
Helicobacter pylori infection and susceptibility to cardiac syndrome X: A systematic review and meta-analysis
2021-05-29 01:52:42MohsenKarbalaeiAmirhosseinSahebkarMasoudKeikha
World Journal of Meta-Analysis 2021年2期
Mohsen Karbalaei, Amirhossein Sahebkar, Masoud Keikha
Mohsen Karbalaei, Department of Microbiology and Virology, Faculty of Medicine, Jiroft University of Medical Sciences, Jiroft 43317803, Iran
Amirhossein Sahebkar, Biotechnology Research Center, Pharmaceutical Technology Institute, Mashhad University of Medical Sciences, Mashhad, Iran
Amirhossein Sahebkar, Applied Biomedical Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
Masoud Keikha, Department of Microbiology and Virology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad 9177948974, Iran
Abstract BACKGROUND Cardiac syndrome X (CSX) is characterized by persistent angina with normal coronary arteries.Several pathophysiologic mechanisms have been introduced, particularly Helicobacter pylori (H.pylori) infection.AIM To investigate the association between H.pylori infection and CSX.METHODS All studies related to H.pylori infection and CSX were evaluated by comprehensive searches of global databases such as ISI Web of Knowledge, PubMed, Scopus, EMBASE, and Google scholar.Statistical analyses of selected articles were evaluated based on the summary odds ratio (OR).Finally, heterogeneity and publication bias were estimated using the I2 statistic and Cochrane Q-test as well as Begg’s and Egger’s tests.RESULTS A total of 11 studies met our inclusion criteria and 1435 patients (63% female, and 37% male) were reviewed.A significant association was observed between female patients and this syndrome (P = 0.02).Our results showed a positive association between infection with this pathogen and presence of CSX (OR: 5.65; 95% confidence interval [CI]: 4.17-7.64; I2: 82.20).However, no significant association was observed with cagA-positive H.pylori strains and this syndrome (OR: 0.97; 0.56-1.70 with 95%CI).Given the heterogeneity and publication bias, the results need to confirmed by further prospective investigation.CONCLUSION Based on our results, H.pylori infection is associated with an increased risk of CSX.This bacterium appears to play a major role in the pathogenesis of CXS by inducing persistent inflammation.
Key Words: Helicobacter pylori; Cardiac syndrome X; Cardiovascular disease; Infection; Meta-analysis; Coronary diseases
INTRODUCTION
Helicobacter pylori (H.pylori)is one of the most important human pathogens in gastric conditions, causing infections in 4-4.5 billion people worldwide[1,2].This bacterium successfully colonizes in the stomach in childhood and causes chronic infections[3].After being diagnosed by two Australian physicians, Barry Marshall and Robin Warren in 1994,H.pyloriwas classified as a class I carcinogen[4] by the International Agency for Research on Cancer.Although 85%-90% of infected individuals remain asymptomatic, 10%-15% of cases progress to severe clinical outcomes such as peptic ulcer disease, gastric adenocarcinoma, and gastric mucosa-associated lymphoid tissue (MALT) lymphoma[5].Most frequently, this bacterium is transmitted through gastrooral, fecal-oral, or oral-oral pathways[6].Today, there is ample evidence that the bacteria are isolated from out-of-stomach sites such as atherosclerotic plaques, synovial fluid and urine, suggesting thatH.pyloriplays an important role in extraintestinal disorders by dysregulating immune response or direct attack[7-14].According to the literature,H.pyloriinfection is significantly associated with hematological and cardiovascular disorders including iron deficiency anemia, primary immune thrombocytopenia, vitamin B12 deficiency, autoimmune neutropenia, antiphospholipid syndrome, plasma cell dyscrasias, atherosclerosis, and ischemic stroke[15-22].Surprisingly, many patients with various disorders such as chest pain, abnormal rest electrocardiogram and positive stress test have normal result of coronary angiogram; this disorder was first named cardiac syndrome X (CSX) by Harvey Kemp in 1973, and then was subsequently termed “angina with normal coronary arteries”[23].CSX is characterized by a variety of features such as angina-like chest pain, positive exercise testing, positive thallium testing, and normal angiography, and accounts for about 20% of chest pain cases[24-26].The prevalence of this syndrome is higher in women than in men[27].Several pathophysiologic mechanisms have been introduced for CSX including inflammation, endothelial dysfunction, genome polymorphism, dyslipidemia, hypertension, smoking, obesity, vasodilator stimuli, and insulin resistance[28-30].This syndrome has a poor prognosis and may lead to myocardial infarction following repeated hospitalization[31,32].The exact mechanism of CSX is not fully understood; however, factors such as chronic inflammation, endothelial dysfunction, and microvascular ischemia appear to be the most important risk factors for progression to CSX[33-35].On the other hand, the role of infectious agents (both viral and bacterial) in susceptibility to cardiovascular diseases (CVDs) has been suggested[36].According to extant evidence,H.pyloriinfection leads to CVDs through chronic inflammation and endothelial dysfunction (i.e.morphological and functional alterations in carotid artery or atrial stiffness)[37,38].According to a case report, eliminating this infection could reduce the incidence of CSX[39].Although several studies have confirmed the link between infection withH.pyloriand this syndrome, there are some studies with controversial results[40,41].Because no comprehensive study has been performed on the relationship between this infection and CSX, the present meta-analysis was undertaken to evaluate CSX susceptibility in patients withH.pylori.
MATERIALS AND METHODS
Search strategy and inclusion criteria
Initially, a systematic search was performed to evaluate the effects ofH.pyloriinfection on susceptibility to CSX.For this purpose, we focused on global databases such as ISI Web of Knowledge, PubMed, Scopus, EMBASE, and Google Scholar, as well as MeSHbased keywords such as “Helicobacter pylori,” “H.pylori,” and “Cardiac Syndrome X.” Relevant studies were retrieved regardless of publication date and language.The literature search process was conducted separately by two authors (Karbalaei M and Keikha M), and to avoid losing information, the references of each article were evaluated.
Study selection
The inclusion criteria were: cross-sectional, case-control, original, and cohort studies; studies associated withH.pyloriinfection and CSX; studies based on standard diagnostic methods forH.pyloriinfection; and studies on the human population.The exclusion criteria were: review articles, case-reports, and congress abstracts; duplicate studies; repetitive samples;in vitroor animal experiments; and unclear or insufficient data.Finally, 11 eligible studies were selected for analysis in this study[41-51].
Quality assessment and data extraction
At this stage, the Newcastle-Ottawa Scale was used to assess the quality of eligible articles.Required information such as first author, publication year, location of study, number of case-control samples, age, gender distribution, infection frequency, diagnostic methods, and reference number are listed in Table 1.
Statistical analyses
We pooled the data using statistical analysis software, Comprehensive Meta-Analysis version 2.2 (Biostat, Englewood, NJ, United States).The association betweenH.pyloriinfection and incidence of CSX was estimated based on the summary odds ratios (OR) and 95% confidence intervals (Cis).We used theI2index and the CochraneQ-test to determine the heterogeneity between studies.Hence,I2> 50 and CochraneQ-testPvalue < 0.05 were considered significant heterogeneity.Furthermore, in both high and low heterogeneity cases, the random-effects model and the fixed-effects model were used, respectively.Publication bias was also examined through funnel plots and Egger’s and Begg’s tests.
RESULTS
Literature search and data extraction
In this study, following an initial search in the global databases, we received 206 articles.After evaluating their titles and abstracts and removing duplicate full-text versions, 42 eligible articles were evaluated according to our inclusion criteria, and finally 11 articles were selected (Figure 1).
All selected studies were conducted during 2004-2018, and the geographical distribution of the articles was limited to some countries such as Iran, China, and Italy.In eligible studies, the enzyme-linked immunoassay and urea breath test were used to diagnoseH.pylori.In this meta-analysis, data from 1,435 participants including 649 CSX patients and 786 controls were evaluated.All cases of CSX were diagnosed by typical history of angina with normal or near normal coronary angiography plus a positive none-invasive test or abnormal ECG diagram.Of all patients, 36.61% were male and the rest were female.There was a significant relationship between female sex and getting CSX (P= 0.02); the mean ages of patients and the controls were 51.48 and 48.81, respectively.Despite the positive correlation in most studies, in three studies, this relationship was inconsistent, even the relationship between thecagAgene and CSX[47-49].In general, all eligible studies evaluated factors including hypertension, diabetes, hyperlipidemia, smoking, systolic/diastolic blood pressure values, serum homocysteine levels, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglyceride.
Association between H.pylori and CSX
Statistical analyses showed that the frequency of infection withH.pyloriin CSX patients was 77.3% (95%CI: 71.7-82,P= 0.01,I2= 89.47,Q= 66.51,P= 0.01; Begg’sP= 0.86; Egger’sP= 0.01), while that of infection in healthy individuals was 54.2% (95%CI: 50-58.3,P= 0.05;I2= 60.7,Q= 17.82,P= 0.01; Begg’sP= 0.13; Egger’sP= 0.03).Based on the summary OR, we found a strong positive association between this infection and CSX (OR: 5.65, 95%CI: 4.17-7.64,P= 0.01,I2= 82.20,Q= 56.19,P= 0.01; Begg’sP= 0.40; Egger’sP= 0.21), suggesting that patients infected withH.pylorimight be more susceptible to progression to CSX (Figure 2).
CagA is regarded as one of the main bacterial factors causing alterations in normal signaling pathways and dysregulation of actin-rearrangement, as well as induction of chronic and severe immune responses[52,53].Based on statistical analyses, no significant relationship was observed betweencagA-positive strains and susceptibility to CSX (OR: 0.97; 95%CI: 0.56-1.70;P= 0.93,I2= 0.00,Q= 0.006,P= 0.96).According to the literature, hypertension and hyperlipidemia are the most important CSX-related factors caused by chronic inflammation[31,54,55].H.pyloriinfectionviadysregulating the immune system (MALT lymphogenesis) may lead to disruption of normal homeostasis and basal metabolism, and eventually cardiovascular risk[56-60].Our results also indicate a positive significant relationship between infection caused by this bacterium and the presence of hyperlipidemia/ hypertension in CSX patients (OR: 3.33; 95%CI: 1.92-5.76; and OR: 2.30; 95%CI: 1.37-3.87, respectively).About 14.1% of CSX patients were smokers; however, there was no significant association between smoking and the risk of CSX (OR: 0.95, 95%CI: 0.62-1.45,P= 0.83).
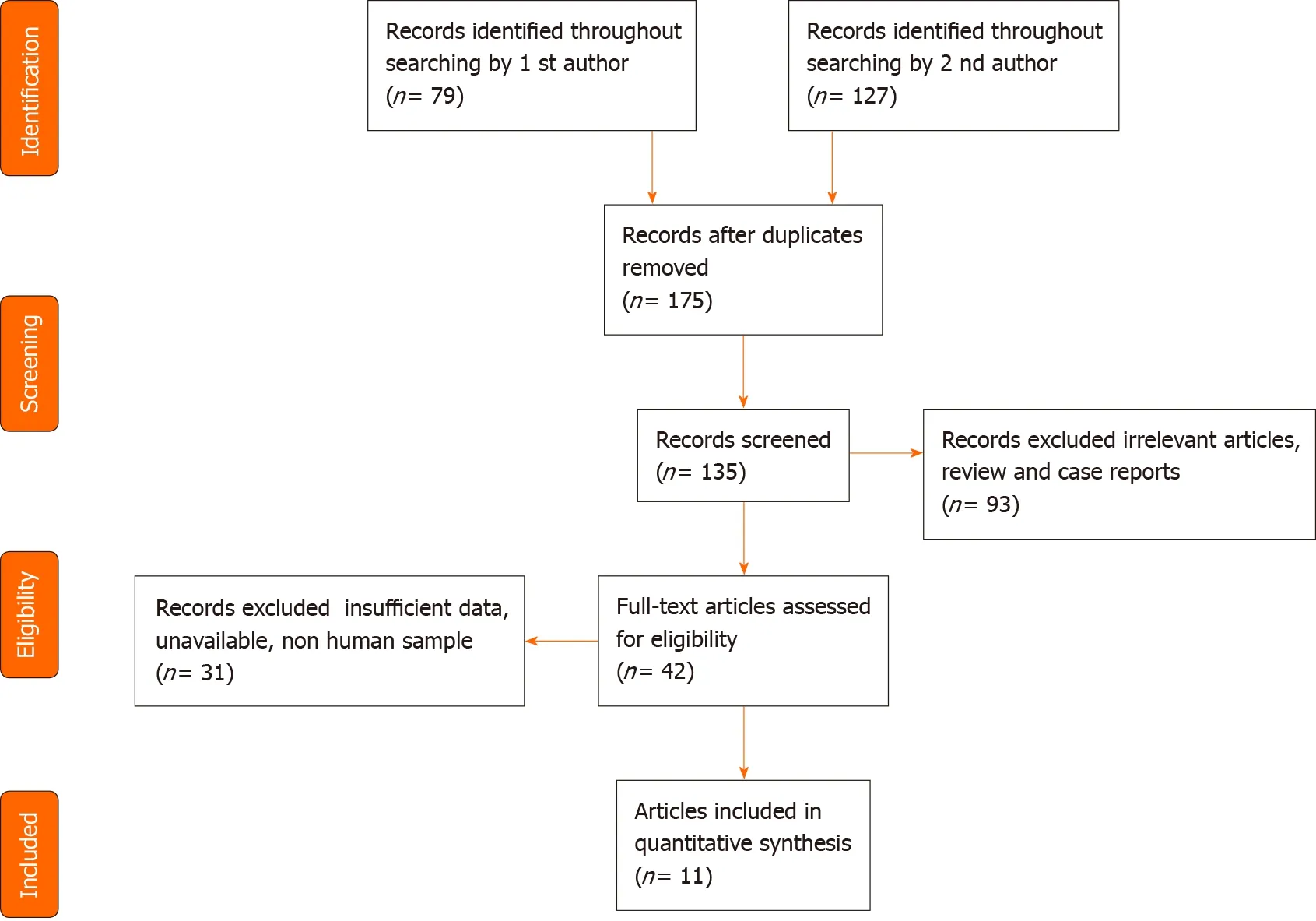
Figure 1 Flow-diagram of literature search and study selection.

Figure 2 The forest plot represents a probable association between Helicobacter pylori infection and susceptibility to cardiac syndrome X.
Publication bias
In the present meta-analysis, we evaluated publication bias using several tests such as Begg’s, Egger’s, and funnel plot evaluation (Figure 3).According to the results, there was significant publication bias that seems to be due to the low number of available articles.

Figure 3 Funnel plot of the meta-analysis on the association between Helicobacter pylori infection and cardiac syndrome X.
DISCUSSION
CSX is one of the heterogeneous syndromes in which cardiac (malfunction of Na-H+ pump, smooth muscle cell migration, endothelial dysfunction,etc.) and non-cardiac (sympathetic reactions, inflammation) mechanisms are involved[61].Although CSX is a multifactorial disease, the most important pathological factors associated with this syndrome are endothelial dysfunction, coronary artery disease, and myocardial ischemia[62,63].Recently, the role of inflammation in pathogenesis of CSX, has been defined[64,65].Pro-inflammatory cytokines, especially interleukin (IL)-1β, IL-6, and tumor necrosis factor alpha (TNF-α), cause several pathological changes, such as endothelial dysfunction, motility vessels, and microvascular stenosis, which in turn predispose to CSX[66].In general, infectious agents are considered risk factors for CVDs due to long-term stimulation of the immune response[67].Today, the role ofH.pyloriinfection in CVDs immunopathogenesis has received increasing attention[68].Immune responses (e.g.,cytokines and reactive oxygen species) against this pathogen lead to extracellular disorders[69,70].Innocentiet al[71] showed that this bacterium can activate endothelial cells.In another study, Oshimaet al[72] found that complications such as systemic inflammation and endothelial dysfunction were more common in patients infected withH.pylorithan in healthy individuals.In this study, we performed a comprehensive analysis of this association, and finally the results showed that there is a meaningful positive relationship between infection with this bacterium and CSX (OR: 5.65; 4.17-7.64 with 95%CIs).In their study, Rasmiet al[47] also showed a significant correlation between these two events in the Iranian population.Moreover, according to a study by Nocenteet al[39], eliminating infection can significantly contribute to CSX regression.Our results also showed that the rate ofH.pyloriinfection is higher in CSX patients than in nested-healthy controls (77.3%vs54.2%).The bacterium contains various virulence factors that act as bacterial super-antigens, and stimulate lamina propria macrophages and local T cells[73].During the infection, inflammatory cytokines such as IL-1, IL-6, IL-8, and TNF-α increase the infiltration of leucocytes, and aggregation of platelets and PMNs into the site of infection.Bacteria cause some events such as platelet activation and endothelial dysfunction by increasing von Willebrand factor[74,75].Chemokine receptors such as E-selectin, Pselectin, and intercellular adhesion molecule 1 damage endothelial vessels by increasing the influx of leukocytes[76].Cannonet al[77] showed that the number of chemokine receptors in CSX patients was higher than that in the control group.Other parameters such as serum fibrinogen level, and white blood cell or platelet count in patients with long-term infection are significantly higher than those in the control group[78,79].Lanzaet al[41] found that IL-1/C-reactive protein levels were higher in CSX patients than in the healthy group, so they identified these as CSX biomarkers.Chronic infection may cause several disorders, such as motility vessel, contraction of small vessels, and eventually endothelial dysfunction, by inducing inflammation and increasing immune responses[80-82].The phenomenon of cross-reaction betweenH.pyloriantigens and autoantigens increases endothelial damage[83].Although CagA antigen is a known virulence factor that is associated with complications such as peptic ulcer disease and gastric cancer, no significant relationship was found between thecagAstatus and CSX disease (OR: 0.97; 0.56-1.70 with 95%CIs).Risk factors such as hypertension, hyperlipidemia, diabetes mellitus, smoking, and alcoholism are among major risk factors for CSX[84,85].In general, inflammatory responses to chronic infections dysregulate the basal metabolism; for example, IL-6 affects the liver and increases gluconeogenesis and synthesis of fatty acids[86-90].Another inflammatory cytokine, TNF-α, reduces the clearance of blood fat particles by blocking liver lipoprotein lipase, thus, it is associated with hyperlipidemia[91-93].Nowadays, there is ample evidence of a positive correlation between chronicH.pyloriinfection and hypertension.In the study conducted by Mignecoet al[94], it was shown that complete eradication of infection with these bacteria significantly reduced hypertension in infected patients[93].Based on previous studies, this bacterium affects the immune system, leading to defects in lipid metabolism and eventually hyperlipidemia[95-98].In general, prolongedH.pyloriinfection leads to extra-gastrointestinal complications such as motility vessel, microvascular constriction, endothelial dysfunction, hypertension, and hyperlipidemia, and at the end CSX (Figure 4).
Limitation
Our meta-analysis had several limitations such as: small number of participants, limited geographical distribution, high heterogeneity, significant publication bias, and lack of adjustment for covariates such as age and CV risk factors, nature of studies (case-control and no cohort), and lack of access to raw data such as socio-economic status, alcohol consumption, and environmental hygiene.However, due to heterogeneity, we need further research to confirm the present findings.
CONCLUSION
The present study was the first comprehensive study to evaluate the relationship betweenH.pyloriinfection and CSX.Overall, our results suggested an association betweenH.pyloriinfection and the risk of CSX; however, we need further research with larger sample sizes to confirm the present findings.In this study, using a systematic review, we showed thatH.pyloriinfection increases the risk of developing the CSX disease through inflammation, endothelial damage, and the effect on related risk factors.
ARTICLE HIGHLIGHTS
Research background
Cardiac syndrome X (CSX) is multilateral condition that not well characterized.
Research motivation
For the first time, we investigated the probable association between Helicobacter pylori(H.pylori) infection and risk of develop to cardiac syndrome.
Research objectives
In the present study, the association between H.pylori infection and CSX was investigated.
Research methods
We searched several databas es to collecting all available documents relevant to impact of H.pylori infection and susceptibility to CSX.odds ratio (OR) is used for estimation of probable link between H.pylori infection and CSX.
Research results
There is a positive association between H.pylori infection and risk of develop to CSX(OR: 5.65, 95%CI: 4.17-7.64, I2: 82.20).
Research conclusions
In this study, we found that H.pylori infection increases the risk of CSX.We showed that there is no significant relationship between cagA status and progression to CSX.The frequency of vascular endothelial destructive risk factors such as hyperlipidemia and hypertension in patients infected with H.pylori was significantly higher than the control group.
Research perspectives
Infectious agents such as H.pylori infection can provide a condition to susceptibility of CSX.
 World Journal of Meta-Analysis2021年2期
World Journal of Meta-Analysis2021年2期
- World Journal of Meta-Analysis的其它文章
- Laboratory hematologic features of COVID-19 associated liver injury:A systematic review
- Therapeutic applications of dental pulp stem cells in regenerating dental, periodontal and oral-related structures
- Nonalcoholic fatty liver disease and cardiovascular concerns: The time for hepatologist and cardiologist close collaboration
- Metabolic and biological changes in children with obesity and diabetes
- Viral hepatitis: A brief introduction, review of management,advances and challenges
- Ankle injuries in athletes: A review of the literature