
Low-dose intralesional injection of 5-fluorouracil and triamcinolone reduces tissue resident memory T cells in chronic eczema
2022-02-11 05:28:56YunWuGuoJiangWangHuiQiongHeHaiHongQinWenTongShenYueYuXunZhangMaoLinZhouJianBiaoFei
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Chronic eczema is a chronic inflammatory skin condition, characterized by longcourse, recurrent itchy papules, and plaques with lichenification and hyperpigmentation[1-3]. Repeated scratching and irritation is the main cause of repeated delay and refractory eczema. In China, 7.5 out of every 100 people suffer from eczema[4]. Recently, tissue resident memory T (T) cells have been suggested to play a pivotal role in the pathogenesis of chronic eczema, in addition to Th2-dominant inflammation[5]. It is reported that after 16 wk of treatment with topical corticosteroids (TCS), Tcells were still present in the tissue[6]. Further studies have confirmed that the skin lesions of dermatitis and eczema patients are dominated by CD8Tcells, and these Tcells can persist for months and induce recurrent eczema[7,8].
TCS and topical calcineurin inhibitors (TCIs) are the most commonly used topical drugs for eczema treatment, and they can alleviate the localized inflammation[9]. However, some patients still suffer from repeated attacks. Oral corticosteroids and immunosuppressants have been widely used for the treatment of severe eczema. However, their long-term use can cause severe side effects, such as high blood pressure, blood glucose level, electrolyte disorders, decreased immune function, and pathogen infection. So far, Dupilumab has been approved for the treatment of moderate to severe eczema. In a phase 3 clinical trial, more than 65% of patients treated with dupilumab in combination with topical steroids achieved 75% improvement in eczema area severity index from baseline[10]. Other potential treatments for eczema such as mepolizumab and omalizumab are still under evaluation. A recent multicenter, randomized, double-blind, placebo-controlled, phase 2 clinical trial showed that 100 mg mepolizumab administered subcutaneously did not show any clinical improvement in patients with moderate to severe atopic eczema[11]. Omalizumab is a safe and relatively well-tolerated with some clinical benefits in atopic dermatitis patients[12], though its efficacy in adults is still under debate[13]. Moreover, these treatment modalities are expensive and require long-term use, which limits their clinical application.
Local intralesional glucocorticoid injection therapy has been used for decades in the treatment of localized dermatitis. Studies have shown that local injection of no more than 20 mg triamcinolone acetonide (TA) is safe and cost-effective for the treatment of localized dermatitis and other inflammatory skin diseases[14]. 5-Fluorouracil (5-FU), another common drug for intralesional injection, has been used for treating inflammatory hypertrophy in the skin as in scarring[15,16]. Our previous study has demonstrated that compared to the TA group, intralesional injection of 5-FU+TA can effectively reduce local inflammation and significantly reduce the recurrence of eczema in a mouse model[17]. However, there have been no clinical studies investigating the effect of 5-FU+TA for chronic eczemaintralesional injection, let alone with large samples and long-term follow-up.
Efficacy score = (score before treatment - score after treatment)/ score before treatment × 100%
The aim of this double-blind randomized controlled prospective clinical study was to further evaluate the efficacy and safety of intralesional injection of 5-FU and TA for the treatment of localized rash and management of relapse in chronic eczema patients and to explore the potential underlying mechanism.
MATERIALS AND METHODS
Study design
Effectiveness percentage = (number of cured patients + number of patients with excellent response)/ total number of patients × 100%
Patients
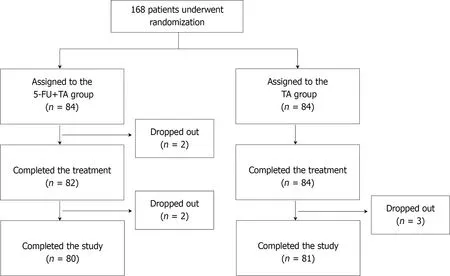
One hundred sixty-eight patients who visited our hospital from January 2018 to June 2019 and were diagnosed with chronic eczema with localized lesions were recruited for the study. All patients provided signed written consent. Using a random sequence generated by a computer program, patients were randomly assigned to two groups: a 5-FU+TA group (= 84) and a TA (= 84) group (Figure 1). Four patients from the 5-FU+TA group and three patients from the TA group discontinued the study for personal reasons.
Treatment protocol and follow-up
A one-time injection was performed for both groups. For the 5-FU+TA group, 2 mL normal saline (Shanghai Xudong Haipu Pharmaceutical Co., Ltd.) was mixed well with 1 mL 5-FU solution (Shanghai Xudong Haipu Pharmaceutical Co., Ltd.) (containing 25 mg 5-FU) and 1 mL TA solution (Shanghai General Medicine Industry Co., Ltd.) (containing 10 mg TA). Infiltration and injection were performed to allow 1 mL of the mixture into every 4 cmof the skin lesion area. The total injection area should be less than 32 cmand protected from contact with water for 3 days after injection to prevent secondary bacterial infection at the injection site. For the TA group, 3 mL of normal saline was mixed with 1 mL of TA solution (containing 10 mg TA). The injection method, total injection area, and course of treatment were the same as those for the 5-FU+TA treatment group.
Follow-up was conducted 2 wk after treatment and monthly thereafter for up to 12 mo. Effectiveness was evaluated, and adverse events were recorded and photographed.
Clinical data analysis
Before treatment and 2 wk after treatment, two dermatologists graded the skin lesions of each patient independently. The evaluation of clinical efficacy referred to the atopic dermatitis severity index (ADSI) scoring system[18]. Because chronic eczema has no exudation, the remaining four indicators including pruritus, erythema, excoriation, and lichenification were graded on a 4-point scale (range 0-3): none = 0 point; mild = 1 point; moderate = 2 points; and severe = 3 points. The total score for these 4 items was ≤ 12 points. An efficacy score was calculated as:
I have much on my conscience; it is high time for me to become white paper! And so he did! he became white paper, the very paper on which this story is printed
The efficacy criteria were: cure, score > 90%; excellent response, score 61%-90%; good response, score 20%-60%; and poor or nonresponse, score < 20%.
He was forced to place himself between the two eldest, they helped him to wine, gave him the best pieces of meat, and thought that in all the world they had never seen a handsomer man
This was a double-blind randomized controlled prospective study. The patients and the two dermatologists were both blinded to the group assignment. The diagnosis of chronic localized eczema was established based on the 2011 Guidelines for Eczema Diagnosis and Treatment designated by the Immunology Group, Dermatovenereology Society, Chinese Medical Association[4]. The inclusion criteria were: Age from 28-80 years and a history of chronic localized eczema lasting for > 6 mo. The exclusion criteria were: i) nullipara, pregnant, planning a pregnancy or lactating; ii) known allergies to FU or glucocorticoid; iii) treatment with any systemic corticosteroids/ antibiotics/ immunosuppressants in the previous 6 wk or use of topical dermocorticoids/ antibiotics/ antihistamines or calcineurin-inhibiting type immunosuppressants in the previous 2 wk; and iv) renal failure, liver dysfunction, hematological disease, immune deficiency, systemic or local infection (including chronic obstructive pulmonary disease patients). The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Shanghai University of Medicine and Health Science Affiliated Zhoupu Hospital’s Research Ethics Committee (No. 2018-C-014-M01). This study has been registered at http://www.chictr.org.cn/ (No. ChiCTR2100043660).
The patients were followed up for 1 year, and the number of patients who relapsed was recorded.
Relapse rate = number of patients with eczema relapse/ total number of effective patients (cured patients + patients with excellent response) × 100%
Evaluation of adverse events
Routine blood tests and liver and kidney function tests were performed before and 2 wk after treatment. We also monitored and recorded the events of local infection, skin atrophy, pigmentation,after treatment and during the 1-year follow-up.
Histopathological examination and immunohistochemical staining
To investigate the histopathological changes and the infiltration of Tcells and other immune cells after treatment of chronic localized eczema, we collected biopsy specimens at the lesion site from 15 patients in each group before and 2 wk after treatment.
Jack Zipes also points out that the story of the oven as a means of execution in a German tale has been particularly disturbing for adults since the Holocaust119 (Zipes 1997). In 2003, author Louise Murphy wrote, The True Story of Hansel and Gretel, a book set during WWII and the Holocaust using elements from Hansel and Gretel.
6. Fairy godmother: This fairy godmother dispenses64 advice instead of gifts to Donkeyskin, unlike her counterpart in Cinderella.Return to place in story.
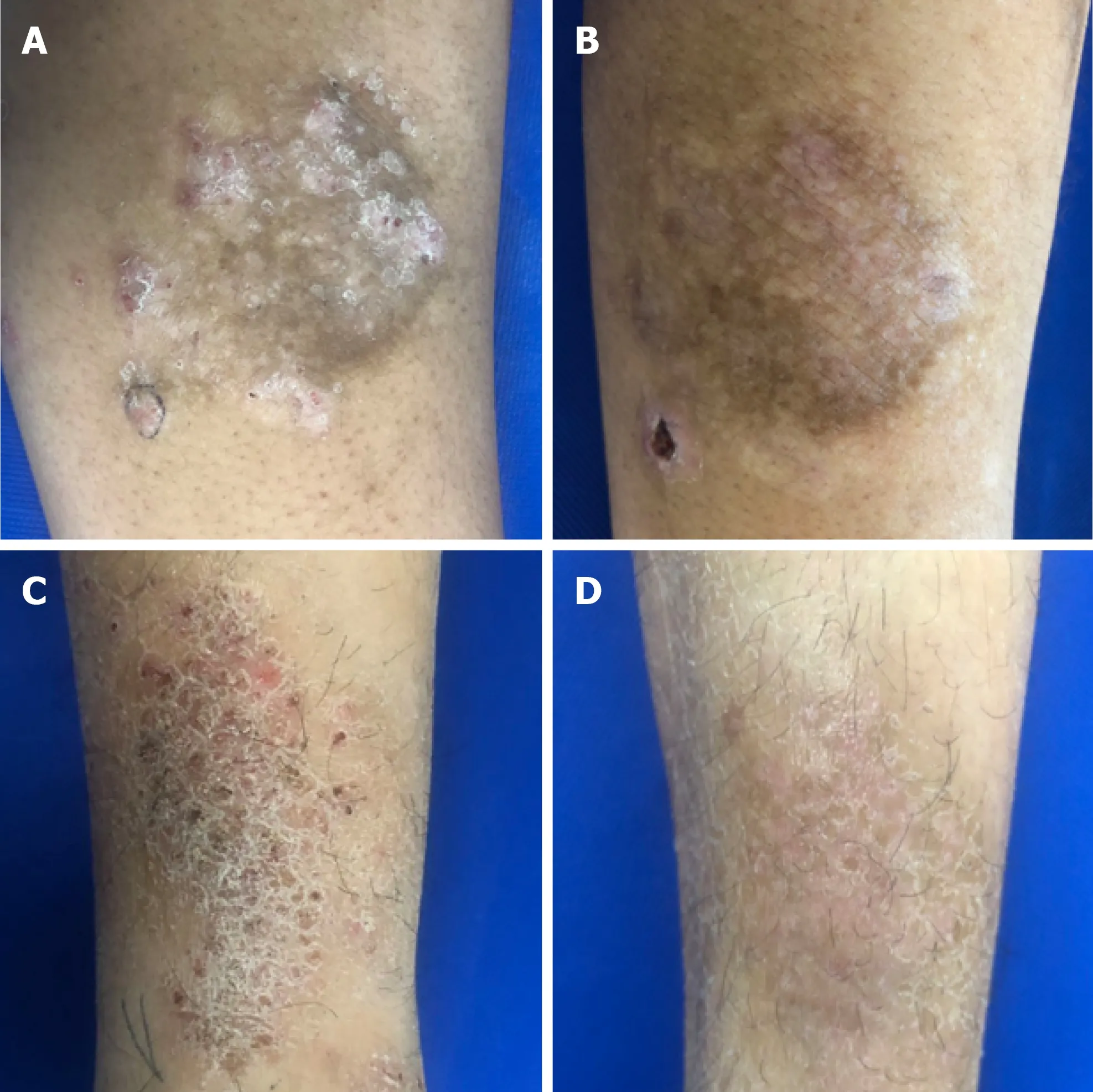
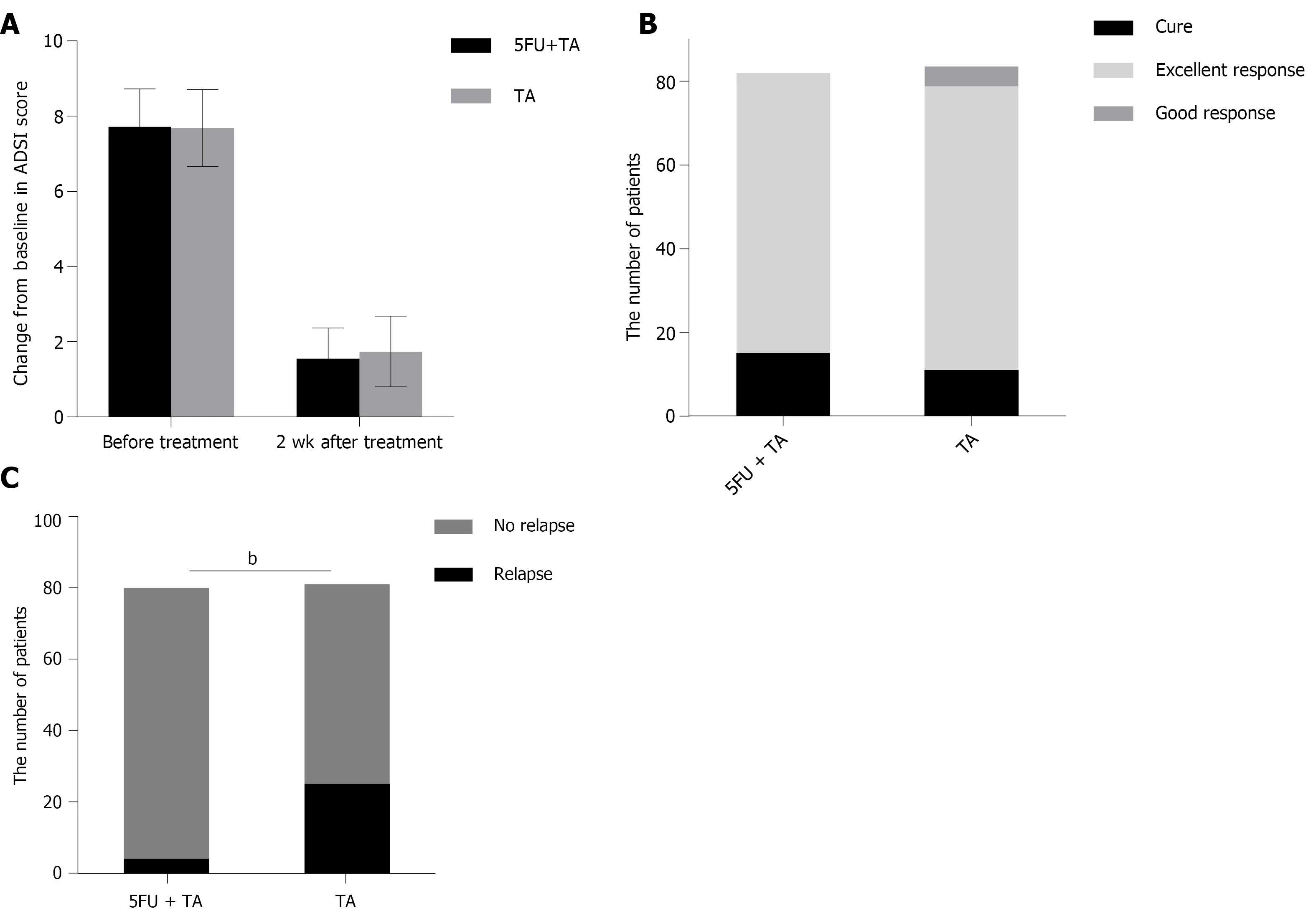
The mean ADSI scores of patients who complete the treatment and evaluation of clinical efficacy before treatment were 7.89 ± 0.89 in the 5-FU+TA group and 7.68 ± 1.02 in the TA group (= 0.154). Two weeks after treatment, pruritus was alleviated significantly according to the patients, and the color of erythema became lighter in both groups. A small amount of scales was found in 23 out of 84 patients (27.38%) in the TA group (Figure 2). The mean ADSI scores at 2 wk after treatment for the 5-FU+TA group and TA group were 1.55 ± 0.82 and 1.74 ± 0.94, respectively. The ADSI scores for both groups were significantly lower than those before treatment for the same group (< 0.001 for both), and there was no significant difference between the two groups (= -1.383,= 0.168; Figure 3A). The 5-FU+TA group had a cure rate of 18.29% (= 15) and an excellent response rate of 81.70% (= 67), and no cases showed a good response or nonresponse. The TA group had a cure rate of 13.10% (= 11), an excellent response rate of 80.95% (= 68), a good response rate of 5.95% (= 5), and no cases of nonresponse. There was no significant difference in the percentage of effectiveness between the two groups (= 3.201,= 0.074; Figure 3B). Interestingly, at the 1-year follow-up, relapse had occurred in 4 patients (5.00%) in the 5-FU+TA group and 25 patients (30.86%) in the TA group (= 18.232,< 0.01, Figure 3C).
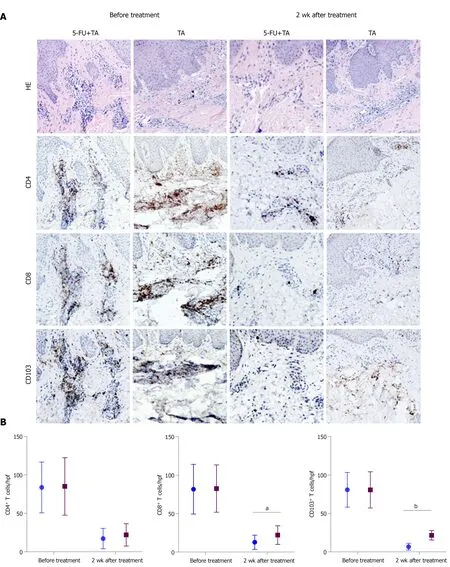
For immunohistochemical staining, the lesional tissue sections were washed in phosphate-buffered saline and then boiled in EDTA for antigen retrieval, followed by 3% hydrogen peroxide incubation and 5% bovine serum albumin blockade. Tissue sections were incubated with primary antibodies against CD4 (1:100, Shanghai Jiehao Biotechnology Co., Ltd., Shanghai, China), CD8 (1:100, Shanghai Jiehao Biotechnology Co., Ltd.,), and CD103 (1:150, Abcam, Cambridge, UK). After incubation with a secondary antibody, staining results were observed under a microscope (Olympus, Tokyo, Japan). The images were recorded for further analysis. Cell counts were performed blindly on randomly selected histological images at ×100 magnification (High power field).
Statistical analyses
The data were analyzed using PASW software, version 22 (IBM Corporation, Armonk, NY). The graphs were plotted using GraphPad Prism, version 8.00 (GraphPad Software, Inc., San Diego, CA). Disease duration was compared between groups using the Mann-Whitney U test. Independent t-tests were used to compare the patients’ ages, ADSI scores, and T-cell counts. The chi-squared test and Fisher’s exact were used to determine statistical differences between the groups in relation to sex, the anatomical site treated, the effective rate of treatment, and the recurrence rate. A twotailedvalue < 0.05 was considered statistically significant. Unless otherwise specified, data are presented as mean ± SD.
Back in England, Carlton Jackson relates, some Eighth Army veterans were belting out “Lili Marleen” one night in a pub frequested by song publisher J. J. Phillips. He remarked that village police might think they were German spies. “If you re so fired up about it,” a soldier yelled, “why don t you write us some English words?”
RESULTS
Patient characteristics
But as I began driving home my conscience started talking to me. It was telling me that I knew exactly who I needed to say I love you to. You see, five years ago, my father and I had a vicious2 disagreement and really never resolved it since that time. We avoided seeing each other unless we absolutely had to at Christmas or other family gatherings3.
Clinical outcomes
For staining of lesional tissue with hematoxylin and eosin (HE), fixed tissues were embedded in paraffin and cut into 5 μm thin sections, followed by staining with HE.
Adverse events
Six patients in the 5-FU+TA group and five patients in the TA group had local pruritus after injection, which resolved without further treatment. During the follow-up, local pigmentation was observed in both groups, and it gradually improved over time. No obvious skin atrophy, redness, swelling, heat, pain, or other symptoms of infection were noted in either group. There were no adverse reactions such as leukopenia, anemia, and thrombocytopenia in either group during the 1-year follow-up.
Six years after high school graduation, Marc called and asked if he could move home for a couple of months. He had spent those years well, graduating Phi Beta Kappa magna cum laude from college, completing two congressional internships in Washington, D.C., winning the Jesse Marvin Unruh Fellowship4 to the California State Legislature, and finally, becoming a legislative5 assistant in Sacramento. Other than short vacation visits, however, he had lived away from home. With his younger sister leaving for college, I was especially thrilled to have Marc coming home.
Intralesional injection of 5-FU+TA reduced local retention of CD103+ memory T cells
To explore the mechanism by which 5-FU and TA reduced the relapse rate of chronic eczema, we investigated differences in T-cell infiltration in the local skin lesions of patients from both groups before treatment and 2 wk after treatment by HE and immunohistochemical staining. The results showed that the lesional skin was infiltrated with lymphocytes and other inflammatory cells in the epidermis before treatment. A number of CD4, CD8, and CD103T-cell infiltration was observed in both groups with no significant differences (= 0.914, 0.945, 0.988, respectively; Figure 4A). Two weeks after treatment, the CD4, CD8, and CD103T cell counts for the two groups were significantly less than before treatment (all< 0.001,= 15 for each group). Although no significant difference was observed in the number of CD4T cells between the two groups (= 0.355) at 2 wk after treatment, the numbers of CD8and CD103T cells in the skin lesions were significantly less in the 5-FU+TA group than in the TA group (= 0.025,< 0.001; Figure 4B). In some skin lesions from the 5-FU+TA group, no inflammatory cell infiltration was observed.
DISCUSSION
Chronic eczema recurs frequently, and its treatment has always been challenging. Once the skin lesions become hypertrophic, the penetration of conventional topical drugs such as TCIs is decreased. Although intralesional corticosteroid has been proven effective for localized dermatitis, long-term or high-dose application of TCI treatment may cause skin atrophy, telangiectasia, increased vellus hair, systemic absorption, prickling, and burning sensations[3,19]. Intralesional 5-FU has been also used for treating localized inflammatory infection. The current study included 168 patients and showed that the combination therapy of 5-FU and TA was effective and safe for the treatment of chronic eczema. To the best of our knowledge, this prospective study is
the first to observe the effect of 5-FU+TA on chronic eczema through intralesional injection.
Tcells are involved in the relapse of chronic eczema. Tcells are distributed in the epidermis and dermis of the skin, and they constantly move around in the local area to quickly recognize a pathogen or an antigen that invades again, and this activity plays an important protective role on the entire skin system. In addition, Tcells release IL-2, tumor necrosis factor-α, interferon-γ (IFN-γ), and other cytokines to further boost the immune response[25-27]. Results from our histopathological and immunohistochemical examinations suggest that the skin lesions from the 5-FU+TA group had significantly fewer CD103Tcells and CD8cells than did those from the TA group at 2 wk after treatment, suggesting that 5-FU may reduce the recurrence of chronic localized eczema by minimizing the number of Tcells in the lesion. Recent studies have shown that allergens can induce the production of CD8Tcells through IL-17A and IFN-γ[28]. The exact mechanisms by which 5-FU reduces the retention of Tcells require further investigation.
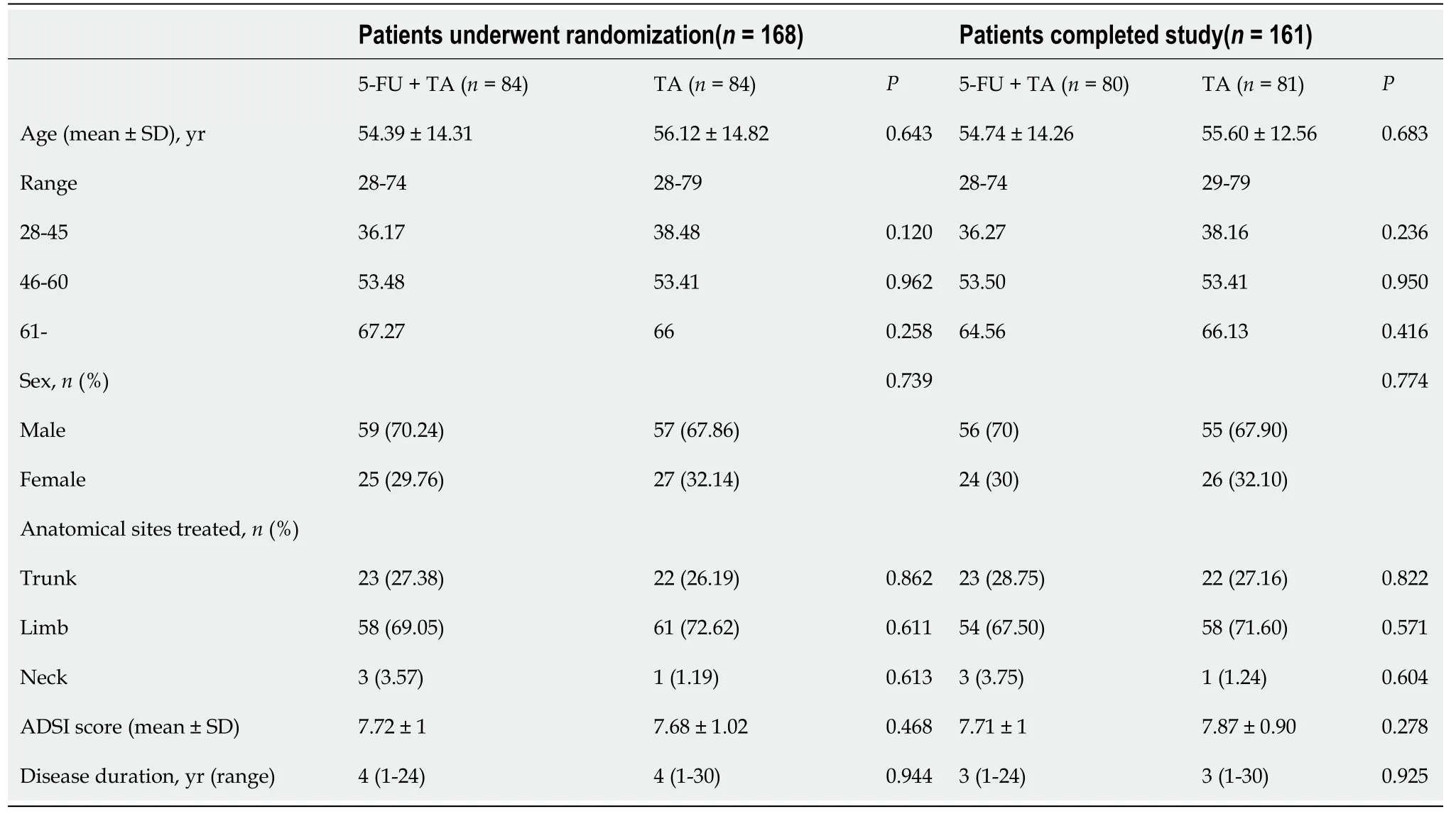
The baseline demographic and clinical characteristics of patients in the two groups are summarized in Table 1. The age, sex, number of anatomical sites treated, and disease duration did not differ significantly between the groups (> 0.05 for all).
The aggravating factors for adult eczema include environmental factors, sweating, physical irritation (including scratching), microbes, stress, and food[21]. Our study was a double-blind randomized controlled prospective study, and all participants were outpatients from our hospital with similar living environments and eating habits. We did not find statistically significant differences in age, sex, anatomical sites treated, or the treatment period among the groups.
When they had got out a little way the man said, Are my eyes green? No, said his wife; why should they be? They rowed a little further out, and he asked again, Are my eyes not green yet? What nonsense is this? said she; why should they be green? Oh, my dear, said he, can t you just say that they are green? Very well, said she, they are green
There is a common concern of the potential adverse reaction of intralesional TA and 5-FU, such as infertility, skin atrophy, and telangiectasia. For the treatment of keloid scars, it is suggested that 5-FU (maximum 90 mg each injection) + TA treatment resulted in a lower incidence of skin atrophy and telangiectasia than treatment with TA alone (10-40 mg TA single injection)[22,23]. The common dosage range of 5-FU is 45-50 mg/mL, and each injection volume is less than 2 mL, with more than 3 sessions[24]. In this study, 25 mg 5-FU and 10 mg TA were used intralesionally once for the treatment. Compared with the dosage for keloid treatment, our dosage of 5-FU and TA is relatively low. Laboratory tests after 2 wk of treatment showed no abnormal results for blood and liver and renal function. Similarly, no such adverse events were observed during the 1-year follow-up. Moreover, the dosage of TA is half of the maximum safe dose reported in a previous study (20 mg) for the treatment of localized dermatitis[14]. No adverse reactions such as skin atrophy or telangiectasia were observed in this study, suggesting that the combination of 5-FU and TA at these dosages was safe for chronic eczema treatment. 5-FU and TA both have an immune suppressive effect, which requires attention regarding the chance of local infection. Patients were informed about the risk of bacterial contamination. No local infection was observed in either group during the follow-up. In clinical practice, topical antibiotics such as Mupirocin could be prescribed for infection prevention.
To the best of our knowledge, there has been no study investigating the effectiveness of corticosteroids for eczema treatment through intralesional injection. A previous study investigated the use of 0.05% fluticasone propionate cream or 0.005% fluticasone propionate ointment given once or twice daily to eczema patients for 1 mo and continued twice weekly thereafter. In that study, the relapse rate at the 16 wk follow-up was 19% for the 0.05% fluticasone propionate cream group and 40% for the 0.005% fluticasone propionate ointment group. For the placebo group, the average relapse time was 6 wk, and the relapse rate was 64%[20]. In the present double-blind randomized study, local injection using 5-FU+TA or TA only was applied, and the patients were followed up for up to 1 year. Our data demonstrate that a one-time intralesional injection of TA in combination with 5-FU could successfully treat the localized rash of chronic eczema. Most importantly, the relapse rate in the 5-FU+TA group was significantly lower than that in the TA group (4.9%31.64%), and also much lower than the rate in the previously mentioned study, demonstrating that 5-FU+TA treatmentintralesional injection can significantly reduce the recurrence of eczema.
This study is not without limitations. Occupation may be a cofounding factor that we should have considered. A longer follow-up is warranted for monitoring the relapse rate and confirming the efficacy and safety of 5-FU+TA treatment. Finally, we would like to collect more samples to explore the potential mechanisms, possibly by measuring the cytokines secreted from the lesional site, in our future studies.
The prince did all as he was told, then they took flight; they crossed the seven seas, and at each one the prince fed the Simurgh When they alighted on the shore of the last sea, it said: O my son! there lies your road; follow it to the city
CONCLUSION
In summary, our study demonstrated that intralesional injection of 5-FU+TA can effectively and safely treat the localized rash of chronic eczema and significantly reduced the retention of Tcells in the skin lesion. This combination may provide a new treatment option for chronic eczema patients with epidermis hypertrophy and localized rash.
ARTICLE HIGHLIGHTS
Research background
Chronic eczema is an itchy, inflamed skin condition that tends to flare periodically.The latest findings suggest that tissue resident memory T (TRM) cells may play an important role in the pathogenesis of chronic eczema.
Research motivation
Intralesional injection of 5-fluorouracil (5-FU) and triamcinolone (TA) can effectively reduce local inflammation and significantly reduce the recurrence of eczema in a mouse model. There have been no clinical studies investigating the effect of 5-FU+TA for chronic eczema via intralesional injection.
Research objectives
To evaluate the efficacy and safety of intralesional injection of 5-FU and TA for the treatment of localized rash and management of relapse in chronic eczema patients and explore the potential underlying mechanism.
Research methods
In this double-blind randomized controlled prospective study, we used the ADSI score to evaluate the efficacy of treatment and the effect on recurrence, and histopathological changes before and after treatment also were assessed.
Research results
The mean ADSI score and effective rates were comparable between the two groups,while the relapse rate was significantly lower in the 5-FU+TA group than in the TA group. Histological examination showed significantly fewer CD8and CD103T cells but not CD4T cells in the 5-FU+TA group.
Research conclusions
5 -FU+TA can effectively and safely treat the localized rash of chronic eczema and significantly reduce the retention of Tcells in the skin lesion.
Research perspectives
Low-dose intralesional injection of 5-FU+TA may be a new treatment option for chronic eczema patients with epidermis hypertrophy and localized rash.
 World Journal of Clinical Cases2022年1期
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Omicron variant (B.1.1.529) of SARS-CoV-2: Mutation, infectivity,transmission, and vaccine resistance
- Clinical manifestations and prenatal diagnosis of Ullrich congenital muscular dystrophy: A case report
- Lunate dislocation with avulsed triquetral fracture: A case report
- Protein-losing enteropathy caused by a jejunal ulcer after an internal hernia in Petersen's space: A case report
- Eustachian tube teratoma: A case report
- Cerebral venous sinus thrombosis in pregnancy: A case report