
Lunate dislocation with avulsed triquetral fracture: A case report
2022-02-11 05:29LingYiLiChengJyhLinChihYuanKo
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Lunate dislocations with associated avulsed triquetral bone fracture caused by high energy trauma ae rarely reported. According to literature reviews, 7% of all carpus injuries involve the lunate, of which only 3% are classified as volar lunate dislocations[1,2]. Owing to their rarity, they are often misdiagnosed and may be missed in 25% of cases[3]. The initial presentation is often atypical. To date, there is no consensus regarding the optimal treatment of lunate dislocation. Currently, most authors consider urgent open reduction for the dislocation, repair or reconstruction of the surrounding carpal ligaments and capsules, and fixation with Kirschner wires or screws. We found these surgical options to be frequently associated with complications and unsatisfactory results. Herein, we report a rare case of acute lunate dislocation with triquetral fracture treated by closed reduction with Kirschner wires. The radiological results were encouraging and the patient demonstrated satisfactory function of the wrist joint.
This manuscript follows the CARE guidelines, and written informed consent was obtained from the patient for publication of this manuscript and the accompanying images.
CASE PRESENTATION
Chief complaints
A 37-year-old man presented to the Emergency Department of our hospital with closed injury to the right side of the face and right wrist, and hyper-extension of the wrist. Initially, the patient complained of headache, dizziness, and moderate pain in the right wrist.
The next day, a motor accident spread all over the barrio(). The motorbike hit the wall leaving the guy dead and amazingly the girl survived! The guy knew that the breaks aren t working. He kept it to his self and made the girl wear the helmet so that somehow she won t get hurt.
History of present illness
The patient symptoms started after a fall from his motor vehicle an hour prior to presentation at the hospital.
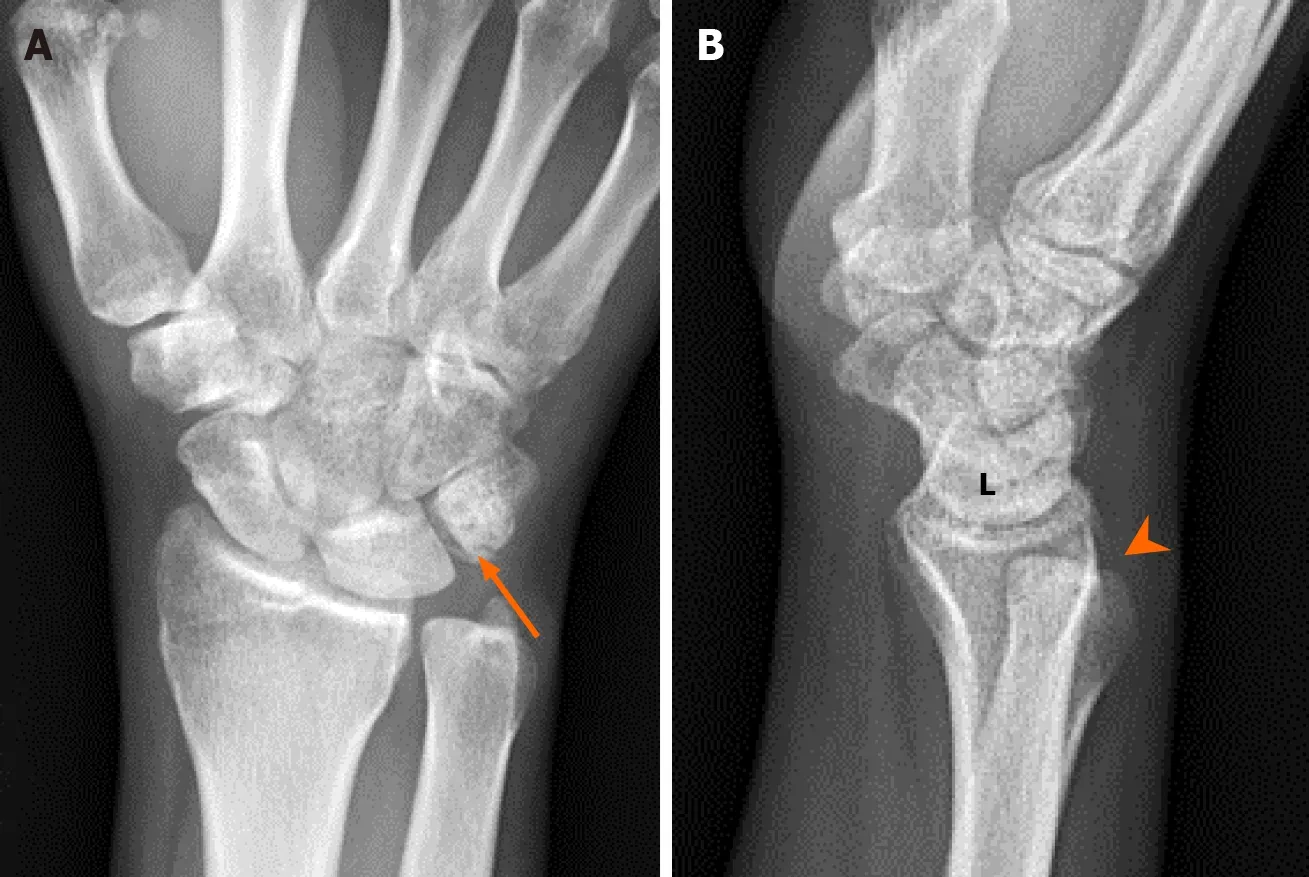
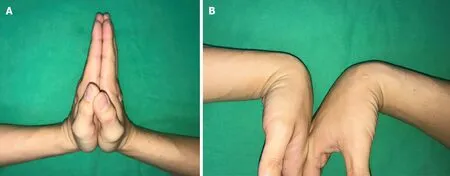
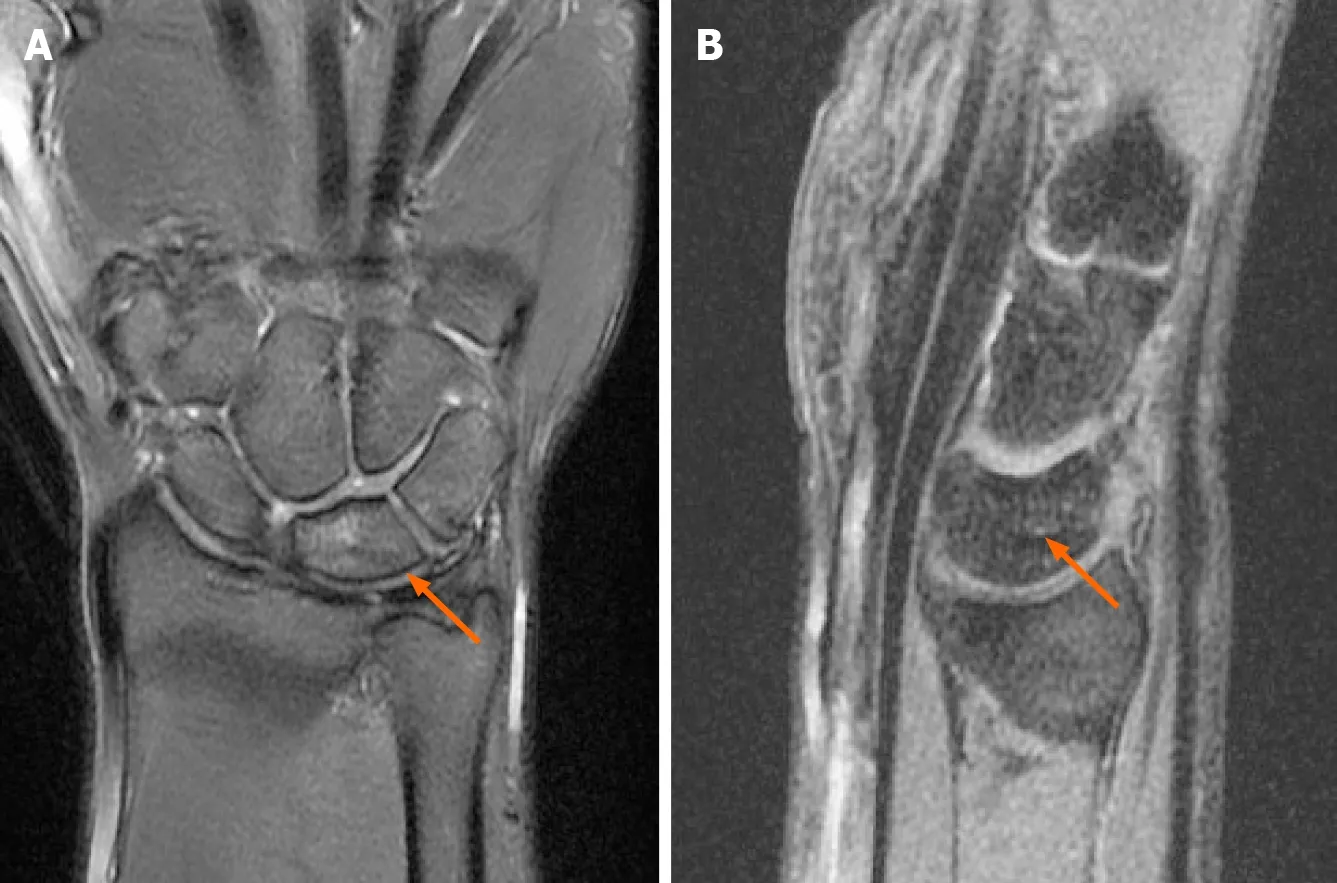
Magnetic resonance imaging (MRI) performed 2 mo postoperatively revealed residual bone marrow edema in the lunate, triquetrum, and scaphoid (Figure 3). Complete bony healing of the triquetrum was confirmed by radiographic examination 20 wk after the trauma (Figure 4). The patient resumed daily activities 24 wk after the trauma. The range of motion of the right wrist was satisfactory with an extension /flexion range of 90°-0°-75°, and pronation/supination range of 90°-0°-90° (Figure 5). The patient experienced no pain at rest, and only reported mild pain related to activity. The movement of the fingers, peripheral sensibility and circulation were fair. There was no avascular necrosis of the lunate, scapholunate instability, or carpal joint arthritis during the one-year follow-up (Figure 6). Furthermore, the patient was underwent a follow-up MRI about 18 mo postoperatively. The lunate edema was almost completely resorbed and the lunate bone had no features of progressing into osteonecrosis (Figure 7).
History of past illness
The patient had no relevant past medical history.
Personal and family history
The little soldier inquired the meaning of all this noise, and was told that the Princess Ludovine, the King s beautiful daughter, had been found, and was about to make her triumphal entry
Physical examination
The patient was finally diagnosed with acute lunate volar dislocation with avulsed triquetral fracture. This fracture pattern could be classified as Mayfield classification stage IV[5].
Laboratory examinations
All the blood tests were within normal values.
Imaging examinations
An emergency physician made the initial diagnosis of fracture of the right mandibular body and contusion of the right wrist at the first survey after radiologic evaluations.
MULTIDISCIPLINARY EXPERT CONSULTATION
This year my youngest son will be a senior in high school. He, too, has now announced that he is too old for notes. But like his older brother and sister before him, he will receive those notes till the day he graduates-and in whatever lunches I pack for him afterwards.
FINAL DIAGNOSIS
The chin was obviously swollen and deformed, and the right wrist appeared slightly swollen; however, distal pulsation, thumb/finger motion, finger sensation remained normal.
TREATMENT
An attempt at closed reduction in the emergency room failed due to excessive swelling of the wrist and inability of the patient to cooperate with the reduction maneuver due to pain. The patient was then scheduled for open reduction and surrounding carpal ligaments repair.
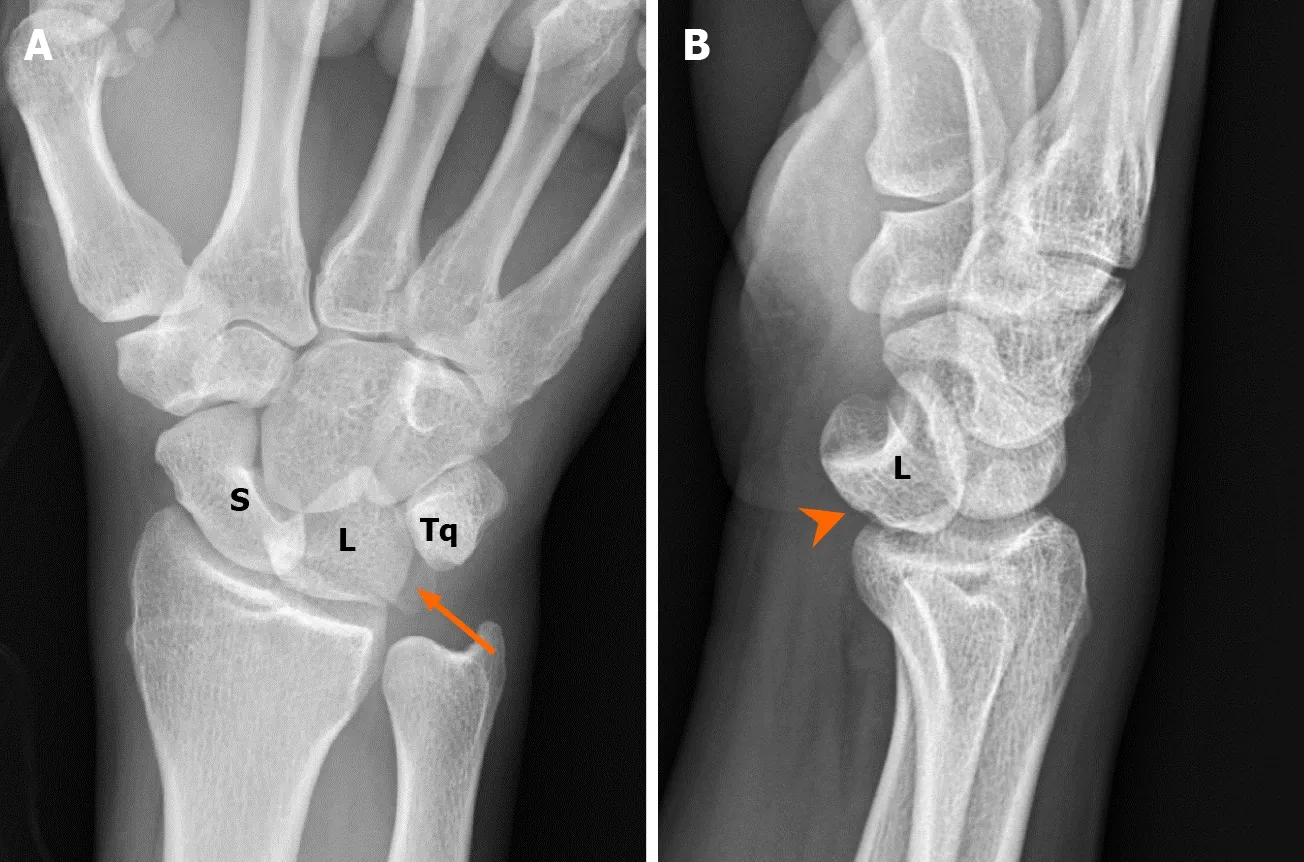
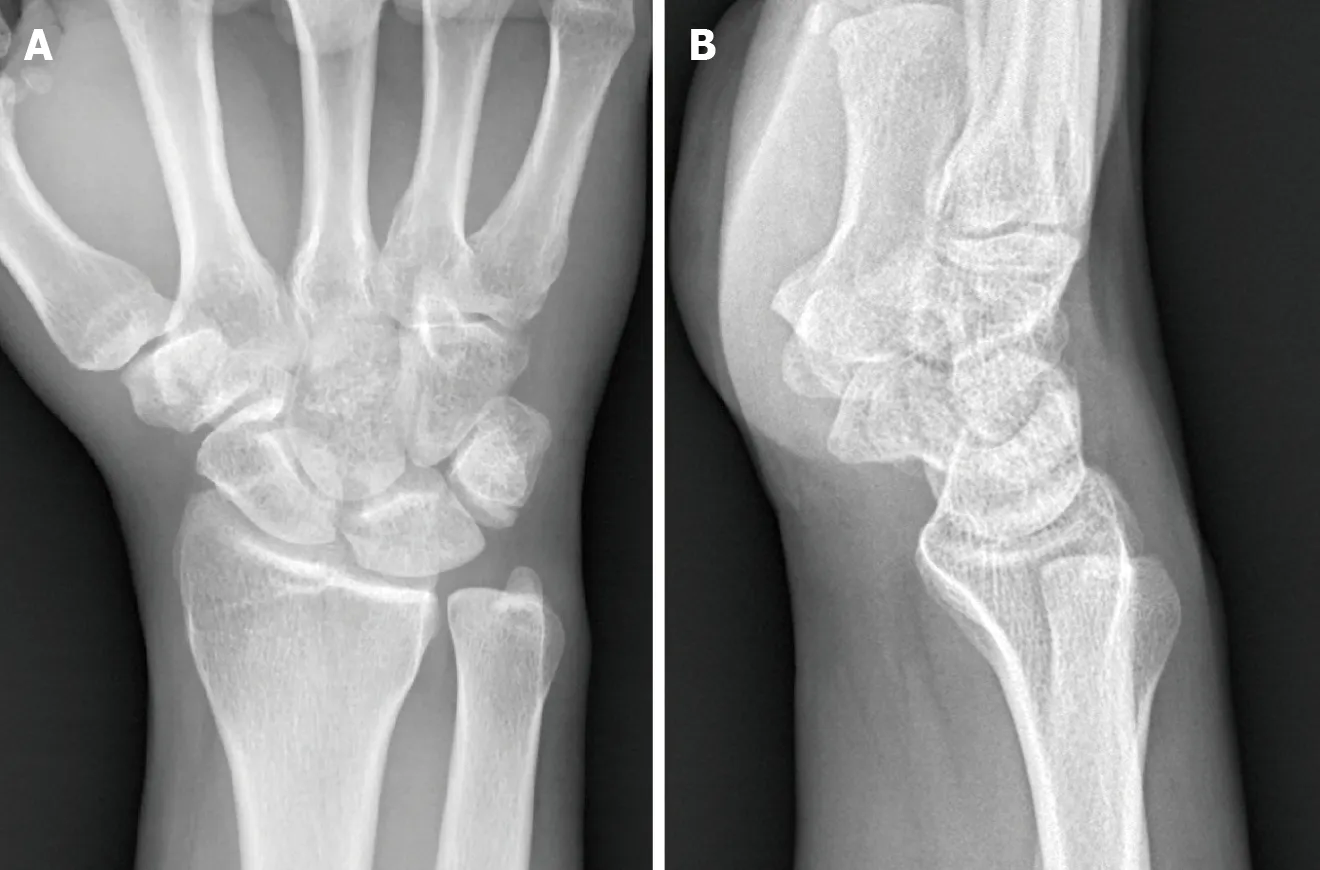
While waiting for facial bone surgery, the swelling and pain in the right wrist increased, with reduction in the range of motion. An orthopedic surgeon was consulted and re-evaluation of the plain radiograph of the right wrist revealed a triangular appearance of the lunate (piece of pie) with triquetral fracture in the anteroposterior view, and angulation and volar displacement of the lunate (spilled tea cup) in the lateral view (Figure 1)[4].
Non-contributory.
That s the 6.20 from Crewe, he said, nursing an unfiltered() Park Drive in his brown coated fingers- then another glance at his watch, He s ten minutes late.
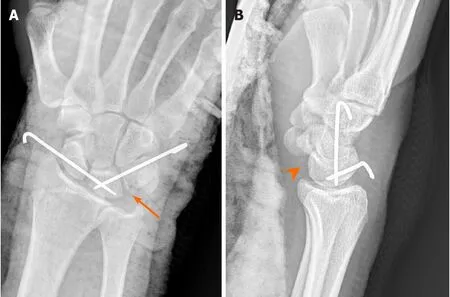
The patient was taken to the operation room approximately 30 h after sustaining trauma. We first tried closed reduction again under general anesthesia using Tavernier’s method, first described in 1906[6]. Fortunately, the dislocated lunate could be reduced with gentle manual traction and slight wrist extension. This was followed by fixation using two Kirschner wires for maintaining reduction (one from the scaphoid to the lunate, and the other from the triquetrum to the lunate). The surgical course was uneventful, and only two pin holes were created (Figure 2). The wrist was immobilized for 4 wk with short arm orthosis and hand therapy for another 8 wk.
OUTCOME AND FOLLOW-UP
Today, I keep that key in my dresser drawer and treasure it. Whenever I hold it in my hand, I am reminded of all the wonderful things Dad has done for me over the years. I realize that, although he is now 68 and I am 40, I still look to him for wisdom, guidance and reassurance15. Most of all, I marvel16 at the fact that his thoughtful gesture of making the extra key may have saved my life. And I understand how a simple act of love can make extraordinary things happen.

DISCUSSION
Lunate injury or peri-lunate injury may be easily missed at the initial presentation. According to the literature, approximately 25% of cases are associated with missed or delayed diagnosis. Lunate injury may result in progressive carpal instability, median neuropathy, avascular necrosis of the lunate, and end- to post-traumatic arthritis of the wrist joint[7]. The mechanism of injury is forced hyperextension, ulnar deviation, and intercarpal supination of the wrist[8].
Mayfield described the pattern of progressive peri-lunate instability in 1984[5]. In stage I, the distal carpal row is forced into hyperextension, and the scaphotrapezoid-capitate ligaments extend the scaphoid, opening the space of Poirier, resulting in a complete scapholunate dissociation. In stage II, the scaphoid-distal row complex may dislocate dorsally relative to the lunate. In stage III, persistent hyperextension may lead to the ulnar limb of the arcuate ligament pulling the triquetrum dorsally, causing failure of the lunotriquetral ligaments. In stage IV, the capitate may be forced by the still-intact radioscapho-capitate ligaments to push the lunate forward until it dislocates rotationally into the carpal canal.
Treatment of lunate or peri-lunate injury is currently challenging, given its rarity and high complication rate. The goals of surgical management are confirmation of reductions, ligamentous repair/reconstructions, fixation of associated fractures, and supplemental fixation of the bony architecture to facilitate ligamentous healing. The surgery can be performed through volar, dorsal, or combined approaches with carpal tunnel release. Herzberg suggested the single dorsal approach for cases in which the rotation of the dislocated lunate is less than 90°, and the double approach when the rotation of the bone is more than 90°[9]. However, several studies have demonstrated comparable outcomes. Thus, the choice of approach is largely influenced by surgeon preference[10-13].
This is the first such case in our practice to be treated with closed reduction and percutaneous Kirschner wires fixation. The reduction technique is meticulous and crucial. Although we agree that the closed reduction method can only be used in earlydiagnosed cases of acute lunate dislocation, this surgical technique can provide an alternative treatment option that may be useful in selected cases.
CONCLUSION
This case provides evidence that the closed reduction technique for addressing acute lunate dislocation and managing triquetral fracture can reduce soft tissue destruction with the use of ligamentotaxis reduction. Postoperative 18 mo follow-up showed satisfactory outcome without progressive sequelae of carpal joint arthritis.
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Hepatitis B virus reactivation in rheumatoid arthritis
- Paradoxical role of interleukin-33/suppressor of tumorigenicity 2 in colorectal carcinogenesis: Progress and therapeutic potential
- Changes in rheumatoid arthritis under ultrasound before and after sinomenine injection
- Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients
- Outcomes and complications of open, laparoscopic, and hybrid giant ventral hernia repair
- Surgical resection of intradural extramedullary tumors in the atlantoaxial spine via a posterior approach