
Awareness and knowledge about glaucoma among patients visiting the screening clinic in Jeddah Eye Hospital, Saudi Arabia
2021-06-11 00:49SalehAlqahtaniMarwanBakarmanAhmedAlmanjoumiSamiAlzahrani
Saleh M. Alqahtani, Marwan A Bakarman, Ahmed Almanjoumi, Sami H. Alzahrani
1Ministry of Health, Jeddah 23545, Saudi Arabia
2Department of Family and Community Medicine, Faculty of Medicine in Rabigh, King Abdul Aziz University, Jeddah 21589, Saudi Arabia
3Ophthalmology Department, Faculty of Medicine, King Abdulaziz University, Jeddah 22234, Saudi Arabia
4Family Medicine Department, Faculty of Medicine, King Abdulaziz University, Jeddah 22431, Saudi Arabia
Abstract
● KEYWORDS: awareness; knowledge; glaucoma; Saudi Arabia
INTRODUCTION
Glaucoma comprises a set of heterogeneous diseases which differ in their causes, risk factors, symptoms,and treatment. Glaucoma is referred to as a progressive loss of vision due to acquired loss of retinal axons and ganglion cells within the optic nerve with a subsequent development of the peculiar optic nerve head appearance. Such peripheral loss of vision is a unique feature of glaucoma[1]. It occurs silently,leading to irreversible optic neuropathy. In adults, glaucoma is classified into primary openangle (OAG) and angle‐closure(ACG), and secondary OAG and ACG according to the morphology of the anterior chamber[2].
Glaucoma has been adopted as the most common cause of irreversible blindness globally, affecting approximately 60 million individuals[3‐4]. However, it ranked fourth as the leading cause of moderate or severe vision impairment in 2015 following uncorrected refractive error, cataract and macular degeneration, where the number of blind individuals attributable to glaucoma was estimated as 4.0 million (80%uncertainty interval 0.6 million to 13.3 million)[5]. Furthermore,the global disability‐adjusted life year increased by 81% from 1990 to 2017[6]. Regionally, glaucoma remains a significant cause of visual impairment, where surgical rates due to the condition ranged between 30 to 68.6 surgeries/million/year in the North Africa and the Middle East region[7]. It accounted for 6.94% and 1.62% of total cases of blindness and moderate‐to‐severe visual impairment in 2015 and these numbers are projected to increase significantly in 2020[8]. In Saudi Arabia, to the best of our knowledge, no available nation‐wide prevalence studies have been conducted. Evidence from distinct regions indicated that primary OAG was the most prevalent type in 60% and 30.5% of patients in the eastern and western regions, respectively[9‐10]. However, Al Obeidanet al[11]had shown that primary ACG was the predominant type in Riyadh. As such, more epidemiological studies are needed across the country to address the typical prevalence patterns as well as the distribution of different glaucoma subtypes.
The most significant risk factors of glaucoma include older age, increased intraocular pressure (IOP) in relation to the pressure sensitivity of the optic nerve head, family history, and ethnicity[1]. IOP‐lowering medications, such as beta‐blockers,prostaglandin analogs, and carbonic anhydrase inhibitors, are usually given for patient management. In some instances, the efficacy of these drugs to arrest glaucomatous progression is questionable[12]. Surgical approaches, including laser trabeculoplasty and trabeculectomy, are also available upon the failure of medical treatment.
However, early detection of the disease is paramount to accomplish good therapeutic outcomes, yet it is often difficult to achieve, particularly in line with the lack of reliable screening tools. It has been shown that more than half of patients with glaucoma remain undiagnosed and the majority of them are frequently detected at late stages[13‐14]. One of the significant factors that contribute to late presentation is the lack of awareness about disease nature and risk factors and subsequently failure to seek for medical care and treatment[15].Lack of awareness about the disease may not only affect the timing of diagnosis, but also using healthcare services. In Saudi Arabia, little is known about the levels of awareness about glaucoma. Moreover, in the light of a personal experience,several glaucomatous patients failed to perceive the relevance of starting medications until a visual defect takes place. One of the pertinent settings to assess awareness levels is the local eye care specialty centers.
The objectives of this study were to assess awareness and knowledge about the following glaucoma‐related dimensions:types, clinical features, risk factors, and management; to compare the level of knowledge among patients who are already diagnosed with glaucoma versus the others; and to explore sources of information about glaucoma and analyze the effectiveness and reliability of each source by analyzing the associated levels of knowledge.
SUBJECTS AND METHODS
Ethics ApprovalThe protocol of the present study was approved by the Research Ethics Committee (REC) of King Abdulaziz University, Jeddah, Saudi Arabia (Reference No.199‐18). Written informed consent was obtained and documented from all participants for participation and publishing. They were informed about the nature of the study and confidentiality of their response. A written consent was obtained from all participants prior to inclusion.
Data StatementAll original data is available in the Department of Family Medicine, King Abdulaziz University, Jeddah, Saudi Arabia. Data used to support the findings of this study are available from the corresponding author upon request.
This analytical cross‐sectional study was carried out at the screening clinic in Jeddah Eye Hospital, Jeddah, Saudi Arabia during the period 01/10/2018‐31/12/2018. Jeddah Eye Hospital is one of three specialized eye hospitals in Saudi Arabia. With its 100 beds and comprehensive subspecialties, JEH covers the western coast area of Saudi Arabia. The study protocol and questionnaire were approved by the Directorate of Health Affairs, Ministry of Health, Jeddah. Additionally, permission was sought from the JEH administrator. Included in this study,all patients aged ≥ 18 years old. Excluded from the study were patients with eye trauma or ocular comorbidities.
The number of patients attended to screening clinic last year(2017‐2018) was 113 036 patients. Using the equation from raosoft.com website, we calculated the sample size for an unknown proportion of adequate knowledge level (P=50%)within a finite population of 113 036, with 5% margin error,95% confidence interval and 80% statistical power. The target sample size was calculated asn=383. Three hundred and eighty‐three participants were included in this study with a mean±SD was 38.50±12.94 years old.
A convenience sampling technique was used to include all eligible and consenting participants until reaching the target sample size. Data collection used a semi‐structured questionnaire, which was designed by the researcher for the purpose of this study. The questionnaire contains 4 parts:The first part recorded the sociodemographic and clinical data including age, gender, educational level, mother tongue,personal history of diabetes or glaucoma and family history of glaucoma. The second part regarded awareness about glaucoma including one question: have you ever heard about glaucoma? The third part consisted of sources of information about glaucoma including TV, newspaper, magazines, friends,a person with glaucoma and physician. The fourth part assessed knowledge about glaucoma including 18 items divided into 4 domains: 1) types of glaucoma; 2) risk factors; 3) clinical features; 4) management. The questionnaire underwent face and content validity with the contribution of a consultant ophthalmologist. Reliability testing of knowledge scale based on the scoring system showed Cronbach’s alpha=0.782 (18 items), indicating good internal consistency.
The researcher approached all patients attending the ophthalmology screening clinic at JEH, introduced himself and invited the patients to participate after having explained the objectives and importance of the study project. All eligible participants were provided with a hard copy of the questionnaire and relevant instructions were given to enable self‐administration the questionnaire. The average time required for filling the questionnaire ranged between 10‐15min. The answered questionnaires were collected back by the researcher in the same day.
Data Entry and AnalysisStatistical analysis was performed with the Statistical Package for Social Sciences version 21.0 for Windows (SPSS Inc., Chicago, IL, USA). Categorical variables are presented as frequency and percentage, while continuous variables are presented as mean±SD. Analysis of factors associated with knowledge was done using two different methods. In the first method, nonparametric tests including Mann‐WhitneyUtest and Kruskal‐Wallis test, as appropriate, were used to compare knowledge score across the different factor categories; results are presented as median and 75thcentile (P75). In the second method, a cutoff score≥9/18 was assumed to indicate adequate knowledge, and Chi‐square test was used to compare the percentage of respondents with adequate knowledge between the factor categories.Additionally, independentt‐test was used to compare mean±SD age between the group of individuals with inadequate versus adequate knowledge.P<0.05 was considered to reject the null hypothesis.
RESULTS
Participants’ CharacteristicsRegarding gender, males(61.9%) were higher than females (38.1%). Most of the participants had high educational level (university degree or higher; 61.6%) and from Arabic‐speakers areas (95.3%),among who 4.4% were bilingual. Medical history showed that 15.1% of participants had diabetes mellitus that may affect eye status, 6.30% had glaucoma and 23.20% had positive family history of glaucoma (Table 1).
Sources of Information about GlaucomaThe most frequently reported source of information about glaucoma was another person with glaucoma (28.2%), followed by physicians (24.8%), TV (19.6%), friends (16.7%), magazine(7.8%), newspaper (4.4%), and finally radio (3.7%) indicating important of friends, physicians and social media in getting information of disease (Figure 1).
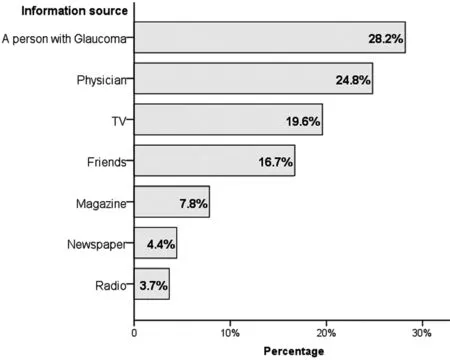
Figure 1 Source of information about glaucoma.

Table 1 Participants’ sociodemographic characteristics n=383
Awareness and Knowledge AssessmentThirty percent of the respondents (n=115) declared being unaware about glaucoma. Of all respondents, 33.4% acknowledged the existence of different types of glaucoma; and identified closed‐angle (26.9%), open angle (16.2%) and congenital (11.2%)as different glaucoma types, while 17.5% replied cataract as glaucoma types and 4.2% respond others. Treatment knowledge 25.8% believed vision loss due to glaucoma is temporary, 4.7% believed it cannot be treated and 47.0%,23.5% and 23.0% mentioned eye drops, laser, and surgery as glaucoma treatment options, respectively (Table 2). These results indicating the poor knowledge and awareness about glaucoma among participants.
Knowledge about risk factors is depicted in Figure 2 and showed family history of glaucoma (39.2%), increased eyepressure (37.6%) and steroid medication used (18.5%), as being the most frequently identified risk factors followed by others (15.7%), chronic smoking (15.1%), obesity (11.7%) and alcohol consumption (3.1%). These results revealed that most of participants were unaware about most important risk factors of glaucoma.
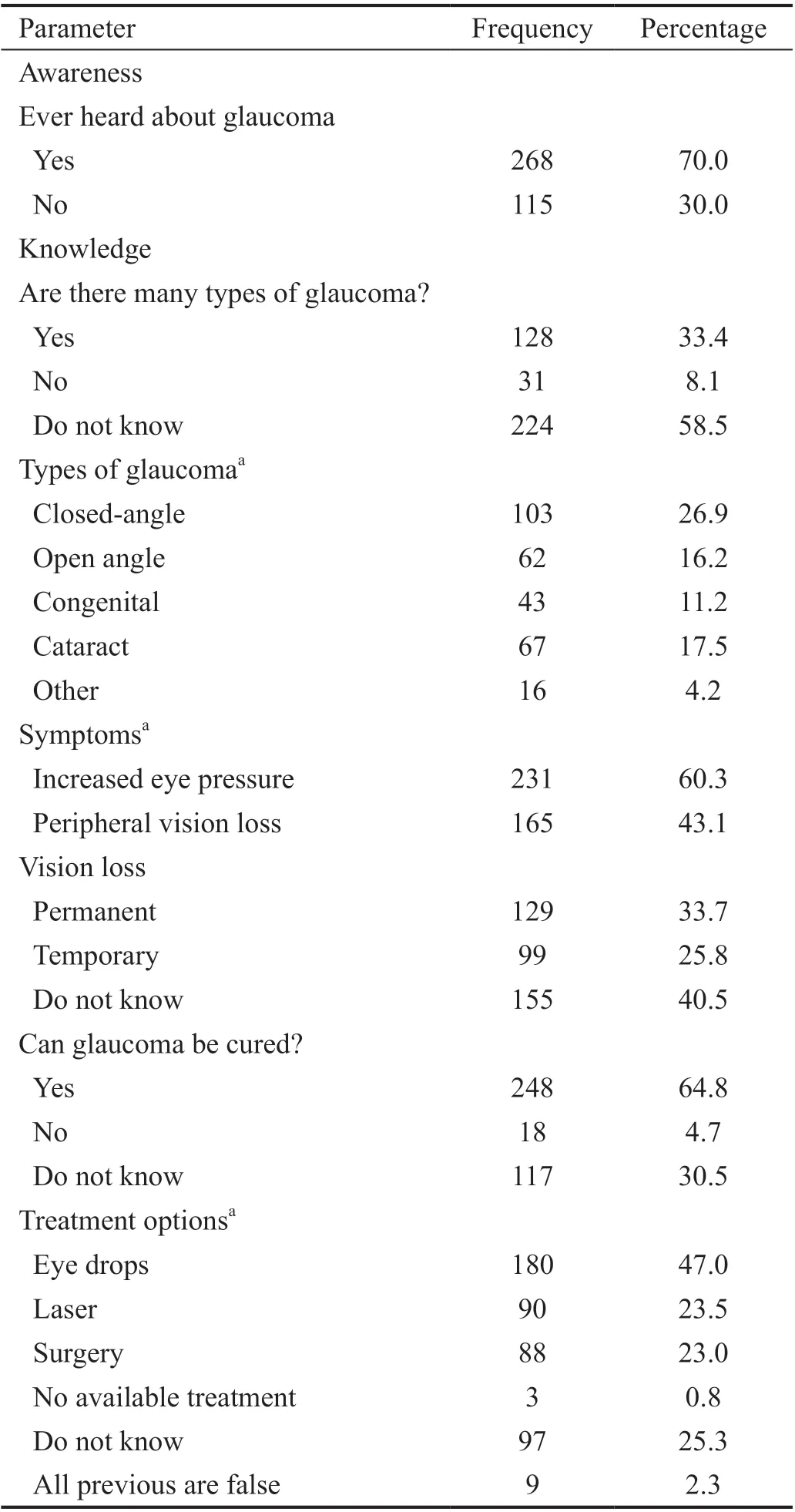
Table 2 Awareness and knowledge about glaucoma n=383
Knowledge Levels by ItemFor each knowledge item,a correctness rate was calculated as the percentage of respondents who replied correctly; results are presented in Figure 3. In glaucoma types, rate ranged from 11.2% for correct identification of congenital glaucoma as glaucoma type to 82.5% for correct identification of cataract as being not a glaucoma type. In risk factors, rates ranged from 3.1% for alcohol consumption to 39.2% for positive family history of glaucoma. For clinical features, 33.7% only correctly replied that vision loss was permanent; while 43.1% and 60.3%correctly identified peripheral vision loss and increased IOP as being sign of glaucoma, respectively. Regarding management,only 23%, 23.5% and 47.0% identified the three glaucoma management options including surgery, laser, and eye drops,respectively.

Figure 2 Knowledge about glaucoma risk factors (RF).

Figure 3 Corrected knowledge about glaucoma by item among the total study population.
Knowledge Level by Knowledge ScoreKnowledge score was calculated as the number of correct answers to the 18 knowledge items (score range=0‐18). The histogram of scores’ distribution is presented in Figure 4 and normality analysis of knowledge score variable showed Shapiro‐Wilk(statistics=0.925,P<0.001) tests, indicating non‐normal distribution. Mean±SD score of total study population was 5.91±3.52 and median was 5 out of 18.
Factors Associated with Knowledge LevelHigher knowledge scores were found among highly educated respondents (P=0.036), those who declared having personal history of diabetes mellitus (P=0.025) or glaucoma (P<0.001),as well as those who have family history of glaucoma(P<0.001) compared to their counterparts (Table 3). These results indicated the important of education in getting accurate knowledge.
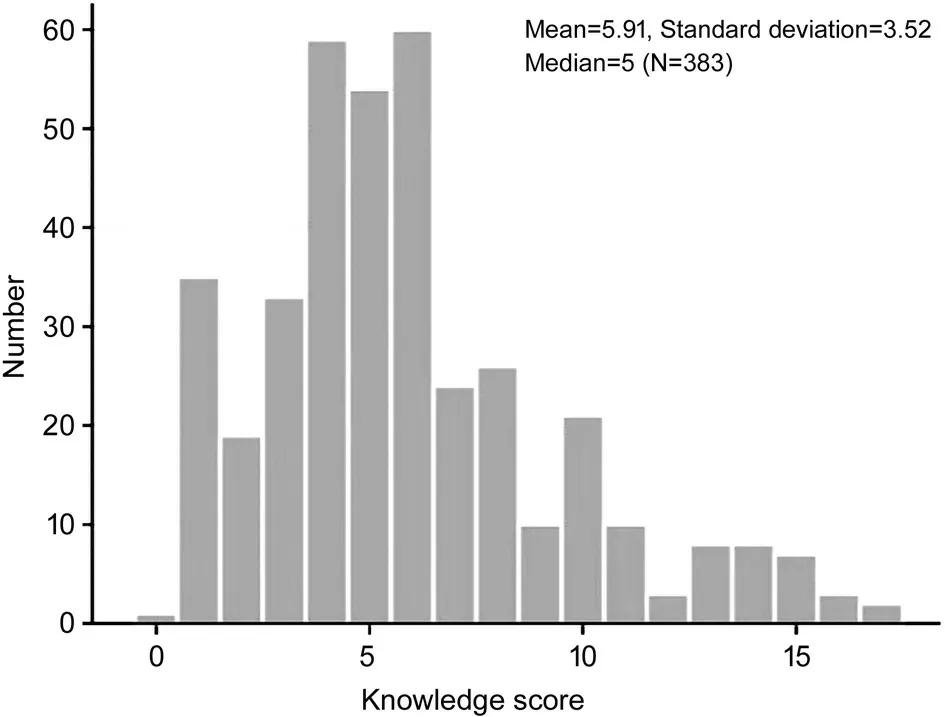
Figure 4 Distribution of knowledge score about glaucoma among the studied population.
The percentage of respondents with adequate knowledge(score≥9/18) was 18.8% (95%CI=15.0%‐23.1%). This indicates low knowledge level among the study population.There were significant difference in individuals with adequate versus those with inadequate knowledge regarding diabetes mellitus history (yes: 29.3%vs70.7%; no: 19.8%vs80.2%;don’t know: 0vs100%;P<0.001), glaucoma history (yes: 45.8%vs54.2%; no: 19.3%vs80.7%; don’t know: 5.2%vs94.8%;P<0.001) and family history of glaucoma (yes: 29.2%vs70.8%;no: 18.5%vs81.5%; don’t know: 8.4%vs91.6%;P=0.002).Of all information sources, respondents who declared having received information by their physician had significantly higher percentage of adequate knowledge (50.5%) compared to their counterparts (50.5%vs8.3%,P<0.001; Table 4).
DISCUSSION
Public awareness and knowledge about glaucoma represent an important pillar in promoting public health‐seeking behavior and enhancing detection of unidentified cases. Patients with the required information is a clinically beneficial and cost‐effective approach to reduce the progression or deterioration of the visual field and improve patients’ compliance to treatment[16‐17].The results of the present study showed that Saudi individuals had low levels of awareness and knowledge regarding glaucoma as indicated by a mean knowledge score of 5.91(out of 18) and only 18.8% had adequate knowledge (scored≥9). Among knowledgeable individuals, the results of this study identified that other glaucomatous patients, physicians,and television as being the main sources of knowledge, and personal and family histories of glaucoma, as well as personal history of diabetes mellitus contributed significantly to improving knowledge levels.
The rates of acceptable knowledge of this study (18.2%) was quite similar to that reported in patients attending the Ministry

Table 3 Factors associated with knowledge score n=383
aStatistically significant;mMann‐WhitneyUtest;kKruskal‐Wallis test.of Health clinics in Aljouf and Hail region (16.9%)[18]and in an outpatient internal medicine clinic in the United States 14.6%[19]. However, it was lower than that reported in a survey‐based study conducted among the attendees of an ophthalmology clinic at King Abdulaziz University Hospital (Riyadh)[20], where 54.8% of the participants had a good knowledge (scored ≥10 out of 15). Additionally, 36.8%of the participants of an outreach program in Nigeria were knowledgeable about glaucoma[21]. The levels of glaucoma knowledge were lower in other countries, where 2.4% among those attending ophthalmic outreach services in Ethiopia[22]and 5.5% among patients presented to a free eye clinic in eastern Nepal[23]had adequate knowledge level. Knowledge variation among these different studies could be attributable to differences in urbanization, sources of knowledge, educational levels, and methodological designs. This may highlight the need for a standardized tool to assess knowledge and awareness about glaucoma to enable accurate intra‐ and inter‐population comparisons. Our rate of acceptable knowledge about glaucoma (18.8%) was relatively in agreement with glaucoma knowledge (14.8%) among Saudi adults in anonline questionnaire‐based study[24]. Similarly, 17.3% of the participants in a community‐based study in an urban area in Ethiopia were knowledgeable (score of ≥8.42 out of 15)[25].Other reported knowledge levels of 15.8% in Nigeria, 8.3% in North India, and 7% in Bangladesh[15,26].
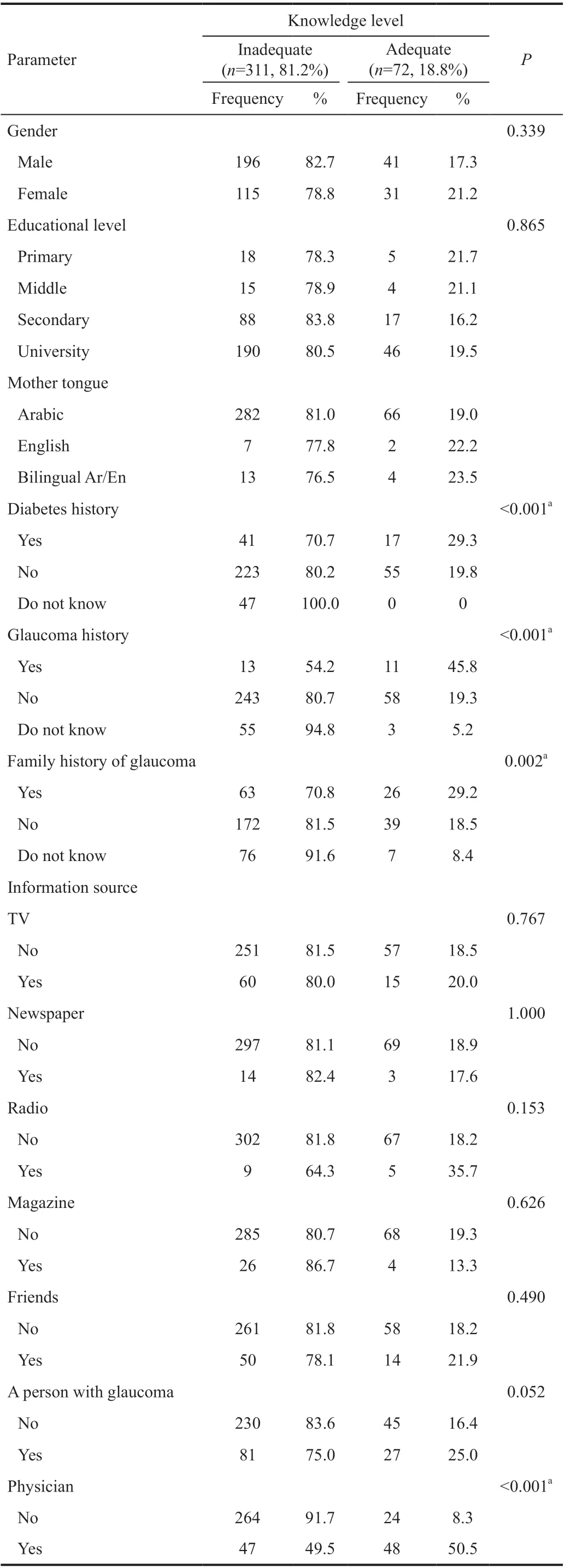
Table 4 Factors associated with knowledge level using score cutofflevel at ≥9 n=383
In this study, adequate knowledge was reported in 19.5% of participants with university, 16.2% with secondary school,21.1% middle school and 21.7% primary school education level. The contribution of health education was apparent specifically in the developing countries, such as Ethiopia,where highly educated participants had a significant increase in awareness levels compared to those received less than high school[22]. Meanwhile, in Ghana, all participants presenting to a teaching hospital who received a tertiary education were aware about the disease, while more than half of those with a middle education lack pertinent awareness[27]. High levels of education was associated with glaucoma awareness and knowledge in Saudi Arabia[18,20]and other parts of the world[21‐23,28]. Highly educated groups have better chances to access relevant information from mass media, internet and other sources, than their counterparts. Additionally, education improves public health through several causal pathways. First,the psychosocial environment, where social standing, social support, and personal sense of control are major influential factors. Second, a better access to health‐related resources could be seen in highly educated individuals. Finally, adopting a healthy behavior in educated persons could eventually raise their health awareness[29]. In Saudi Arabia, public health awareness evidenced a steady growth over the last two decades[24,30]parallel with the achieved progress in all public sectors. However, efforts should target enhancing awareness and knowledge levels through mass media and internet‐based resources.
The present study showed that having a personal history of glaucoma was significantly associated with better knowledge scores. Additionally, diabetic participants represented 15% of the total population under study and they had a significantly higher awareness compared to non‐diabetic peers. This is consistent study in India[31], where about 25% of the diabetic participants showed good knowledge about glaucoma. This observation can be explained by that diabetic patients may visit an ophthalmologist at some point of their lifetime for diabetes‐related ocular problems, and the treating physician had provided some information about glaucoma. A recent Meta‐analysis combined the outcomes of the relevant prospective studies and found an increased risk of primary OAG in diabetic patients[32]. While the potential mechanism for this association is still unclear, suggestions that diabetes‐induced vascular injuries in the retina and optic nerve may ultimately cause deteriorative damage to retinal ganglionic cells and initiation of glaucomatous impairment[33].
Individuals with a positive family history showed a significant increase in mean knowledge scores as well as being allocated to the adequate knowledge group. Generally, a positive family history has been reported in 13%‐25% of glaucomatous patients and it was associated with a two‐fold increase in risk of developing at least OAG[34]. In a patient‐directed survey,Grameret al[35]found that patients with a positive family history were diagnosed at younger ages when compared to those with a negative history, and this observation was consistent in all types of glaucoma. From another perspective,even with the presence of a glaucomatous patient within the family, the patient may fail to inform other family members.Hence, it has been early demonstrated that 27% of patients were unknowledgeable about glaucoma even in families with a positive history of glaucoma[36]. In a cross‐sectional study conducted in a campaign for awareness about glaucoma in Brazil, only 15 participants (out of 31 with a positive family history) were knowledgeable about the disease and they lack the required information about the necessity of regular eye examinations[37]. In agreement with our findings, acquaintances with glaucoma constituted the major source of information about the disease in multiple local international studies[18,23,38].Repeatedly, this signifies that having relatives with eye diseases, and more specifically glaucoma, can contribute to better knowledge and awareness.
This indicates the preference of asking a trustworthy person for useful information. Besides, physicians should consider their remarkable role in increasing patient’s knowledge. In this study, in patients who received their information from physician about 50.5% had adequate knowledge. However,the role of mass media, internet, and social media should be focused. The impact of mass media and television has been deemed significant in Nigeria[21]while internet‐based resources and social media accounted for about three‐quarters of all sources of knowledge about eye diseases in a Saudi study[30].The findings of the latter study were not surprising given that data collection was performed through an online platform and thus the participants are expected to frequently access online information. In China, Liet al[39]conducted a cross‐sectional survey consisting of 15 questions for individuals educated about glaucoma eitherviaan outpatient department or a mobile‐based education program through a social media service (WeChat). The authors found that the educated respondents through WeChat service scored higher compared to hospital‐surveyed participants[39]. Seemingly, internet‐ and mobile‐based resources provide more comfortable, quickly‐accessed, and updated information with high reliability if provided by trustworthy sources. As such, their role should be emphasized, considering the implementation of user‐friendly and instantly‐accessible interfaces.
The present study is not without limitations. First, it is a hospital‐based study. Despite low awareness and knowledge levels about glaucoma in our study, lower figures may be reported in community‐based studies since people in the general population have much less contact with healthcare providers and patients, which represent notable sources of information. Second, an obvious limitation is sampling bias due to the convenience sampling approach used in this study.Therefore, the sample may be relatively unrepresentative of the entire population. Third, response bias, as with other self‐report questionnaires, could be apparent due to particular responses provided by some participants.
In conclusion, irreversible blindness is the primary concern in glaucomatous patients. Early detection and treatment are paramount to prevent this inevitable consequence. Good awareness and knowledge about the disease are major determinants of diagnosis and treatment. The results of this study revealed low awareness and knowledge levels among the attendees of a local eye care hospital in Jeddah, Saudi Arabia.The participants revealed a mean score of 5.9, while only 18.8% scored less than 9 (out of 18). Several misconceptions about disease risk factors, clinical features, and management were identified. However, knowledgeable participants were highly educated. Positive histories of diabetes or glaucoma as well as a positive family history of glaucoma were the most significant associated factors with high knowledge scores. They declared also some important sources of information that could be focused on, such as other persons with glaucoma, physicians and mass media. Future research studies are warranted based on a population‐based sample to reveal awareness levels among the potentially undiagnosed individuals.
ACKNOWLEDGEMENTS
Conflicts of Interest: Alqahtani SM, None; Bakarman MA,None; Almanjoumi A, None; Alzahrani SH, None.
 International Journal of Ophthalmology2021年6期
International Journal of Ophthalmology2021年6期
- International Journal of Ophthalmology的其它文章
- A decrease in macular microvascular perfusion after retinal detachment repair with silicone oil
- Surgical outcomes in acute dacryocystitis patients undergoing endonasal endoscopic dacryocystorhinostomy with or without silicone tube intubation
- Dr. Father Wacław Szuniewicz, a forgotten pioneer in refractive surgery and his work in China
- Deterioration of Avellino corneal dystrophy in a Chinese family after LASlK
- A mutated CRYGD associated with congenital coralliform cataracts in two Chinese pedigrees
- Autophagy dysregulation mediates the damage of high glucose to retinal pigment epithelium cells