
Eustachian tube teratoma: A case report
2022-02-11 05:29JinYeLiLiXinSunNaHuGeShengSongWeiQiangDouRuoZhenGongChuanTingLi
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Teratomas of the head and neck account for 5%-15% of all teratomas and principally involve the nasopharynx and neck[1]. Reports of teratomas involving the temporal bone are scarce[2,3]. Herein, we present a case of mature teratoma of the eustachian tube (ET) in an adult male with a history of chronic otitis of the left ear from infancy.
CASE PRESENTATION
Chief complaints
A 48-year-old man was referred to our hospital for chronic otitis, cholesteatoma and a middle ear mass.
History of present illness
The patient had experienced chronic otitis of the left ear from infancy and underwent surgery for cholesteatoma in the tympanum at another hospital. However, his clinical symptoms had persisted. His conscious hearing was poor, and he suffered from earache, ear boredom, headache and dizziness.
History of past illness
The patient had no significant past medical history.
Personal and family history
The patient’s family history was unremarkable.
Physical examination
Then the doll s eyes began to shine like two stars and it became alive. It ate a little and said: Do not fear, little Vasilissa. Go where thou hast been sent. While I am with thee no harm shall come to thee from the old witch. So Vasilissa put the doll back into her pocket, crossed herself and started out into the dark, wild forest.

Laboratory examinations
His daughter reflected for a moment, and then said: Dear father, I wish for eleven girls as nearly as possible of the same height, age, and appearance as myself
The laboratory examination was otherwise unremarkable. The laboratory assessment included routine blood tests. Tests for C-reactive proteins and viral hepatitis markers were negative. Glucose and serum insulin levels were normal.
Imaging examinations
The ET diameter was expanded, to about 0.8 cm. The part of the mass in the tympanum and external auditory canal was classified as a fleshy polyp. However, “hairs” were visible on the surface of the mass and cartilage surrounded by the mass could be seen in the ET area (Figure 1). The mass, in which the anterior lower part and posterior upper part were connected by a thin membranaceous tissue, was in the ET. It was tightly bonded to the former ET wall and could not be removed, so serial partial excision was performed. The resulting cavity (composed of the tympanum and external auditory canal) was then resolved by filling with abdominal fat.
Pathological results
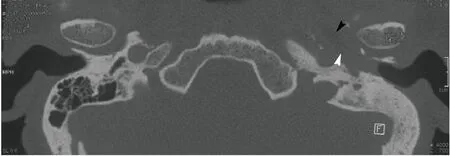
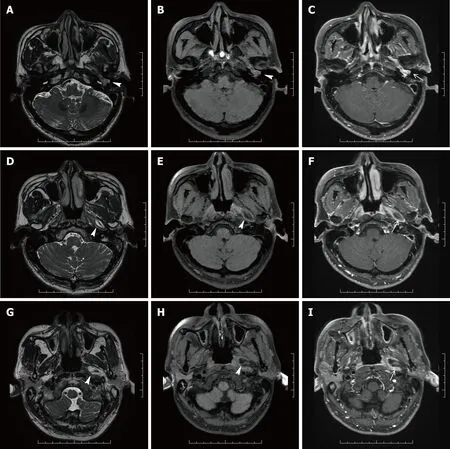
The unenhanced computed tomography (CT) of the temporal bone showed some changes, including a well-circumscribed, mixed density tumor with a fat density area in the ET; the lesion extended down to the left part of the tympanum and external auditory canal (Figure 2), without ossicular chain, which had resulted from the mastoidectomy. The T1- and T2-weighted magnetic resonance imaging (MRI) in the transverse plane showed a 3.2 cm × 1.3 cm × 2.0 cm, well-defined, homogeneous lesion with high signal intensity along the left ET. The mass showed signal intensity similar to that of the fat on all sequences and with little cartilage signal (Figure 3). The lesion extended down to the left part of the tympanum and external auditory canal, where the signal was slightly higher than the part in the ET. On fat-saturated T1- and T2-weighted sequences, the part of the mass in the ET demonstrated a decreased signal intensity, indicating that the mass was consistent with macroscopic fat. The mass was surrounded by a smooth, thick, hypointense capsule, which was enhanced slightly after contrast administration.
No sooner had he placed it in the Princess s mouth than she opened her lovely eyes, and, looking up into the happy youth s face, she kissed him tenderly, thanked him for freeing her from her magic sleep, and promised to be his wife
On gross examination, the resected mass appeared as a cluster of irregular, soft, grey-colored tissue. Microscopically, a photomicrograph of the mass revealed characteristics of keratinized squamous epithelium, adipose, sweat gland and mature skeletal muscle tissues. Photomicrographs of the areas including the tympanum and external auditory canal revealed squamous epithelial mucosal polyps (Figure 4).
Otoscopic examination demonstrated a large amount of pus in the left external auditory canal, a fleshy polyp present at a deeper site, and mucosal edema in the previously operated area (Figure 1). Audiometric assessment confirmed a severe conductive hearing loss; hearing threshold was 80 dB and auditory brainstem response was 70 dB on the affected side. Nasopharyngoscopy showed that the orifice of the left ET opened well.

FINAL DIAGNOSIS
The mass was removed completely by mastoidectomy, with the patient under general anesthesia.
TREATMENT
Mature teratomas.
The dwarf could not refuse this request, and so they all went together through the beautiful green paths and flowery meadows, and came at last to the river which flowed for miles round the Princess s land and formed the boundary of her kingdom
OUTCOME AND FOLLOW-UP
After follow-ups at 7 mo and 2 years, the patient showed no signs of disease relapse.
DISCUSSION
Mature teratoma is a true neoplasm composed of all three basic germ cell layers (ectoderm, mesoderm, and endoderm), which differs from dermoids and epidermois[4]. Most cases involve a midline or paraxial location, and the most common site is in the sacrococcygeal region (40%-60% of cases)[5]. Only 2%-10% of cases have involved the head and neck regions[5], especially the cervical and nasopharyngeal regions. We used the PubMed database to search for relevant publications on (keywords) “mature teratoma” and “eustachian tube”. We found only eight relevant publications among the English-language literature, excluding reports on dermoid cysts, which represent a special category of teratomas. According to the histologic classification of teratomas in the head and neck region that is most commonly used today, the term ‘dermoid’ (as it was proposed by Arnold in 1888) is most appropriate[6]. This implies an origin from epidermal and mesodermal elements, which differentiates them histologically from teratomas composed of elements from all three germinal layers and from cholesteatomas, which are only of ectodermal origin[7]. Of these 9 total cases reported to date (including this case), 4 were male and 5 female; the near 1:1 ratio indicates that there is no sex preponderance for ET teratoma. The age of the 9 patients ranged from 1 d to 48 years, with a median of 10-mo-old. The cases had various clinical manifestations, as follow: foul-smelling left otorrhea[8], peripheral palsy of the seventh cranial nerve[5], a tongue-like structure which protruded when the patient cried and retracted into the mouth when swallowing[9], a history of refractory otitis media and a nasopharyngeal mass[3], a discharging left ear since infancy[10], respiratory distress in a premature infant[11] with recurrent otitis media and chronic otorrhea of the left ear[12], and a history of chronic otitis of the right ear from infancy[13]. However, all these manifestations were due to obstruction of the channel or oppression of the surrounding structures.
The case presented here is the first reported for an ET teratoma with the anterior lower part and posterior upper part connected by a thin membranaceous tissue, accompanied by a fleshy polyp in the tympanum and external auditory canal. The patient, who had a history of chronic otitis of the left ear from infancy, was older than the other 8 patients reported for previous cases. It is, therefore, possible that the history of chronic otitis of the left ear and previous operations he underwent led to the formation of a fleshy polyp in the tympanum and external auditory canal. Of note, in patients with a history of chronic otitis that exhibit polyps in the tympanum and/or external auditory canal, it is important to avoid the assumption that these are merely a result of inflammation. Equally important is to avoid making an immediate call for surgery. Both CT and MRI examinations must be performed to appraise the condition of the ET and identify possible neoplasms. For our patient, the only examination made before his previous surgery was a CT scan. This led to the failure of identifying the ET tumor. Had a preoperative MRI examination been conducted, the ET tumor would likely have been detected and the following operation would have addressed both the inflammation and the tumor.
Ultrasound is an ideal initial imaging modality to investigate neck masses, as it reveals the solid or cystic nature in most cases and localizes the lesion in relation to surrounding structures[14], but it has some limitations when applied to the temporal bone region. A combination of CT and MRI scans provides valuable clinical information to exclude alternative cranial base pathologies and assess the extent of the lesion. The CT scan allows for better evaluation of the bone architecture, whereas the MRI scan can better demonstrate the relationship between the mass and the carotid artery beneath the temporal bone[7]. The typical clinical presentation of ET teratomas includes recurrent episodes of otitis media and chronic otorrhea[15,16], caused by the obstruction of the ET by the teratomas. Ultimately, ET teratoma requires surgical removal and has excellent prognosis upon complete resection[12].
At first I was grieved to see Lolotte cry, resumed the Princess, but I soon found that grieving was very troublesome, so I thought it better to be calm, and very soon afterwards I saw the Fairy Mirlifiche arrive, mounted upon her great unicorn110
CONCLUSION
In summary, this case highlights the necessity of examinationa combination of CT and MRI pre-operation for ET teratoma. The surgical removal itself provides an excellent prognosis upon complete resection.
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Hepatitis B virus reactivation in rheumatoid arthritis
- Paradoxical role of interleukin-33/suppressor of tumorigenicity 2 in colorectal carcinogenesis: Progress and therapeutic potential
- Changes in rheumatoid arthritis under ultrasound before and after sinomenine injection
- Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients
- Outcomes and complications of open, laparoscopic, and hybrid giant ventral hernia repair
- Surgical resection of intradural extramedullary tumors in the atlantoaxial spine via a posterior approach