L) approach was used in the control group, and modified Stoppa approach combined with preiliac crest approach was used in the study group. After open reduction, plate fixation was performed in both groups. Fracture reduction was compared between the two groups. Harris score of hip function and ADL at 3, 6 and 12 months after operation were compared between the two groups. The operative time, operative blood loss, postoperative hospital stay and postoperative complications were compared between the two groups. Result: Fracture reduction in the study group was better than that in the control group, the difference was statistically significant (P<0.05). At 3, 6 and 12 months after surgery, Harris scores and activity of daily living (ADL) scores in the study group were higher than those in the control group (P<0.05). There was no significant difference in operation time between the two groups (P>0.05). The amount of surgical bleeding in the study group was lower than that in the control group, and the postoperative hospital stay was shorter than that in the control group (P<0.05). The postoperative complication rate of the study group was 9.52%, compared with 15.00% of the control group, there was no statistical significance (P>0.05). Conclusion: Compared with traditional K-L approach, modified Stoppa approach combined with anterior iliac crest approach can better display the anatomical structure of the pelvis and acetabulum, which is conducive to the reduction and fixation of complicated pelvic and acetabular fractures, besides, fracture reduction, postoperative hip function recovery and activity of daily living are good.
[Key words] Pelvic and acetabular fractures Kocher-Langenbeck approach Stoppa approach Anterior iliac crest approach Open reduction
First-author’s address: Jiamusi Traditional Chinese Medicine Hospital, Heilongjiang Province, Jiamusi 154002, China
doi:10.3969/j.issn.1674-4985.2022.03.037
盆骨髋臼骨折的手术一般采用切开复位内固定治疗,需充分暴露视野,手术创伤大、难度高[1]。由于髋臼周围血管神经较多,解剖结构复杂,采取何种手术入路以获得最佳的术后解剖复位和功能复位、更好地恢复髋关节功能一直是临床研究的热点。对于复杂髋臼骨折,Kocher-Langenbeck(K-L)入路为临床应用最广泛的切开复位手术入路,但发生坐骨神经损伤、血管损伤、异位骨化的并发症发生率较高[2-3]。近年来新提出的改良Stoppa入路联合髂嵴前入路可以较好地暴露骨盆缘和四方区,充分显露骨盆髋臼解剖结构,便于复位,具有一定优势,适合于复杂髋臼骨折[4-5]。本研究探讨K-L入路、改良Stoppa入路联合髂嵴前入路下切开复位钢板内固定治疗复杂盆骨髋臼骨折的效果,并分析术后髋关节功能及骨折复位情况,为临床手术提供参考,现报道如下。
1 资料与方法
1.1 一般资料 选取2018年1月-2019年12月佳木斯市中医院收治的82例复杂盆骨髋臼骨折患者。纳入标准:符合盆骨髋臼骨折的诊断标准[6];年龄≥18岁;根据文献[7]中Letournel-Judet分型判断为复杂髋臼骨折,包括T形骨折、后壁+后柱骨折、横断+后壁骨折、前柱+后半横断骨折、双柱骨折;符合切开复位手术适应证;受伤至手术时间<14 d。排除标准:手术禁忌证;陈旧性骨折;严重骨质疏松;合并颅脑、胸、腹外伤;合并血管神经损伤;凝血功能障碍;合并严重心、脑、肝、肾疾病,或不能耐受手术。根据切开复位手术入路分为研究组42例和对照组40例。所有患者及家属均知情同意并签署知情同意书,本研究已经医院伦理委员会批准。
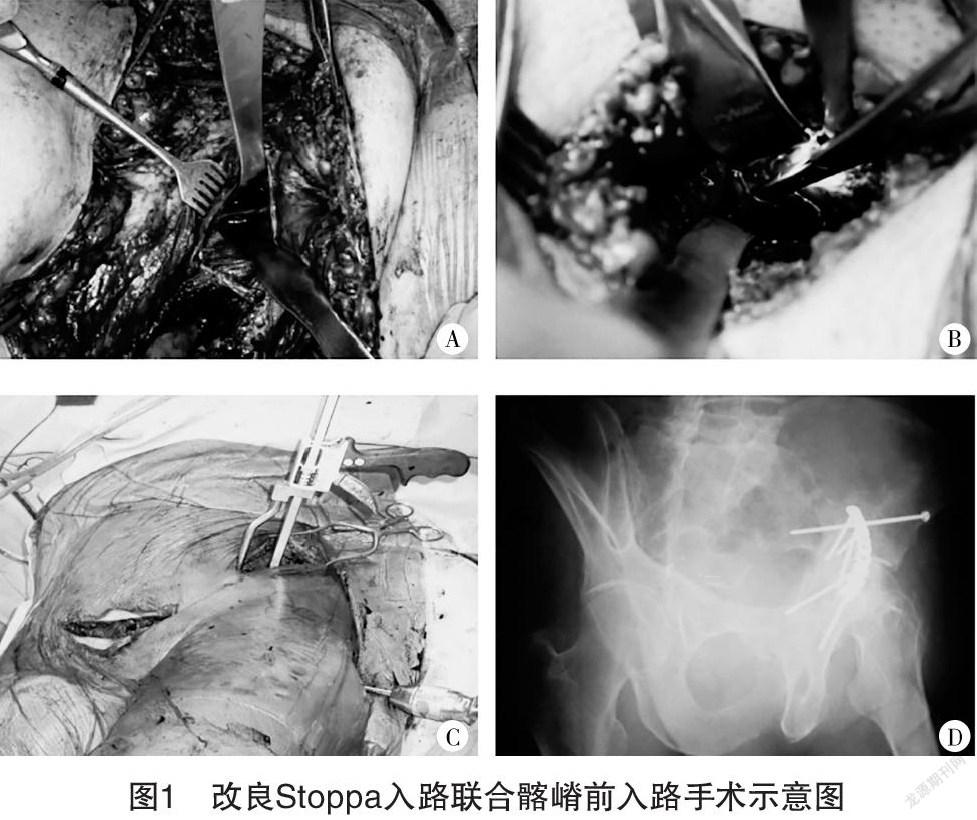
1.2 方法 对照组采取K-L入路,研究组采取改良Stoppa入路联合髂嵴前入路,两组均切开复位后行钢板内固定。对照组:气管插管全麻,患者取漂浮体位,视情况结合手术台调整为侧卧位、伸髋屈膝、髋关节轻度外展。K-L入路起自髂后上级前方,呈外凸的弧形延伸,沿臀大肌、臀中肌间隙,经大粗隆后缘,沿臀大肌纤维走形切开。术中牵引,充分暴露髋臼骨折面,去除碎骨渣,清理髋关节腔。在K-L入路中应重点保护坐骨神经。术中仔细辨认分离坐骨神经,将其从正常一侧牵向靠近骨折一侧。术中仔细辨认外旋肌和梨状肌,分离肌肉,在远离股骨止点处分开切断,将外旋肌和梨状肌挂线打结。分离髋臼上方的髂骨翼部分,在后上方和前上方分离臀中肌,打入钢针并钢板内固定。术野清创、灌洗,去除微小游离骨折碎片,以避免異位骨化的发生。研究组:先行髂嵴前入路,术者站于患侧,经过下列3个窗口复位髋臼骨折,第一窗口位于髂腰肌外侧,暴露髂窝内侧面和骶髂关节前面;第二窗口位于肌间隙内侧,在血管间隙外侧的股动静脉和淋巴管附近,分离髂耻筋膜,暴露骨盆缘和四方区(图1A);第三窗口位于股动静脉内侧,暴露耻骨上支和耻骨后间隙。改良Stoppa入路于腹直肌白线处垂直分离,术者站于患肢对侧,沿着耻骨支后间隙和四方区分离,血管夹结扎髂外动脉与闭孔动脉间动脉吻合支(图1B),将髂耻筋膜从骨盆缘分离出来,充分暴露骨盆环和髋臼。若骨折累及髂窝或延伸至髂嵴时,增加外侧窗固定髂窝骨折和髋臼前柱高位骨折(图1C)。完成复位后,沿着髂嵴或从髂前上棘至坐骨柱,使用钢板内固定(图1D)。
1.3 观察指标与判定标准 (1)术后3个月比较两组骨折复位情况。优良:骨折达到解剖复位,矫正骨折端各种移位,恢复正常的解剖关系,髋关节功能恢复正常。较好:骨折未达到解剖复位,但达到功能复位,髋关节功能恢复正常。尚可:骨折达到功能复位,髋关节功能恢复至正常的70%以上[8]。(2)比较术前与术后3、6、12个月,髋关节功能Harris评分与日常生活活动能力(activity of daily living,ADL)评分。Harris评分:①疼痛评分0~45分;②功能跛行评分0~11分,行走辅助评分0~11分,行走距离评分0~11分,上楼梯评分0~4分,穿袜子和鞋评分0~4分,坐椅子评分0~5分;③畸形:评分0~4分;④活动度评分0~5分[9]。总分范围0~100分。ADL评分:①大便评分0~10分;②小便评分0~10分;③修饰评分0~5分;④如厕评分0~10分;⑤吃饭评分0~10分;⑥转移评分0~15分;⑦活动评分0~15分;⑧穿衣评分0~10分;⑨上楼梯评分0~10分;⑩洗澡评分0~5分[10]。总分范围0~100分。(3)比较两组围术期指标。包括手术时间、手术出血量、术后住院时间。(4)比较两组术后并发症发生情况。包括股骨头坏死、深静脉血栓、异位骨化、坐骨神经损伤等。
1.4 统计学处理 采用SPSS 22.0软件对所得数据进行统计分析,计量资料用(x±s)表示,组间比较采用独立样本t检验,多个时间点比较采用重复测量方差分析,方差分析的两两比较采用SNK-q检验;计数资料以率(%)表示,比较采用字2检验;有序分类等级资料采用Mann-Whitney U检验。以P<0.05为差异有统计学意义。
2 结果
2.1 两组一般资料比较 两组一般资料比较,差异均无统计学意义(P>0.05),具有可比性,见表1。
2.2 两组骨折复位情况比较 研究组骨折复位情况优于对照组,差异有统计学意义(Z=12.092,P=0.002),见表2。
2.3 兩组髋关节功能比较 两组髋关节功能Harris评分存在组间与时间效应(F组间=14.936,P组间<0.001;F时间=382.735,P时间<0.001),且两组的手术方法与时间对髋关节功能Harris评分的影响存在交互作用(F交互=8.544,P交互<0.001)。术前,两组Harris评分比较,差异无统计学意义(P>0.05);术后3、6、12个月,研究组Harris评分均高于对照组(P<0.05)。与术前相比,两组术后3、6、12个月的Harris评分均上升(P<0.05)。见表3。
2.4 两组日常生活能力比较 两组ADL评分存在组间与时间效应(F组间=10.207,P组间<0.001;F时间=216.317,P时间<0.001),且两组的手术方法与时间对ADL评分存在交互作用(F交互=6.782,P交互<0.001)。术前,两组ADL评分比较,差异无统计学意义(P>0.05);术后3、6、12个月,研究组ADL评分均高于对照组(P<0.05)。与术前相比,两组术后3、6、12个月的ADL评分均上升(P<0.05)。见表4。
2.5 两组围术期指标比较 两组手术时间比较,差异无统计学意义(P>0.05);研究组手术出血量低于对照组,且术后住院时间短于对照组(P<0.05)。见表5。
2.6 两组术后并发症比较 两组术后均未发生股骨头坏死,无深静脉血栓形成,术后切口均一期愈合。研究组发生异位骨化4例,并发症发生率为9.52%(4/42)。对照组发生坐骨神经损伤2例、异位骨化4例,并发症发生率为15.00%(6/40)。两组术后并发症比较,差异无统计学意义(字2=0.574,P=0.449)。
3 讨论
盆骨髋臼骨折手术入路的选择通常基于骨折类型、手术医师经验以及对髋臼解剖结构的把握。为达到理想的解剖复位与功能复位,采取何种手术入路十分重要。文献[11]针对髋臼骨折手术入路的调查显示,56.5%的骨科医师倾向于改良Stoppa法,改良Stoppa术式已成为北美地区髋臼骨折的首选手术入路,近年来广受临床青睐。本研究分析两种临床主流的入路方式,比较K-L入路与改良Stoppa入路联合髂嵴前入路对术后髋关节功能及骨折复位情况,结果显示,改良Stoppa入路联合髂嵴前入路能获得更好的复位,骨折复位优良、较好、尚可的比例分别为45.24%、40.48%、14.29%,优良率高于K-L入路,这与文献[12-13]报道相符。并且改良Stoppa入路联合髂嵴前入路在术后3、6、12个月的Harris评分和ADL评分均大于K-L入路,说明改良Stoppa入路联合髂嵴前入路手术的术后髋关节功能和日常生活能力恢复更佳。国外一项采取改良Stoppa入路手术的研究表示,复杂髋臼骨折中双柱骨折占28%,后壁+后柱骨折、后壁+横断骨折占36%,其余为T形骨折、前柱+后半横断骨折等,解剖复位达到54%,功能复位达到43%,复位满意率为97%,患者健康相关生活质量明显提高[14]。
结合既往文献和本研究经验分析,改良Stoppa入路联合髂嵴前入路的优点包括以下几个方面:第一,可直视整个前柱,尤其是方形区,提供良好的手术视野,能够更好地显露骨盆髋臼解剖结构[15-16];第二,可以重建钢板周定并支撑方形区,该钢板可直接置于髋关节内侧,还可显露后柱并固定,固定稳固,尤其是涉及后柱的髋臼骨折复位效果好[17-18];第三,处理死亡之冠简单,避免大出血严重并发症[19-20]。本研究发现,尽管两种入路的手术时间大体相当,但改良Stoppa入路联合髂嵴前入路的手术出血量明显低于K-L入路,术后住院时间也较短。两种入路的术后并发症发生率分别为9.52%与15.00%,差异无统计学意义(P>0.05),但K-L入路有2例发生坐骨神经损伤。术后坐骨神经损伤为复杂盆骨髋臼骨折的常见并发症[21],为了预防坐骨神经损伤,结合临床经验,笔者建议:第一,应注意从股骨上剥离臀大肌肌腱,有助于充分暴露视野,避免术中过度牵拉坐骨神经导致神经损伤;第二,术中视情况调整为伸髋屈膝位可以放松坐骨神经;第三,少数患者可能存在坐骨神经被夹在骨折骨块之间,应十分仔细地鉴别并将坐骨神经从骨折块中挑出,避免误伤。
综上所述,相比传统K-L入路,改良Stoppa入路联合髂嵴前入路能够更好地显露骨盆髋臼解剖结构,有利于复杂盆骨髋臼骨折的复位与固定,骨折复位良好,术后髋关节功能和日常生活能力恢复更佳。
参考文献
[1] GIORDANO V,ACHARYA M R,PIRES R E,et al.Associated both-column acetabular fracture:An overview of operative steps and surgical technique[J].J Clin Orthop Trauma,2020,11(6):1031-1038.
[2] COSGROVE C T,BERKES M B,MCANDREW C M,et al.Kocher-langenbeck approach for posterior wall acetabular fractures[J].J Orthop Trauma,2020,34(2):21-22.
[3] SHAATH M K,LIM P K,ANDREWS R,et al.Clinical results of acetabular fracture fixation using a focal kocher-langenbeck approach without a specialty traction table[J].J Orthop Trauma,2020,34(6):316-320.
[4] GUO H Z,HE Y F,HE W Q.Modified stoppa approach for pelvic and acetabular fracture treatment[J].Acta Ortop Bras,2019,27(4):216-219.
[5] TANNAST M,KEEL M J B,SIEBENROCK K A,et al.Open reduction and internal fixation of acetabular fractures using the modified stoppa approach[J/OL].JBJS Essent Surg Tech,2019,9(1):e3.
[6]白求恩骨科加速康复联盟,白求恩公益基金会创伤骨科专业委员会,白求恩公益基金会关节外科专业委员会.加速康复外科学分会创伤骨科学组.加速康复外科理念下髋臼骨折诊疗规范的专家共识[J].中华创伤骨科志,2019,21(11):929-938.
[7] DYSKIN E,HILL B W,TORCHIA M T,et al.A survey of high-and low-energy acetabular fractures in elderly patients[J].Geriatr Orthop Surg Rehabil,2019,20(10):2151-2156.
[8] PANELLA A,SOLARINO G,VICENTI G,et al.Internal fixation of acetabular quadrilateral plate fractures in elderly patients:Could the fracture reduction quality affect their functional recovery[J].Aging Clin Exp Res,2020,9(3):502-508.
[9] LAU B C,SCRIBANI M,LASSITER T,et al.Correlation of single assessment numerical evaluation score for sport and activities of daily living to modified harris hip score and hip outcome score in patients undergoing arthroscopic hip surgery[J].Am J Sports Med,2019,47(11):2646-2650.
[10] KROM M A P,KALMET P H S,JAGTENBERG E M,et al.Medium-term patient-reported quality of life and activities of daily living in surgically treated trauma patients with pelvic,acetabular or combined pelvic and acetabular fractures in a retrospective single-center study[J].J Orthop Trauma,2021,35(4):192-197.
[11] MOED B R,ISRAEL H A.Which anterior acetabular fracture surgical approach is preferred?a survey of the orthopaedic trauma association active membership[J].J Orthop Trauma,2020,34(4):216-220.
[12]邓志刚,李凯.改良Stoppa入路联合髂嵴前入路与K-L入路治疗复杂髋臼骨折合并骨盆骨折的疗效比较[J].现代诊断与治疗,2017,28(2):290-291.
[13]田思宇,王忠正,赵阔,等.改良Stoppa入路与髂腹股沟入路钢板内固定治疗髋臼前柱/前壁骨折的疗效比较[J].中华创伤杂志,2020,36(11):977-982.
[14] VERBEEK D O,PONSEN K J,HEIJL M,et al.Modified Stoppa approach for operative treatment of acetabular fractures:10-year experience and mid-term follow-up[J].Injury,2018,49(6):1137-1140.
[15] CHEN Z,YANG H,WU Z,et al.A combination of the modified Stoppa approach and the iliac fossa approach in treating compound acetabular fractures by using an anterior ilioischial plate[J].Acta Orthop Belg,2019,85(2):182-191.
[16] NAYAK T,MITTAL S,TRIKHA V,et al.Short-term results of surgical treatment of acetabular fractures using the modified Stoppa approach[J].J Clin Orthop Trauma,2020,11(6):1121-1127.
[17]薛飞,贾文超,武剑,等.改良Stoppa入路内髂坐钢板固定治疗涉及后柱的髋臼骨折[J].中华创伤骨科杂志,2019,21(6):478-483.
[18] WU H,ZHANG L,GUO X,et al.Meta-analysis of modified Stoppa approach and ilioinguinal approach in anterior pelvic ring and acetabular fractures[J].Medicine,2020,99(4):1839-1845.
[19] AÇAN A E,KILINC C Y,GÜLTAÇ E,et al.Effects of different anesthesia techniques on intraoperative blood loss in acetabular fractures undergoing the Modified Stoppa approach[J].Ulus Travma Acil Cerrahi Derg,2020,26(3):445-452.
[20]付忠泉,陳健荣,禤天航,等.改良Stoppa入路在髋臼及骨盆骨折手术治疗中的应用[J].实用医院临床杂志,2019,16(5):129-131.
[21]吕刚,王利昕,马钰,等.Kocher-Langenbeck入路结合拉力螺钉技术治疗髋臼横断和后壁骨折T形骨折[J].中华骨科杂志,2019,39(13):803-809.
(收稿日期:2021-5-18) (本文编辑:田婧)
猜你喜欢
中华骨与关节外科杂志(2022年1期)2022-08-31 09:18:48
西安交通大学学报(医学版)(2022年1期)2022-01-13 08:13:08
浙江临床医学(2021年8期)2021-10-14 02:04:44
中国医疗器械信息(2019年19期)2019-10-19 08:24:46
骨科临床与研究杂志(2019年2期)2019-03-07 07:12:12
分子影像学杂志(2018年1期)2018-02-05 05:43:21
中华骨与关节外科杂志(2016年6期)2016-05-17 06:11:09
中华骨与关节外科杂志(2016年5期)2016-05-17 06:11:01
中华骨与关节外科杂志(2016年5期)2016-05-17 06:10:53
中国卫生标准管理(2016年36期)2016-03-28 12:52:33